
Abstract
Objective
Forgetfulness is one of the main reasons of unintentional medication non-adherence. Adherence technologies that help people remember to take their medications on time often do not take into account the context of people’s everyday lives. Existing evidence that highlights the effectiveness of remembering strategies that rely on contextual cues is largely based on research with older adults, and thus it is not clear whether it can be generalized to other populations or used to inform the design of wider adherence technologies that support medication self-management. Understanding how younger populations currently remember medications can inform the design of future adherence technologies that take advantage of existing contextual cues to support remembering.
Methods
We conducted three surveys with a total of over a thousand participants to investigate remembering strategies used by different populations: women who take oral contraception, parents and carers who give antibiotics to their children, and older adults who take medications for chronic conditions.
Results
Regardless of the population or the type of regimen, relying on contextual cues—routine events, locations, and meaningful objects—is a common and often effective strategy; combinations of two or more types of cues are more effective than relying on a single cue.
Conclusions
To effectively support remembering, adherence technologies should help users recognize contextual cues they already have at their disposal and reinforce relevant cues available in their environment. We show that, given the latest developments in technology, such support is already feasible.
Introduction
Despite high adherence being crucial to ensure that medications are effective, 1 adherence rates are low.2–4 Non-adherence can start even before the patient visits a pharmacy: primary non-adherence, a situation where a patient fails to redeem their prescription in the first place, affects an estimated 15% of patients. 5 However, redeeming the prescription is just the first obstacle. Once patients obtain their medications, they may still fail to adhere to their regimen. They may consciously decide to modify or discontinue their treatment (intentional non-adherence) because of side effects, lack of understanding of how the treatment works, their beliefs regarding the necessity of the treatment, and other related concerns.6,7 They can also become non-adherent because of factors beyond their control (unintentional non-adherence), such as the inability to access the medication (e.g. medication unavailable at the local pharmacy), unclear communication with the physician, misunderstanding of the regimen,3,8 or deficiencies in their memory or dexterity. 9 Patients can be non-adherent intentionally and unintentionally to the same medication regimen at different times, 6 and both types of non-adherence can overlap as, for example, people with lower motivation to take their medications are less likely to put effort into developing a reliable remembering strategy and therefore are more likely to forget. 10
In this paper, we focus on forgetfulness, as it is the main reason for unintentional non-adherence and can affect anyone, 11 including those who are motivated and would like to stay adherent. There are several ways in which patients’ memory can fail: they can forget their regimen (e.g. the number of doses, number of pills per dose, taking instructions and drug interactions), forget to take medications on time, forget to pack them when going away or travelling, or forget to order prescription refills. 12 We focus specifically on forgetting to take medications on time, as it can occur even when people have medications with them and remember their regimen. Moreover, such forgetfulness is still prevalent despite the wide access to technologies designed specifically to avoid this problem. While various commercial products exist, from simple smartphone apps to complex medication management systems, and various researchers are working on novel approaches to supporting patients’ memory,13–18 existing adherence technologies seem to neglect people’s actual behavior and the context within which they remember their medications.
When we think about context in terms of technology design, it is more than just a background in which a specific activity takes place: context arises from the activity; it is something that people do. 19 This is especially relevant for understanding forgetfulness, as remembering relies heavily on contextual cues. Remembering to take medications on time is linked with prospective memory, i.e. a set of cognitive processes that regulate the formation, retention, and retrieval of intended actions at a particular point in the future. 20 Based on the type of cue, prospective memory tasks can be divided into time-based tasks, e.g. taking medications at 9am; and event-based tasks, e.g. taking medications with breakfast.20,21 Prospective memory research shows that tasks associated with existing routine events are easier to remember and, 22 by preventing forgetfulness, they can help to maintain higher adherence.3,23 Contextual cues such as preceding actions or surrounding objects also support the process of habit formation, which makes remembering easier in the long-term, as elements of the environment start to drive the behavior and make it automatic.24,25 The benefits of using contextual cues to support memory and behavior have also been noted in medical and nursing literature.26–29 However, what we know about contextual cues rarely underpins the design of adherence technologies.
While several studies have explored the remembering strategies that people develop to support their memory and highlighted the positive role of daily routines and other contextual cues, existing research tends to be limited to the experiences of older adults, mostly those living in care homes or those who need to be supervised.18,29–31 Research on remembering strategies developed by other populations, especially younger adults and those remembering medications for non-chronic conditions or taking preventative measures, is scarce. Even though the studies mentioned earlier provide empirical evidence that contextual cues can support medication management, it is not clear whether their findings can be applied to all populations. Many people believe that older adults do not use technology, 32 and as a result, designers of technologies aimed at younger populations may assume that what we know about contextual cues does not apply here. It is also not clear how contextual cues could be supported by adherence technologies, as the majority of existing solutions—including devices designed with older adults in mind—do not provide that kind of functionality, as we will highlight later. Therefore, exploring how young adults remember their medications and comparing their strategies to those developed by older adults would help us gain a fuller understanding of approaches used by various age groups, and would inform the design of future adherence technologies that take advantage of existing contextual cues and fit into people’s everyday lives.
To achieve that, we present three surveys that explore how over a thousand participants from three different populations remember three distinct medication regimens. We compare strategies developed by women who take oral contraception, representing younger populations, with strategies developed by parents and carers who give antibiotics to their children and by older adults who take medications for chronic conditions. The paper makes two contributions. First, we describe remembering strategies developed by young women taking oral contraception and highlight similarities with approaches reported by other populations. Our results corroborate the data from existing studies and provide a fuller understanding of how people remember their medications in their day-to-day lives, outside adherence interventions. We show that, regardless of the regimen length or the number of daily doses, relying on daily routines, locations and meaningful objects in daily medication management is a common and often effective strategy; in contrast, adherence technologies are rarely used. Second, we argue that to design more effective medication adherence technologies that support remembering and better meet users’ needs, we should take into account current behavior and the cues people already use. As different types of cues require different approaches, we conclude by discussing how technology could support routine events, meaningful locations and objects to enhance existing solutions and help people better remember their medications.
Medication management strategies
Several studies have explored how people remember and manage their medications. For example, an ethnographic study with 10 older adults living within the Danish welfare system showed that for many participants medication management was a personalized behavior that had developed over time and was guided by the physical environment and temporal rhythms of the day. 30 In another study, conducted with 27 chronically ill older adults, 26 participants received electronic medication boxes and were encouraged to keep them in meaningful places where they completed routine actions (e.g. by a coffee pot). The results showed that it was possible to improve adherence rates through tailoring remembering strategies and leaving visible cues in routinely visited places. The location of medications is especially important, as cues that become visible right before the action should be completed are more effective than cues that are constantly visible. 33 Such contextual cues can also support the formation of resilient strategies,34,35 i.e. actions that aim to minimize the chances of making an error or to reduce its consequences. In the context of medication management, resilient strategies can include: always taking medications out the previous evening so they will not be forgotten in the morning, 28 turning over pill bottles to indicate that the medication has been taken, 27 or leaving medications in meaningful places where they would be encountered at the right time.29,30 However, these and many other existing studies focus on older adults and the management of chronic conditions.
Younger populations also take medications and would benefit from technology support; however, relevant research is scarce. For example, even though McGee-Lennon et al. explored remembering strategies of 379 participants including different age groups (13% were 18–30 years old and 46% 31–60 years old), 18 their focus was on designing assistive technologies for people with memory issues: they included younger populations to understand their preference for assistive technologies they may need in the future. When the focus is specifically on young populations and their current needs, research is seldom concerned with their existing behavior. For example, while several studies have been conducted to investigate how women remember oral contraceptive pills and the reasons for their non-adherence,36–39 or how specific action plans (e.g. “When I put my mascara on, I will take my Pill from my make-up bag”) could support adherence, 40 none of them investigated existing remembering strategies developed by women outside the intervention or without prompts from the clinicians. Neither did they look at technologies that support remembering: while studies like Hou et al.’s evaluated the impact of a specific technology during an intervention aiming to increase the adherence to the Pill regimen, 41 at the time of writing there were no studies that evaluated the technologies selected by women themselves. The situation is even worse regarding remembering short-term regimens such as antibiotics. Even though 50–90% of patients make unintentional errors while taking antibiotics, 42 and the omission of single doses is the most common mistake, 43 there are no studies that explore what strategies people develop to remember antibiotics and what cues are the most effective.
Adherence technologies
Adherence technologies available to patients vary from simple smartphone apps to smart devices and complex medication management systems. Even though they come in different shapes and sizes, they largely tend to ignore users’ existing behavior and related contextual cues. In this section we describe the main groups of devices to highlight their limitations.
Smartphone apps are the most common solutions, easily available to anyone with a smartphone. They are also the simplest. For example, a review of 229 existing medication reminder apps shows that they focus on reminding and do not provide functions that support routine behavior. 44 Moreover, in most cases, they do not differ much from default smartphone alarm clocks; in some cases, they provide even more limited functionality, as unlike alarm clocks they often do not allow users to postpone the reminder. 44 A review of 32 dedicated contraception reminder apps 45 shows a similar trend: while the apps primarily provide notifications, less than half allow users to snooze the reminder; features designed to support the habitual nature of oral contraception regimes are not available.
Other, more sophisticated types of commercial adherence technologies are also available. For example, complex medication systems such as PivoTell Automatic Pill Dispenser or Philips Medication Dispensing Service are designed specifically for patients who manage multiple medications.46,47 They can hold over a month’s supply of medications and dispense them when necessary, freeing the patient from the burden of remembering when and which medications to take. However, they are big and stationary, which requires users to be nearby when their next dose is due. While this might not be a problem for older adults who often lead highly organized lives, 48 this type of adherence support may not be practical for other populations. Augmented medication containers are a simpler solution. For example, GlowCaps are a set of interactive medication box caps, 49 and GlowPack is a pouch that can hold inhalers, injections, or blister packs; 50 both are paired up with an alert light that can be plugged into a power outlet anywhere in the house. These products are rare examples of technologies that could support existing routines, although it is not clear whether they have been tested with users.
Academic researchers have also been exploring how technology could better support patients, mainly older adults with chronic conditions. For example, MoviPill allows users to track their doses and awards them with points visible on a companion app; 13 the focus is on keeping people motivated. DwellSense shows usage statistics and missed doses on an ambient display, 14 also focusing on motivation. Colorado Tablet allows older users and their carers to track doses, check medication information, and prepare for doctor visits. 16 None of them explicitly supports the use of contextual cues. The closest to supporting daily routines are ambient information systems that display the number of doses already taken directly on medication containers and thus could be used without changing users’ existing behavior.15,51 However, while the early evaluation suggests that it might be effective, the system is a prototype and, apart from a small feasibility study, 52 has not been tested with users. Other systems devised by researchers do not differ much from commercially available apps. For example, MediFrame is a tablet app with a built in calendar that allows users to plan their medication intake while considering scheduled activities (work, leisure), retrieve information about their medications (side effects, drug interactions, etc.), set reminders, contact GP, and record medications taken as-needed. 17
The above examples are just some of the available solutions, but they illustrate the fact that overall, technologies are designed to provide alerts that actively remind users about medications or aim to keep them motivated. While some of them could be used as visual cues (e.g. complex medication management systems placed in a meaningful place), they hardly ever explicitly support users’ daily routines or other types of contextual cues.
In the next section we describe our research conducted to understand how people remember medications and how technology could support their existing behavior and fit into their everyday lives. As studies exploring medication management strategies tend to focus on older populations, it can be difficult to generalize the findings. Therefore, to gain a fuller understanding of the role of contextual cues in remembering strategies developed by younger adults, we present three surveys that provide a detailed overview of remembering strategies developed by over a thousand mostly young and tech-savvy people. Our research explores how they remember their medications, what role contextual cues play in that process, and what types of cues effective remembering strategies have in common across regimens.
Understanding remembering strategies
Existing research suggests that relying on daily routines and other contextual cues can be an effective remembering strategy that supports medication management. Based on existing literature and research conducted with older adults, we hypothesized that regardless of the complexity (e.g. number of doses) or length of a regimen, more people would rely on contextual cues than on technology to help them remember their medications (Hypothesis 1, H1), and that it would be an effective strategy (Hypothesis 2, H2). We also wanted to find out what cues effective remembering strategies have in common (Research Question, RQ) and thus what types of cues should be supported by adherence technologies. To test the above hypotheses and answer the research question, participants representing three regimens of varying length and complexity were selected:
Women taking oral contraception, representing a long-term, single-medication, single-dose regimen; Parents whose children take antibiotics, representing short-term, single-medication, multi-dose regimen; Older adults taking medications for chronic conditions, representing long-term, multi-medication, multi-dose regimen.
Focusing on oral contraception (“the Pill”) allowed us to reach a large number of participants and enabled us to gather remembering strategies from a younger population that is also likely to use technology (90% of 16–24 year olds in the UK own a smartphone and women aged 20–24 are the most likely to take oral contraception).53,54 The additional data from parents and older adults complemented the findings and allowed comparisons across distinct regimens, and helped to deepen the understanding of the role of contextual cues and the use of existing technologies in medication management. As in all surveys we used the same questions with minor modifications to match regimen of each participant group, we provide a combined method section, but report findings separately.
The preliminary results of Survey I were summarized in our previous paper, 44 where we highlighted the role of routines and the lack of technology use among young women to motivate our review of medication adherence reminders and their customer reviews; the details of their remembering strategies and information about cues other than daily routines have not been published before. Similarly, preliminary results of Survey III, limited to information about reasons for forgetting and main groups of cues (daily routines, medications as reminders, and alerts), were used to motivate the design of an ambient medication reminder system; 52 detailed information about cues and rates of forgetting are reported here for the first time. Survey II and the combined analysis of remembering strategies developed by participants who reported not missing doses have not been published before.
Method
Participants
Information about 1146 participants who initially completed the surveys.

Procedure
To reach women taking oral contraception and parents whose children take antibiotics, online surveys were distributed through a mailing list among staff and students at a large university in the UK, and were advertised on social networks. The antibiotics survey was also advertised via leaflets distributed in nurseries and primary schools in south London, UK. Both groups of participants were offered a chance to enter a raffle to win one of three £25 Amazon vouchers. Survey III was conducted in Mexicali, Mexico. Participants were recruited by contacting relatives and friends, and by visiting local public centers that provide older adults with healthcare and social services, with which the second author made an a priori collaboration agreement. Participants were approached face-to-face, with interviewers filling in the survey on a tablet computer; they were not offered any incentives for participation.
Materials
An online questionnaire was used to collect the data. We used the same questions, with small modifications made to reflect different regimens (the version used in Survey I is available in the Appendix). The first page included informed consent form and only those participants who agreed to participate were able to proceed. The surveys consisted of two main parts. The first part included 18 questions that investigated how respondents remembered their medications, and how often and why they forgot. The key questions that we used to analyze remembering strategies provided pre-defined answers that were informed by existing research, but participants could also add free text answers; multiple answers were allowed. The second part included the standardized 16-item self-report Prospective and Retrospective Memory Questionnaire (PRMQ) that includes an 8-item subscale for assessing prospective remembering and an 8-item subscale for assessing retrospective memory. 55 PRMQ was selected as it is the most widely used instrument for assessing prospective memory through self-reports that has been validated and used in other studies. 56 PRMQ scores were later used to eliminate participants with memory issues or those with exceptional prospective memory who could skew the results. Survey III questions were translated into Spanish and a validated Spanish version of PRMQ was used. 57 We also collected general demographic information and regimen details (see Table 1).
Analysis
The analysis was conducted in two stages (see Figure 1). First, PRMQ scores were calculated and compared with the control group,
55
and participants whose scores fell outside two standard deviations from the control group’s score were excluded from the analyses reported below (42 participants from Survey I, five from Survey II and six from Survey III). Data of 1093 participants were used to test H1 and H2. We used descriptive statistics to analyze the main trends and to understand types of cues participants used, and Chi-square tests for independence to calculate differences in the effectiveness of daily routines and technology used by participants.
Stages of analysis, showing the total number of participants and the number of participants in each study.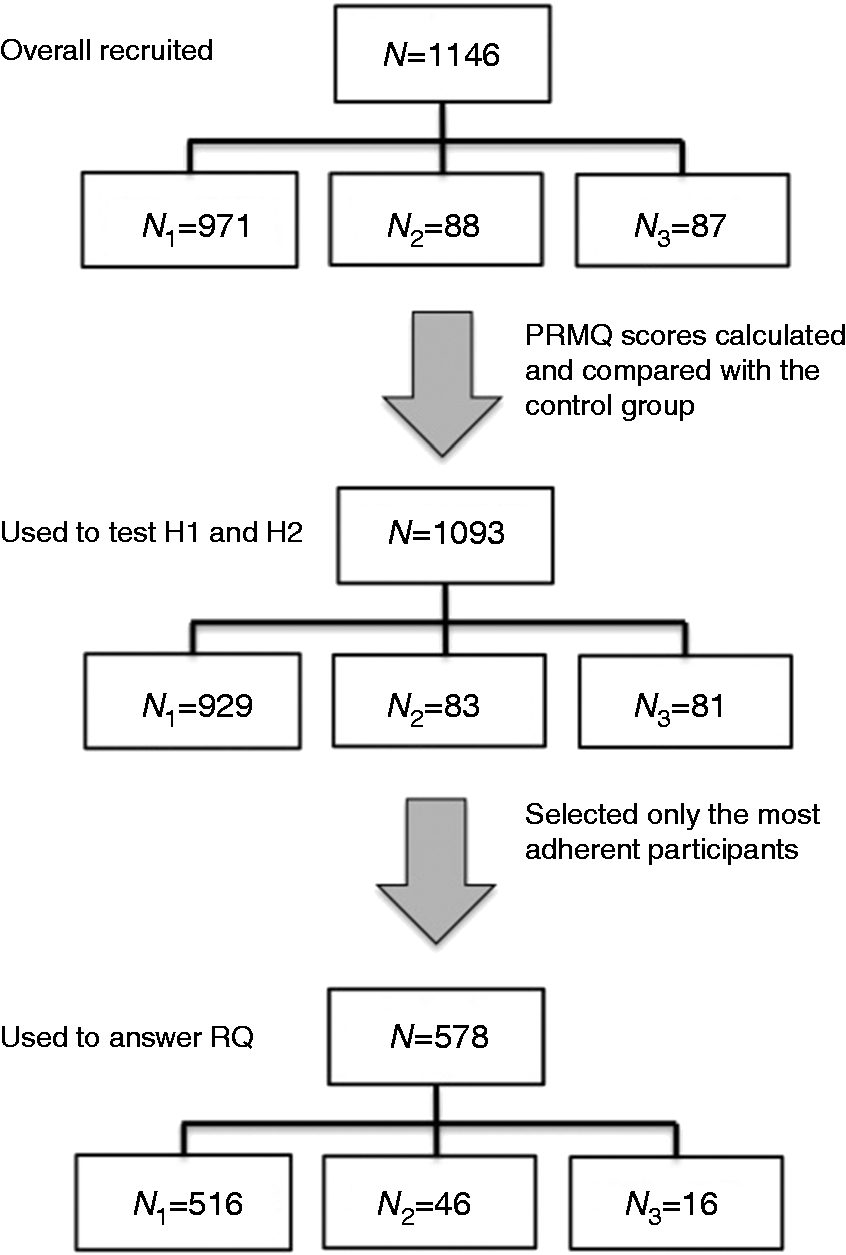
The format of a question investigating remembering strategies (“What do you use to help you remember to take your pills?”; see Appendix) differed between the surveys to match the data collection method: in Survey I and II it was a multiple answers question, but in Survey III it was open-ended. The first author and two researchers not involved in this research independently matched the open-ended answers with survey categories. For 75 entries (86%) all raters were in agreement. For 11 entries (13%), 2 out of 3 raters were in agreement, and their answers were used. In one case there was no agreement between the raters and the best category was selected after a discussion (“a clock” was filed under “Other” as it wasn’t clear whether the participant meant paying attention to actual time or used reminders).
Next, to answer the RQ, details of the most adherent participants were extracted. We selected the responses of 578 participants who reported that they did not forget their medications at all during the month preceding the online surveys (516 women taking oral contraception and 46 older adults) or who reported that they did not forget any doses last time their children took antibiotics (16 parents). For each participant, we noted the following information: medication location, time they took them, reported remembering strategies and additional free text comments they provided. To understand what safeguards they used to avoid forgetting, their strategies were also matched with corresponding resilient strategies. 34
Findings
Summary of remembering strategies and forgetfulness information for all participants.
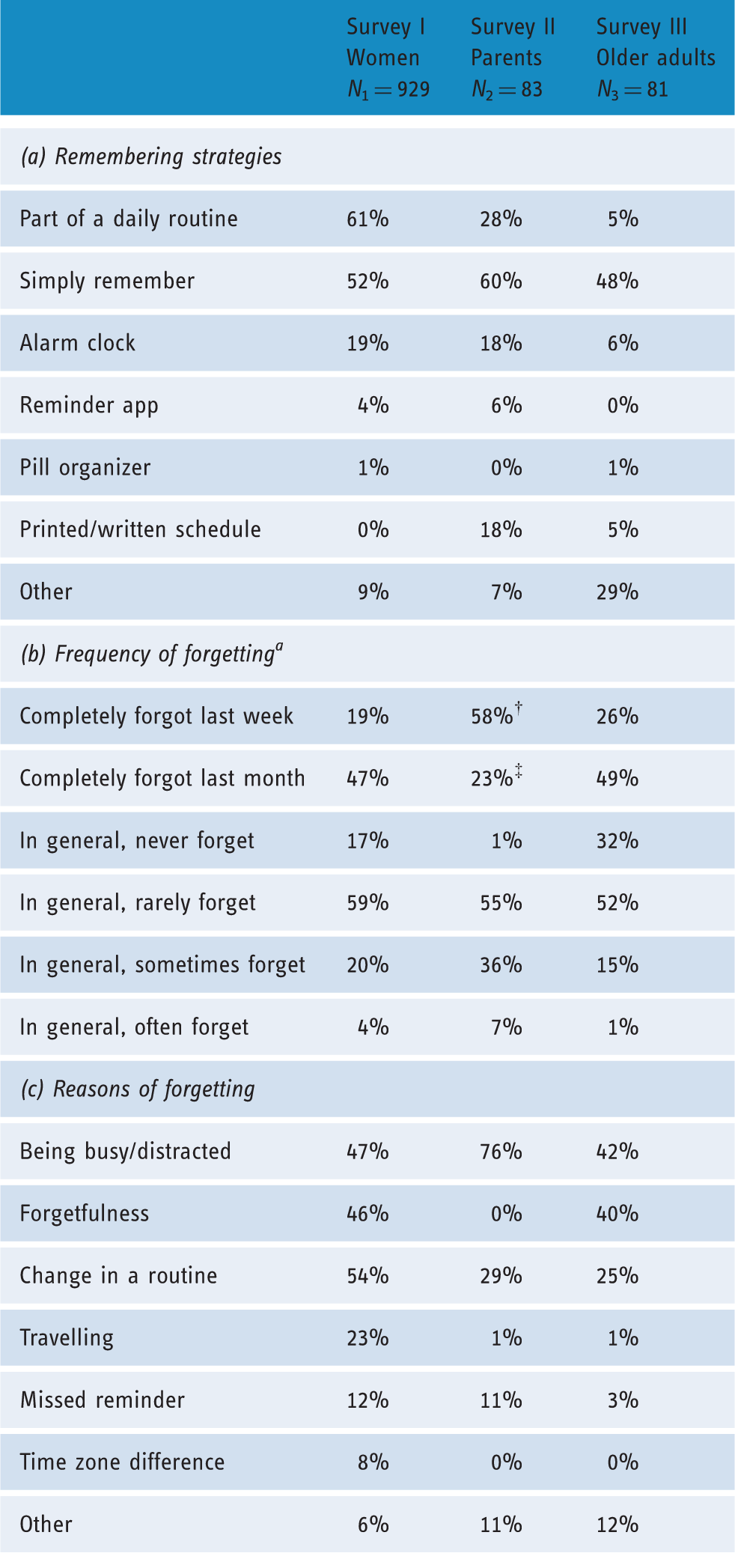
Figures for antibiotics refer to the last time respondents’ children took antibiotics. Instead of rates for last week we show the percentage of parents who forgot 1–2 doses (indicated with a dagger †) and instead of rates for the past month we show the percentage of parents who forgot 3 or more doses (indicated with a double dagger ‡).
Survey I: oral contraception. Long-term, single-dose regimen
Responses from 929 participants was analyzed. When asked what helped them remember (see Table 2(a)), the majority of respondents reported relying on daily routines or said they simply “tried to remember”. They tended not to use technology to remind them about the Pill, and if they did, they more often reported using alarm clocks than dedicated apps. A quarter (24%) of women who used some sort of technology (N = 210) also said that Pill-taking was a part of their routine. Their remembering strategies were often linked with routine events such as waking up (33%), going to sleep (28%) or eating breakfast (6%). They also reported keeping their pills by the bed (52%), in a handbag or a purse (19%), in the bathroom (10%), or in a make-up bag (6%); the location (e.g. bathroom) and associated items (e.g. a purse) provided additional cues. However, they still forgot (see Table 2(b)). When asked about the month preceding the survey, the majority reported taking the Pill later than they should and nearly a half reported completely forgetting to take it that day. Participants reported changes in the daily routine, including anticipated disruptions such as travelling, as the main reasons of forgetting; being busy or distracted, general forgetfulness and missed reminders were also blamed (see Table 2(c)).
Chi-square tests for independence were conducted to investigate how effective relying on routines was. The results showed that women for whom Pill-taking was a part of a daily routine (N = 565) reported forgetting less often than women who did not rely on routines (N = 364); the results were statistically significant for both forgetting during the past week (χ2(1,929) =23.8, p < .001, phi = −.16) and the past month (χ2(1,929) = 17.1, p < .001, phi = −.14). A similar analysis was conducted to compare women who reported using apps or alarm clocks (N = 210) with those who did not use any technology-based memory aids (N = 719); the results were not statistically significant (χ2(1,929) = 1.54, p = .215, phi = .044 for forgetting during the past week and χ2(1,929) = .09, p = .76, phi = .013 for forgetting during the past month), suggesting that the presence of technology did not provide any benefits.
Survey II: antibiotics. Short-term, multi-dose regimen
Responses from 83 participants were analyzed. When asked about specific remembering strategies, the majority reported that they simply “tried to remember” and therefore did not use any memory aids (see Table 2(a)). However, they still relied on contextual cues: they reported keeping antibiotics in the kitchen (84%), most often inside the fridge or a kitchen cabinet (74%); 12% reported keeping antibiotics in a visible place. For a quarter of participants, remembering antibiotics was a part of their daily routine, and a similar number reported using some sort of technology to support their memory, usually their mobile phone’s alarm clock. A third of respondents (33%) also said their children were involved in remembering. Over a half of participants reported missing 1–2 doses (reported in Table 2(b) in the rows for forgetting last week/month, see table footnotes for clarification), mostly due to being busy and distracted (see Table 2(c)). 11% of participants also mentioned issues related to childcare as causes of forgetting, e.g. the child being asleep when the dose was due, leaving medications at the nursery, or issues with synchronizing antibiotics with meals.
Nearly half of respondents (43%) said that fitting antibiotics into their daily routine was difficult or very difficult, mainly because of too many daily doses and having to care for more than one child. The age of the child was also a factor, as it is difficult to manage evenly spaced doses when the child is young and parents have to follow a specific daily routine that may not be compatible with the regimen. In a few cases respondents reported difficulties with managing antibiotics when multiple people and locations were involved (e.g. home and nursery), as it was harder to remember when the last dose was administered and who was responsible for the next one.
A Chi-square test for independence was conducted to investigate the associations between the presence of a routine and missed doses. Participants who reported relying on routines (N = 23) also reported forgetting less often than other participants (N = 60), although the result was not significant (χ2(1,83) = .34, p = .56, phi = .09). Another Chi-square test was conducted to investigate the associations between the use of technology and incidents of forgetting, and while generally respondents who reported using technology (N = 20) forgot less often, the result was also not statistically significant (χ2(1,83) =1.14, p = .29, phi = −.15). As the majority of participants were women (80%), we conducted the same analyses to investigate whether there were any gender differences in selected strategies or incidents of forgetting; the results were not statistically significant.
Survey III: older adults. Long-term, multi-dose regimen
Responses from 81 participants were analyzed. They reported taking their medications before sleep (57%), in the morning after waking up (48%) or with meals (27% of participants took their medication after breakfast and 31% after lunch); for 82% the time was prescribed by their doctor. 46% of participants reported keeping their medications by the bed and 43% in the kitchen (22% in a cabinet and 21% on a table). In addition, 24% of participants reported keeping them in a bag or a wallet. Overall, 69% of respondents reported relying only on routine events, 20% combined routine actions with specific time and 12% took their medications at a specific hour. However, when asked directly about what helped them remember, only 5% explicitly mentioned routines (see Table 2(a)). Forty-two participants (48%) reported that they did not use anything to help them remember, even though they kept medications in places that made remembering easier (e.g. by the bed, in the kitchen) or took them in conjunction with routine events (e.g. before going to sleep, after waking up). Only five participants reported using alarm clocks as reminders.
The majority of participants reported that they did not forget their medications at all during the week or the month preceding the survey. A half of participants reported that overall they rarely forgot and a third said they never forgot (see Table 2(b)). When asked about main reasons for forgetting, they reported being busy and distracted, simple forgetfulness, and changes in the routine (see Table 2(c)).
To explore the relationship between remembering strategies and forgetfulness, participants were divided into those who reported relying on routines or keeping medications in visible places (N = 17) and those who reported using other strategies (N = 64). The result of Chi-square test for independence was not statistically significant for instances of forgetting in the past week (χ2(1,81) = 1.69, p = .19, phi = .18) or in the past month (χ2(1,81) = .364, p = .55, phi = .097), indicating that the presence of contextual cues did not make any difference. Given that the majority of participants reported not using anything to help them remember (N = 42), we conducted another Chi-square test to compare them to the rest of participants (N = 39). The results were not statistically significant for forgetting in the past week (χ2(1,81) = 1.47, p = .23, phi = .163), but were significant for the past month (χ2(1,81) = 5.43, p = .02, phi = .28), indicating that participants who reported not using any cues forgot less often. However, even though they said they did not use any memory aids, answers to other questions showed that they did take medications in response to routine events or used other contextual cues. Even though the majority of participants were women (79%), we did not discover any gender differences: the results of analyses exploring differences in selected strategies or incidents of forgetting were not statistically significant.
Characteristics of effective strategies
The analysis of responses of participants who reported not missing any doses showed that they took their medications in response to routine actions (e.g. waking up, eating meals, brushing teeth; 88% of respondents), kept them in meaningful locations related to these actions (e.g. by the bed, on the kitchen table; 78%) and relied on visual cues (e.g. kept medications in a visible or meaningful spot, used pill organizers; 66%). Over half of participants (55%) reported using all three types of cues and a further 25% used a combination of two; 8% of participants reported relying only on routines and did not specify any other types of cues. Only 6% of participants (35 women from Survey I) reported using technology-based reminders as their sole remembering strategy and did not mention any other types of cues. A quarter (25%) of participants reported using reminders in conjunction with other types of cues (13% with daily routine events and 12% with objects), although most of them specified that they used reminders “just in case”.
In terms of resilient strategies, the most common was cue creation: 66% of participants created cues by leaving medications in a visible spot (e.g. on a bedside table) or in a place related to their routine (e.g. inside a make-up box). Over a quarter (27%) used reinforcement (defined as reinforcing safety barriers, procedures or practice): even though they used visual cues or routines, they also used other safeguards such as technology-based reminders or relied on other people (partners, children) to remind them about medications. Another common strategy was managing resource availability (defined as taking action to ensure that necessary resources are available when needed): 21% of participants reported keeping their pills in a wallet, bag or purse—somewhere where they would be at hand if they forgot to take them at the usual time. Three participants also modified their daily routines to allow for checks whether they have already taken the medication (routine adjustment). Overall, 27% used more than one strategy, often combining cue creation with reinforcement.
Discussion
Our research presented above investigated remembering strategies developed by participants from different populations to remember different regimens. Oral contraception was used as an example of a single-dose long-term regimen; antibiotics were used to represent short-term, multi-dose regimen; and older adults represented patients with multi-medication, multi-dose regimens. The aim was to understand what types of cues are a part of effective remembering strategies (RQ); and to test the hypotheses that regardless of the complexity of a regimen more people would rely on contextual cues than on technology (H1), and that this would be a more effective strategy (H2). We also wanted to corroborate the data from existing studies focusing on older adults and to establish whether there are similarities in approaches to medication management across different populations.
The results supported H1. Regardless of the type of regimen, participants tended not to use technology and primarily relied on everyday routines, physical objects used as visual cues and the location of their medications. This is in line with previous studies conducted with older adults;26–30 we show that this is true for all age groups. This reliance on contextual cues was especially prominent among the subset of people who reported not forgetting: their effective remembering strategies were characterized by a combination of two or more types of cues. Their strategies also hardly ever involved the use of technology. If technology was used, it was only as an additional safeguard that reinforced other cues. However, there were small differences in the use of these cues across regimens.
Results of the oral contraception survey showed that relying on a daily routine was an effective remembering strategy. Women who took the Pill in response to existing events (e.g. right after waking up), and who kept it in visible (e.g. by the bed) or in meaningful places (e.g. in a handbag or a purse) forgot less often than other participants. The small number of participants using apps came as a surprise: given their age, they were the most likely to own a smartphone and install apps. 53 The majority of those who did use technology preferred alarm clocks to dedicated reminder apps and often used them together with other cues, mostly as a back-up. Given that reminders seemed to make no difference in preventing forgetfulness and that reminder apps in general do not support daily routines,44,45 relying on other cues is a rational strategy supported by existing research. 23
Parents and carers also reported relying on routine events, even though the course of antibiotics is too short to be turned into a routine in itself (the standard length of an antibiotics treatment is 7–10 days). 58 As a result, most of them “simply tried to remember” or used existing routine events as triggers to action. In addition, while antibiotics were not always visible, they were kept in places where they still could serve as visual cues, e.g. in the fridge, even if that visibility was not intentional. This is a reasonable approach, as cues that become visible at the right time (e.g. opening the fridge and seeing antibiotics that need to be taken with meals) are more effective than cues that are visible all the time. 33 Even though we expected parents to use technology, mainly due to complexity of an antibiotics regimen and difficulties with remembering multiple daily doses, 43 it was not the case. Perhaps parents did not see the benefits of reminders (relying on them was not associated with reduced rates of forgetting) or setting up reminders that match the regimen was not possible (a third of medication reminders for smartphones impose limitations on alert scheduling 44 ).
The lack of technology use among older adults was not surprising as only 0.7% of older adults in Mexico used a smartphone and 17% used a tablet computer in 2014. 59 Moreover, this result is supported by the data from McGee-Lennon et al., 18 who discovered that older adults were significantly less likely to rely on reminders compared to younger populations. In line with the existing research, our participants reported relying on daily routines and keeping medications in a visible place.29–31,60 However, the majority of them did not see themselves as using any cues at all: their medication management strategies were so ingrained in their daily lives that they often did not recognize them as such. The way they planned when to take their medications and where to keep them provided prompts to action, and in their mind they simply remembered on their own. Such ingrained reliance on contextual cues has also been observed in previous studies. 29 It could be explained by a more structured daily life of older adults, who tend to have higher levels of temporal organization compared to other age groups, 48 although people in general may not recognize the cues that prompt their behavior. 61 This also suggests that they might have developed a habit and their behavior became automatic, which would explain the lack of awareness of what cues were prompting them. 62
As reliance on contextual cues makes it easier to remember,3,23 helps to develop a habit over time,24,25 and minimizes occurrences of memory lapses, 63 we expected that our data would support H2. However, it turned out to be true only for women taking oral contraception, possibly due to differences in sample sizes. Even though the trend was the same for parents and older adults (those who reported that taking medications was a part of their routine forgot less often than those who did not mention routines), the differences were not statistically significant. However, while routines were generally associated with a reduced number of incidents of forgetting, they were not perfect: participants still forgot and changes in their routine were the main cause of missed doses, which has been reported previously. 29 This illustrates the vulnerability of routine behavior and also its heavy reliance on the context and the environment.64,65 The analysis of effective strategies confirms it: participants who reported not missing any doses also often reported relying on daily routines that were linked with other contextual cues. This highlights an opportunity for adherence technologies that could provide the support to multiple contextual cues that are already in use.
Supporting cues with technology
Only a small proportion of participants reported using technology to support their medication management, with the majority using alarm clocks. Not all patients see a need for adherence technologies because their own strategies provide enough support,
66
and indeed, our participants mostly relied on contextual cues. However, while the cues played an important role in supporting each regimen, that role differed. For women taking oral contraception, the act of taking the Pill was a routine in itself. For older adults, medications were so ingrained in their lives, that they often did not realize what helped them remember, which suggests the behavior was a habit. Parents and carers administering antibiotics to their children primarily relied on the placement of medications. Despite these differences, all regimens were linked to the same types of contextual cues that support self-management of medications:
They all took medications in conjunction with routine tasks, e.g. taking them after waking-up, with meals, or before going to sleep; They took or kept them in meaningful locations, often related to the routine, e.g. on the bedside table, inside a bag, or in the fridge; and They used objects associated with medications as visual cues, e.g. pill organizers, make-up bags, or medications themselves.
Routine tasks, locations and objects were often connected and it was not always possible to separate them. Combinations of cues were often further reinforced by resilient strategies such as additional back-up reminders or keeping pills in a bag, so they would always be at hand. This echoes Dourish’s notion of context as something that “people do”: context and activity cannot be separated. 19 For example, keeping medications on the bedside table and taking them every morning is a combination of an object, routine and location. Taking pills with breakfast combines a routine with location. However, existing adherence technologies do not seem to be designed to work within this context and do not make use of existing cues. In the next section, we discuss how technology could work with each type of cue and provide more robust adherence support by helping people fit medication-taking into their everyday life.
Supporting daily routines
Almost all participants took their medications in response to a routine event: waking up, eating meals, getting ready to sleep, etc. This is a common approach already reported in literature.29–31 Rather than simply providing reminders, adherence technologies could take advantage of that existing behavior by helping users identify existing routine events that are unique and associated with medications, and reinforcing the connections with them.
Technology could help users recognize contextual cues already linked with their medications by facilitating reflection on their daily habits. For example, some of our participants reported that they did not use any memory aids and “simply tried to remember” while in fact they took their medications with meals or after waking up and kept medications near the bed. While it can be difficult to reflect on triggers to action when the behavior is a habit 62 —as might have been the case for our participants, especially those from Survey III—asking users to clarify where they keep medications and what happens before they take them would increase their awareness of cues they rely on, making them more salient, 67 and could protect against forgetting caused by mindless, automatic behavior. 62 Similar type of support was provided in MediFrame, 17 where users were able see their scheduled routines on a calendar interface. However, technology needs to go further and support routines in a more active way. Reminders could help to reinforce the connection between medications and their cues,44,68 and there is already evidence that such “plan reminders” are effective at supporting health-related behavior change interventions,69–71 which suggests they could also work with medication-taking. By reminding users of their plans to action, i.e. the task with its cue (e.g. “Remember to take your pill with breakfast”), technology would enable them to reinterpret their daily routine (e.g. “eat breakfast, take medications”) as a single task routine (“take medications with breakfast”), making it easier to remember. Several technologies have been proposed that make patients aware of their medication compliance by using either abstract representations such as virtual adherence scores shown in an app, e.g. as in MoviPill, 13 or explicit representations such as ambient displays, e.g. like DwellSense. 14 To support contextual cues, such technologies would have to allow their users to monitor the accomplishment of the reinterpreted medication routine, i.e. not only indicating whether they took medications or not (“medication taken”), but whether they took it along with the task acting as a cue (“medication taken with breakfast”). Linking medications with a cue in that manner would help people with a long-term regimen to turn the medication routine into a habit, and help those with a short-term regimen to remember how they should enact their task-based medication routine. In both cases, it would emphasize routine events and allow users to take advantage of them.
While routine support is important, adherence technologies should also focus on other types of cues. Even though routine actions can support habit formation in the long-term, they may not be enough to effectively support prospective memory when the behavior is still new. 68 Thus, other types of cues are needed: meaningful location can strengthen the routine and meaningful objects can provide visual cues, and overall, combinations of cues can provide extra support and support remembering when the routine changes.
Supporting meaningful locations
The majority of participants reported keeping their medications at home. However, the location alone was seldom the main cue reported by participants, and it was often linked with a routine (e.g. antibiotics in the fridge to be taken after dinner) or an object (e.g. a pill organizer on a nightstand in the bedroom), which made it more meaningful. Moreover, it was often very specific: “bedside table” instead of “the bedroom”, “fridge door” instead of “the kitchen”, etc. Technology could help people identify and select the best location when the cues would be the most likely to be encountered at the right time,18,26,29 and further emphasize these connections.
As people may not be aware of the cues that guide their behavior, 61 technology could provide necessary support. By facilitating reflection over one’s own daily behavior, technology could help people find a spot that makes forgetting medications the least likely. For example, some women reported keeping their contraceptive pills in a make-up bag, because they knew they would see them there every day. Adherence technologies could give suggestions or ask specific questions regarding the location: Do you visit the location every day? Is it unique? Can you notice the medications there even when you are in a rush? In the make-up bag example, such questions would encourage women to think whether they put make-up on every day, and think of situations when their routine changes and the potential consequences of such a change. Once the location was selected, technology could provide location support by asking users to fill in fields that will appear in a reminder in a way similar to that mentioned earlier in regards to recognizing existing routine events.
Location-aware medication containers could help to detect whether a person is near them. As cues that become active at the right moment are more effective than cues visible at all times, 33 the adherence system could provide reminder prompts only when users are near their medications. Alternatively, it could activate when the person is in the right location but it is already past their usual medication time. The ambient display presented by Lee and Dey in a way provided that kind of support. 14 However, once the display was removed, adherence returned to pre-intervention levels; the main visual cue was gone. Thus, the support system should not be visible at all times. Instead, users could be notified only when their routine changes or if they are not in their usual location. This echoes recommendations for effective reminders that specify the need for contextualization and highlight the need for sophisticated planning algorithms. 18 However, allowing users to specify where and when they should be reminded if they do not take their medications at the usual time could also provide such support.
Supporting everyday objects
Objects associated with medications or related routines frequently provided visual cues. Palen and Aaløkke suggest that medication management systems could be distributed across the home and be based on existing physical objects that are digitally supported. 30 As we have shown earlier, researchers have already started to investigate augmented pill organizers and commercial products like GlowPack or GlowCaps are available to the public. The latter in particular have potential to support existing remembering strategies, as they could be integrated within the routine as meaningful objects that provide an additional notification light when a user misses or is about to miss a dose. However, augmentation should not be limited to notifications.
Some participants already reported setting up back-up reminders on their phone—augmented objects could also provide that type of functionality. For example, women who reported keeping contraceptive pills in a make-up bag would benefit if the bag was augmented with sensors: it could get their attention on the days when they decided not to put make-up on. GlowPack already provides similar support, but its notification light needs to be plugged into a power socket; the bag itself does not provide reminders. 50 This type of support would allow users to carry on their routines and would not require a change in a behavior that already helps them remember. As objects used by participants were often linked with locations, smart medication boxes could provide notifications only when they are moved to a new location, e.g. to remind about medications when on holidays.
Supporting medications in context
Designers tend to understand context as a physical environment in which the system is being used and as concurrent activities with which users are engaged at the time. 72 However, the support for the whole context in which medication-taking takes place—routines, locations, and objects—is often missing from currently available adherence technologies. Our work shows that remembering strategies used by older adults are also shared by younger populations; thus, adherence technologies aimed at all populations should take into account daily routines and contextual cues. As our findings are based on a large sample, we offer a richer understanding of what types of contextual cues are used to support memory during medication self-management. We provide evidence that effective strategies are made of multiple cues that describe the context of use: medications are often linked with daily routines that involve the use of specific objects that are kept in meaningful places; single cues are often not robust enough to reliably support memory. Rather than remembering for the users and only providing reminders, adherence technologies should support the cues people already use. To illustrate how this could be done, we have provided several suggestions for designing better adherence technologies that take advantage of the immediate environment and support existing behaviors.
Limitations and future work
Our research has a few limitations linked to its international nature and the characteristics of the target populations. The data was collected in the UK and Mexico, which could be a source of potential confounds due to setting differences, including different healthcare system and medication policies, higher illiteracy of older adults in Mexico, etc. However, given our research question and hypotheses, we welcomed such differences, as we were interested in remembering strategies in different contexts. Reported cues and strategies turned out to be similar despite these differences.
Unlike Surveys I and II, Survey III was conducted face-to-face. Changing the format allowed us to gather responses from older adults. This might have had an impact on some responses, as participants might not have wanted to admit they were non-adherent. However, patients perceive forgetfulness as more socially acceptable than admitting intentional non-adherence and may report it instead,11,73 and thus the forgetting rates they reported are likely to be accurate. The change of format also resulted in changing the remembering strategies question into an open-ended one in Survey III. While remembering strategies in general were similar and we were able to easily map open-ended answers onto the pre-defined categories from Survey I and II, we noticed a difference in the number of people who reported relying on routines. As routines were explicitly mentioned on the list of potential remembering strategies, Survey I and II participants might have selected them because they were prompted to think about them. Survey III participants were not given that prompt and instead provided specific strategies. However, as we also asked about the wider context and did not just focus on strategies directly reported by participants, we believe the findings are still valid.
Sample sizes of our surveys varied due to the characteristics of target populations and their regimens. Moreover, we intended the Survey I population to be the biggest, as we were interested in exploring remembering strategies of younger adults. Nevertheless, with a total of over a thousand participants and similar cues reported across all surveys, we believe that this provides a reliable overview of medication management behaviors that are in line with the prospective memory literature and previous research.
Most of our participants were women. This was inherent to the design of Survey I. The gender imbalance of other surveys could be explained by the fact that women tend to be primary carers (Survey II) and on average live longer than men (Survey III). Nevertheless, further research focusing on remembering strategies developed by men would be beneficial, as gender (and other intra-personal factors) can influence adherence. 1 In this case, however, we did not observe gender differences in remembering strategies developed by our participants; both men and women reported using the same types of contextual cues.
Apart from the three types of contextual cues we described here, the literature and previous studies identify a fourth contextual factor: carers and family members who support medication management. This is especially important for chronically ill older adults, who frequently rely on their spouses and close relatives. 74 Moreover, there is evidence that being a part of a cohesive family and living with another person increases adherence. 75 However, given that this trend was not prominent in our findings (only 14 participants mentioned other people), a discussion on the relationship between contextual cues and other people involved in medication management is out of scope. Nevertheless, future work could explore how contextual cues could be used to support collaborative remembering.
Despite the limitations, our findings support and complement existing research on remembering strategies developed by older adults, and provide a better understanding of how younger people remember other types of regimens and use adherence technologies. The findings help to understand what cues are frequently associated with medications when one has to remember medications on their own, and how we could support them with technology. As currently available adherence technologies are insufficient in this regard, we have discussed how technology could take advantage of each type of cue.
Our future work will focus on understanding how people form remembering strategies and choose their cues in the first place: how they decide where to keep their medications, and why; at what times of day to take them, and why; whether they change and adjust existing cues; and whether they use technology. Understanding this selection process would allow us to design better adherence technologies that help users link medication management with reliable daily routines guided by relevant contextual cues.
Conclusions
We have presented a survey-based research that explored medication management strategies of three distinct regimens. Our goal was to address the gap in understanding of how different populations, especially under-researched younger adults, remember their medications and whether the rich body of research on remembering strategies of older adults could be reliably used to inform the design of adherence technologies built with other populations in mind. This paper makes two contributions that are of interest to researchers working with adherence technologies. First, based on the responses of over a thousand participants, our findings corroborate existing research and provide an overview of contextual cues commonly used across different regimens and populations. Regardless of the population or a regimen type, people tend not to use technology and the effective remembering strategies they use are made up of two or more types of contextual cues: routine events, physical objects serving as visual cues, and meaningful locations. Second, we have discussed how adherence technologies could support each type of cue, and highlighted the fact that such support is already feasible. By ensuring that all types of cues are taken into account, we can design adherence technologies that support users’ memory without requiring them to change their everyday behavior.
Footnotes
Acknowledgements
We would like to thank Dr. Mónica Tentori and Dr. Jesús Favela for their feedback on the early version of the manuscript. We also thank the students of the School of Engineering, UABC, who helped us to recruit and interview older adults.
Contributorship
All authors contributed to the conception and design of the research. KS led research activities in the UK and MDR in Mexico. KS wrote the first draft. All authors reviewed and edited the manuscript and approved the final version.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the UK EPSRC (grant number EP/G059063/1) CHI + MED: Multidisciplinary computer–human interaction research for the design and safe use of interactive medical devices. KS was supported by EPSRC-DTG. MDR was supported by CONACyT (project ID: CB-2010-01/153863). The international collaboration was made possible through the FP7 Marie Curie IRSES Ubi-Health Network, ![]()
Ethical approval
The research was approved by UCL Ethics Committee, project ID: Staff/1213/005.
Guarantor
KS
Peer review
This manuscript was reviewed by Kathie Insel, University of Arizona and Eleni Karasouli, University of Warwick.