
Abstract
Multimorbidity, defined as the concurrent experience of more than one chronic health condition in an individual, affects ∼65% of people over 65 and 85% of those over 85 years old with 30% of those also experiencing mental health concerns. This can lead to reduced quality of life and functioning as well as poorer outcomes in terms of condition management, adherence to treatment, and ultimately disease prognosis and progression. Digital health interventions offer a viable means of condition self-management, as well as psychological support, particularly for those who may have difficulty accessing in-person services. To best meet the needs of older adults with multimorbidity, deeper insights are needed into their specific concerns and issues around condition management, particularly with regard to distress in relation to managing one's condition. The present study aimed to explore this using one-to-one qualitative interviews and focus groups with people with chronic health conditions and healthcare professionals. Participants were 11 older adults with multimorbidity (4 males; mean age: M = 72.7 years) and 14 healthcare professionals including five clinical nurse specialists, four pharmacists, two general practitioners, one occupational therapist, one speech and language therapist and one dietician. Thematic analysis was used to identify key themes, which included: patient feelings of anxiety or worry leading to an unwillingness to access essential information; the various mental health challenges faced by those with multimorbidity; the importance of personal values in providing motivation; and the importance of social support. Findings are discussed in relation to the potential development of transdiagnostically applicable digital interventions for the management of distress in those with multimorbidity.
Background
Multimorbidity is defined as two or more chronic health conditions (i.e. un-curable, long-lasting illnesses) 1 and is a considerable issue in older adults, affecting ∼65% of people over 65 years old and 85% of those over 85 years old globally. 2 Chronic illnesses typically bring about a complex set of symptoms and demanding lifestyle adjustments. The burden of managing such conditions (known as ‘treatment burden’) 3 is associated with reduced quality of life as well as less time spent engaged in social or personal activities. 4 While research shows that the majority of those diagnosed with a chronic illness eventually show good psychological adjustment, ∼30% take considerably longer to adjust or in some cases, do not. 5 Moreover, upwards of 30% of individuals with one or more chronic health conditions such as heart failure or chronic obstructive pulmonary disease (COPD) also experience a clinically significant mental health concern such as depression or anxiety.6–8 Depression and anxiety are associated with poorer treatment adherence, reduced functionality, increased hospitalisation, and increased mortality risk across studies.9–11 Therefore, management of psychological distress (defined by Viertiö et al., 12 as non-specific symptoms of depression, anxiety, and stress, which are indicative of mental health impairments, including clinically significant mental health concerns in some instances) in those with multimorbidity is not only important for improving quality of life and functioning, but is also critical for management of their condition, adherence to treatment, and ultimately disease prognosis and progression. Research has found that psychological support can improve quality of life, symptoms of distress and disease management in those with chronic health conditions.13–15
Disease self-management is defined by Barlow et al. 16 as an individual's ability to manage the necessary responsibilities involved in preventing complications and/or progression of the disease, including managing symptoms, medication use, and relevant lifestyle and behaviour changes. However, studies show low levels of adherence to self-management following the diagnosis of chronic illnesses.17–19 Findings from a review by de Ridder et al. 20 indicated that mood levels appear to considerably impact an individual's ability to engage with necessary lifestyle changes, with even low levels of distress or unwanted/uncomfortable thoughts impacting one's ability and willingness to self-manage conditions. Higher levels of depression, in particular, are linked with poorer self-management of diseases with studies indicating that it is a major risk factor for treatment non-adherence (e.g. not taking medication as directed).21–23
On the other hand, factors such as a sense of control over disease and leading a values-driven life have been found to improve self-management of disease.24,25 One issue that has been found to considerably impact adherence and willingness to self-manage in those with chronic conditions is avoidance-based coping. Suppression of fear and unwanted thoughts about the realities of living with one's condition can lead to inaccurate perceptions around one's health and therefore insufficient management or treatment adherence. 25 There is also considerable evidence to suggest that issues around medication adherence and self-management are linked to avoidance of unwanted thoughts and feelings in relation to the disease in question, including shame and fear.25–27
The majority of empirical investigations into psychotherapeutic interventions for those with chronic health conditions conducted to date involve in-person therapy, which typically can be quite costly, time-consuming and difficult to access, particularly for those dealing with the additional demands of chronic diseases. 28 Interventions delivered in the form of a digital application may offer a solution, and while they have not been extensively investigated in those with chronic health conditions, there are promising findings emerging across a wide range of outcomes, including but not limited to well-being, quality of life, adherence, and self-management behaviours.29–31 Digital psychotherapy offers a number of advantages over traditional in-person therapy, in addition to being more cost- and time-effective, 32 digital interventions (including those based primarily online) have also been shown to increase health literacy and knowledge, to improve coping 33 and to reduce stigma as they can be used anonymously. 34 Evidence also suggests that digital interventions can result in reduced depressive symptoms in older adults.35,36 They also provide increased availability and flexibility 37 which is particularly important for older adults with multimorbidity. Findings from a recent meta-analysis indicated that therapy delivered by means of video-conferencing technology is no less effective than in-person therapy. 38 Digital therapy has been particularly important during the COVID-19 pandemic in cases where it was not possible to access in-person therapy and while research is still preliminary, promising findings have been observed for the use of online and video psychotherapy in the context of the pandemic.39–41
However, a number of issues have been identified by researchers, among which include, user concerns regarding privacy and data security, communication issues as a result of technology, user concerns about therapist competence and efficacy of therapy, and limited empirical evidence to date.37,42,43 While there is a dearth of research involving samples of older adults, studies examining older adults’ use of digital health apps indicate that there are similar concerns around data security and confidentiality and accuracy of the information given as well as issues around usability and understanding.44–46 Digital health platforms and applications have the potential to support effective self-management behaviours for older adults with single or multiple chronic conditions. 47 Such systems often include features such as symptom monitoring and data review, education, goal-setting and sharing of data within a care network. There is little evidence in human–computer interaction and design research on integrating interventions to address psychological distress alongside chronic disease management. Research has explored stand-alone mental health applications, typically with a focus on stress, for example, the needs and preferences of students in relation to self-tracking mental health data, 48 how to visualise sensor-based stress data for self-management 49 designing digital mindfulness technologies for stress management, 50 the use of digital cognitive behavioural therapy 51 and how to integrate digital and human therapy for the management of depression. 52 Furthermore, older adults are generally underrepresented in research exploring digital mental health interventions.53,54
In order to best meet the needs of older adults with multimorbidity, it is important to understand what it is like to live with and manage multimorbidity, especially in relation to mental health challenges. This will allow for an advanced understanding of how best digital health technologies may support the mental health needs of such populations. To this end, this article presents a qualitative study exploring these issues with older adults with multimorbidity and healthcare professionals (HPs). The findings presented in this article indicate a range of issues that can potentially impact effective self-management related to mental health and well-being and as such an intervention approach is recommended to address this range of concerns.
Method
Sample and design
The present study involved secondary qualitative analysis of semi-structured interviews and focus groups with older persons with multimorbidity (PwMs) and HCPs, which were conducted as part of the requirements gathering phase of the ProACT Horizon 2020 project, 1 to investigate how the use of digital technology might support older adults self-managing multiple chronic conditions. Each participant took part in one interview or focus group (dependent on convenience), which explored a range of issues relating to multimorbidity management, the challenges associated with it and strategies to support effective self-management. 55 Current usage and perceptions of technology across stakeholders were also explored and have been reported elsewhere. 56 While these data have been previously analysed to broadly examine self-management challenges and the use of digital technologies as a way of managing them, the impact of living with multimorbidity on mental health and the impact of any mental health concerns on the ability to manage one's conditions have not yet been explored in the data.
Participants
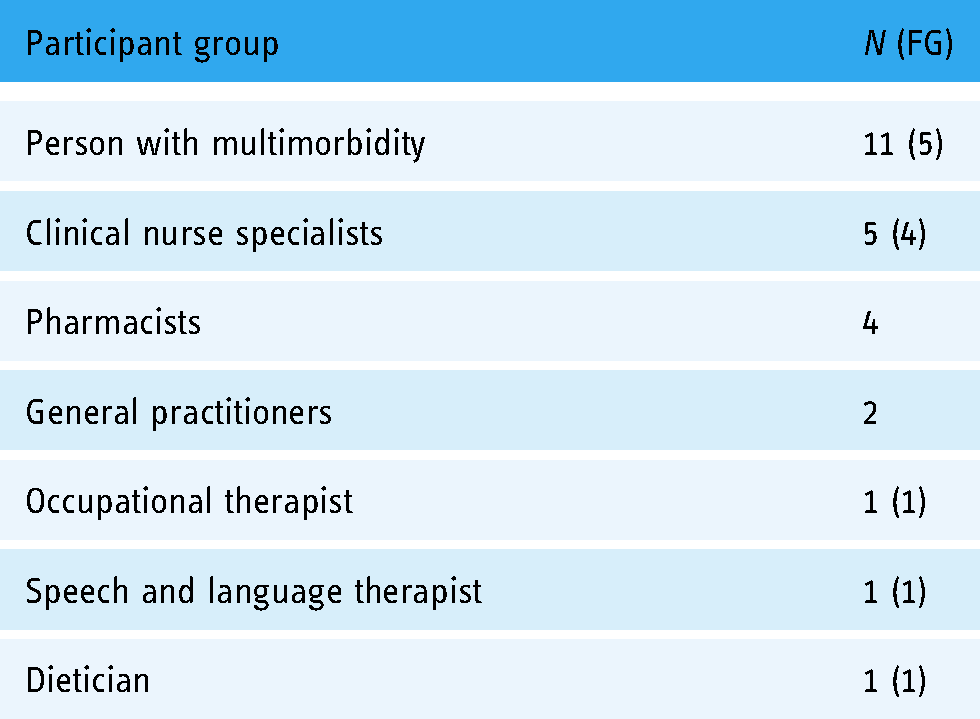
Eleven older PwMs (4 males; mean age: 72.7 years, age range: 60–84 years) and 14 HCPs took part. HCPs were recruited through existing links with local hospitals and clinics while PwMs were recruited through HCPs, formal care organisations, living labs and various social groups for older adults using convenience sampling methods. Inclusion criteria for PwMs were people aged 60 years or older, with two or more conditions (diabetes, COPD, chronic heart disease (CHD), congestive heart failure). However, most PwM participants who took part had additional co-morbidities beyond those of the inclusion criteria (see Table 2) and as such the interviews and focus groups resulted in discussions related to self-management of all conditions.
Participant demographics.

CHD: chronic heart disease; COPD: chronic obstructive pulmonary disease.
Data collection
The breakdown of participants who took part in focus groups and interviews is provided in Table 1, with a more detailed breakdown provided for individual PwM participants in Table 2. All interviews and focus groups were semi-structured and lasted between approximately 45 and 120 min. Both interviews and focus groups followed the same protocols and were broken down into a series of topics, including health conditions and their impact, patient journey through the healthcare system, care plans and goal-setting, self-management, integration of care and communication, medication management and technology supports. All interviews were audio-recorded and transcribed verbatim for analysis.
Study sample breakdown of persons with multimorbidity and healthcare professionals.
Analysis
Thematic analysis was used to analyse the data 57 and NVivo for Windows (Version 12, QSR International, Doncaster, Australia) was used to conduct coding. A thematic analysis provides a flexible and iterative method of identifying patterns within the data. 57 Analysis was primarily inductive in nature, wherein the researchers used a bottom-up approach to generate themes and patterns within the data. However, analysis was broadly guided by the research aims with coders paying particular attention to codes pertaining to mental health and psychological well-being. Themes were also generated at a latent level, wherein analysis goes beyond the semantic meaning of the presented data, instead of focusing on ‘underlying ideas, assumptions, and conceptualisations’. 57 , p.84 Following completion of initial coding (by OM), all study authors were consulted to discuss, recode and categorise codes into themes until agreement was reached on all themes and subthemes. In order to assess reliability, two transcripts were selected at random (one person with multimorbidity (PwM) and one HCP) and coded in full by a second coder (SS) and subsequently matched to establish a reliability score. Inter-rater reliability was calculated using Cohen's Kappa statistic. Cohen's Kappa is considered superior to percentage agreement and controls for common absences and scores should be upwards of 0.4 to be considered reliable 58 Cohen's Kappa for the present study was 0.556.
Results
Participant demographics are summarised in Table 2
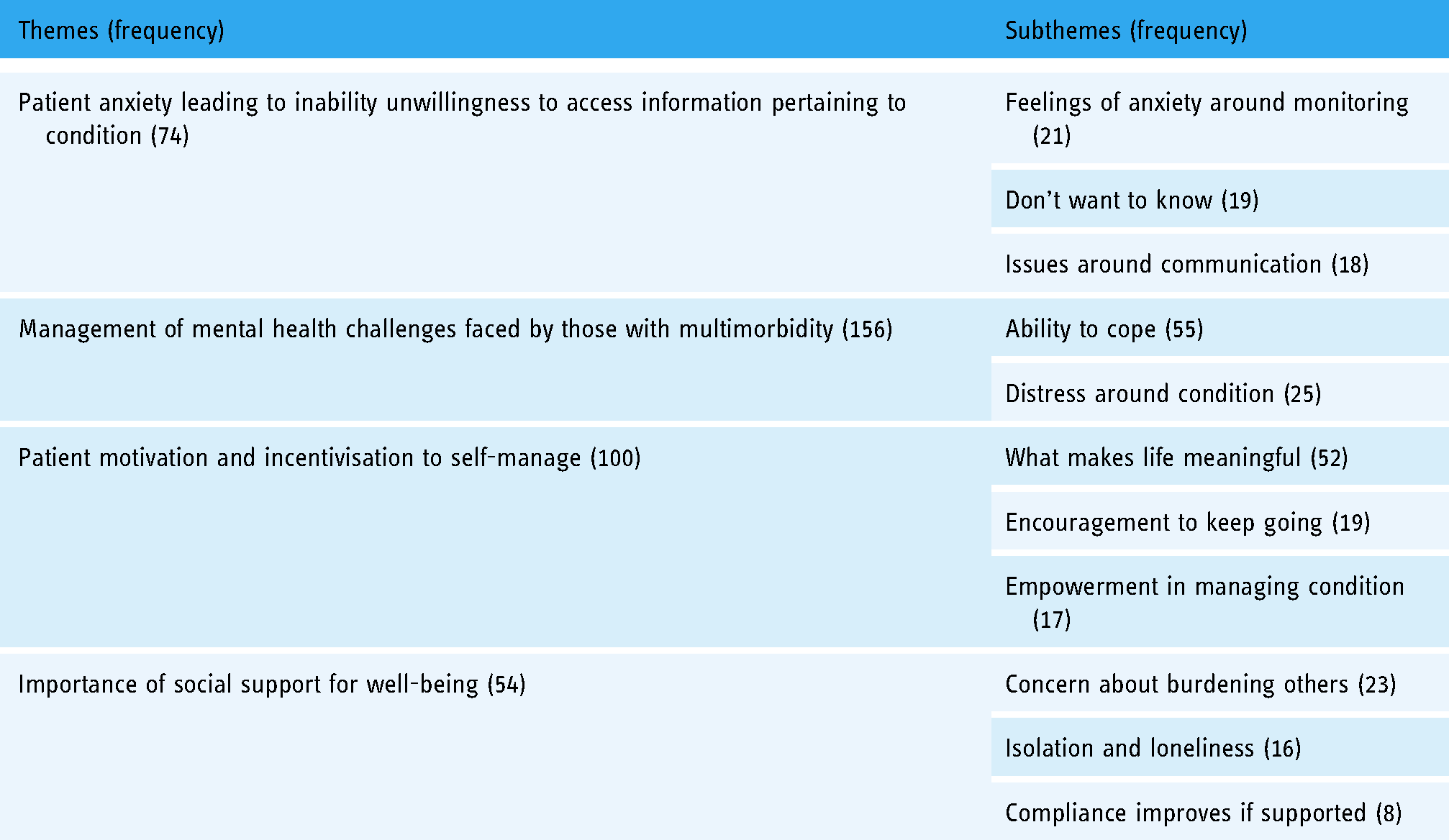
Study results, including themes and subthemes generated from the data and the number of times they occurred in the data, are summarised in Table 3. Four overarching themes were identified, namely, patients’ feelings of anxiety leading to inability/unwillingness to access information pertaining to condition; management of mental health challenges faced by those with multimorbidity; patient motivation and incentivisation to self-manage; and importance of social support for well-being; with between two and three subthemes corresponding to each main theme.
Coding frame detailing the frequency of themes and subthemes within the data.
Patient anxiety leading to inability/unwillingness to access information pertaining to condition
Feelings of anxiety/worry and distress around acquiring various types of health-related information were identified as issues by both HCPs and PwMs. One pharmacist talked about how when PwMs were feeling distressed and overwhelmed following news regarding their condition, it could make it difficult for them to communicate and process information regarding their condition: It's just too much sometimes you know [for them to take in]… and then sometimes they might ring the next day and say oh what do I do with this or you know, so it's kind of they haven’t thought to ask the question maybe at the time, or maybe you’ve said it to them and it just hasn’t registered which I supposed is fairly common as well you know. (Pharmacist 1)
Likewise, they talked about how feelings of confusion and anxiety, which were frequently induced by a hospital environment, could impact communication and consequently ability to accurately share necessary information: Certainly in all cases where somebody will not tell a doctor, I’m not allergic to it and they are, but again it's just that they are confused in the hospital setting whatever it is, maybe get a little bit panicky (Pharmacist 1).
A number of subthemes also fell under the overarching theme of Impact of Feelings of Anxiety on Acquiring Information, namely Feelings of Anxiety around monitoring; Don't want to know; and Issues around communication. These are discussed in further detail below.
Feelings of anxiety around monitoring
PwMs and HCPs reported symptoms of anxiety/worry and distress around monitoring symptoms and taking readings were a considerable issue. As one GP reported, for some patients monitoring caused increased feelings of anxiety, especially where readings may not be completely accurate: We wouldn’t give a pulse oximeter. In fact it would add to their neurosis. It would add anxiety and people reacting to figures rather than if it wasn’t fully on their finger or on the wrong finger or the machine needing batteries. But actually that would add to neurosis for sure. (GP)
This could in turn lead to obsession with figures or even affect the accuracy of readings, making them appear worse than they are: They get very obsessed with specific figures. Rather than you know, and they get annoyed at the figures and that makes them worse and worse, whereas in fact you settle down and if you leave it for a while and repeat again, so. (GP)
One PwM also reported that she would not take readings due to fear of seeing something she did not want to: No. I’d be afraid to go near them…just in case they’d be high and I’d be trying to figure out. (IE-01-0004, Female, 67)
Another talked about how they noticed others obsessing over symptoms and the feelings of anxiety that this often brought about: And some people, I know I have a friend and she used to convince herself that she had more conditions when she was quite young, because if she saw a spot here it would have to be skin cancer and if she saw a lump somewhere else it would have to be cancer, and she nearly drove herself mad. And I said why are you looking up that you are getting these ideas, and she had bought herself an encyclopaedia, a medical encyclopaedia. So I think the less you know in that line the better, but just if the doctor decides what you have and you go for your check-ups and you’re told what to do and you just follow your instructions, you know. (IE-01-0016, Female, 75).
Don’t want to know
Both HCPs and PwMs reported that when acquiring information on health conditions, avoidance and not listening/engaging were common as a result of patient feelings of anxiety and not wanting to hear something that may scare them: They do but they don’t retain it all and sometimes they don’t hear it all and sometimes they don’t want to know. (GP)
HCPs reported that they had to persistently follow up with patients to ensure they had the necessary information in cases where they were reluctant to hear it: They don’t want to know, but you kind of have to bring them, haul them back in. (Clinical Nurse Specialist)
PwMs also reported that they would be satisfied with obtaining the minimum amount of knowledge essential to manage their conditions and did not want to know any unnecessary information: No, I was in the hospital when they said it to me and when they would say things to me I’d never ask them any questions for the simple reason, I don’t want to know, like, leave me with what I have and I’ll manage with what I have but don’t go into the ins and outs because I wouldn’t have a clue what you’re talking about. (IE-01-0017, Female, 60).
Issues around communicating
Fear of judgment from HCPs meant PwMs were unlikely to tell their doctor or other HCPs if they were not adhering to treatment or encountering issues. For example, one pharmacist reported participants can be afraid to ask what certain medications are for and to communicate to their doctor when they have stopped taking medication: I don’t know, I think they’re afraid sometimes to ask what they are for, I think they are afraid to tell their GP that they are not taking it, or maybe afraid to tell us they are not taking it thinking that they will be in trouble or something, and you know that's not going to happen here you know, people just need to know what they are taking and what they are not taking really for their own sake. (Pharmacist 1).
A PwM participant also referred to this, reporting reluctance to ask questions about her medication due to fear of judgment from HCPs: I don’t know. I don’t know anything about them. You mightn’t ask because they’d look at you as if you had two heads. So I say no I’m not going to ask you at all. (IE-01-0004, Female, 67) And if you want your patient to feel that they can ask you about something. You’d mention that there's a day centre and on what days. You want that to happen. So you want them to feel that they can ask the questions that you have that rapport. (Occupational Therapist)
Management of mental health challenges faced by those with multimorbidity HCPs and PwMs discussed the various mental health challenges that frequently affect people with multimorbidity, and the different supports and means of managing mental health concerns. One PwM discussed how his carer supported him by managing things that may bring about stress and ultimately helping manage symptoms of depression: I don’t stress myself – you know – and that's part of why I have a carer – that she, she looks after a lot of the de-stressing stuff that I would get stressed about and that's keeping my depression under control. (IE-01-0005, Male, 80)
The same participant also talked about having frequent psychiatric support, particularly when encountering issues or events that would bring about difficult emotions: I have seen my psychiatry person usually every 2 months and if I feel that I am having a problem or coming up to a difficult period, em, you know, for example, my wife's anniversary now in July I’ll, you know, I will get something from him to steady me during that time cause that's a high stress time and you know, I manage that. (IE-01-0005, Male, 80)
Subthemes that also fell under the theme of Managing Mental Health, included Ability to Cope and Distress around Condition and are discussed in further detail below
Ability to cope
PwMs described their ability to deal with their illnesses and the challenges associated with them, including a positive outlook and psychological support. One participant emphasised the importance of having an optimistic outlook: Well I was always very positive. You know, and I think I’m an optimist You know the little story about the optimist and the pessimist – the difference is droll – one sees the doughnut and the other sees the hole. [Laughing]. And I see the doughnut. And the glass is always half full not half empty. So I think that is very important, to have a positive attitude. (IE-01-0010, Female, 75)
Another PwM spoke about how he chose to stop keeping a record of his pain as it was causing him to dwell on negativity when he wished to keep his attention on the positive: And I keep it in a diary and then you can take it to the benefit office or that. And I started doing that and I thought, no. I’m not doing that. It's giving you a negative, because you are continually conscious about the negativity of something rather than the positive. You are thinking about pain, pain instead of thinking about how well you are doing. (IE-01-0013, Male, 66)
He also spoke about the importance of being aware of the limits of what he could do on a given day: I seem to cope but I have to take notice of my limitations as well. (IE-01-0013, Male, 66) You know the grieving for my wife, em, so I really had broken down into two areas – I had the depression area and I would discuss that with him and then I would move to the grieving area – you know I am having trouble here, you know (IE-01-0005, Male, 80).
Another participant spoke about the difficulty she was experiencing with her condition slowing her down and making it difficult to do the things she used to: But I find it very hard and very frustrating, like I worked till I was 67… I’m finding it very, very hard to cope. (IE-01-0010, Female, 75)
Distress around condition
HCPs talked about how one's mental health and well-being was frequently impacted as a result of their diagnosis and the impact their condition has on their lives. One pharmacist talked about how feelings of anxiety and confusion were common when patients were trying to manage medication for multimorbidity: I think sometimes it can be very confusing for them, especially if there is a few conditions going to go, I think it worries them I think it stresses them out sometimes, I think they can be quite anxious about it. (Pharmacist 1) It's hard to go out and watch people enjoying themselves, say dancing, knowing that it's not possible to join in because you’d be too winded. Going out is a problem because of perfumes, flowers, air fresheners, damp, smog, smoke, burning candles and so on. (IE-01-0017, Female, 60)
She also described how she found it difficult to need help doing basic self-care tasks: She (carer) also helps me showering. I wash myself but she has to dry me. It is very hard having to have someone help with showering. (IE-01-0017, Female, 60)
Patient motivation and incentivisation to self-manage
Both HCPs and PwMs spoke about how identifying what personally motivates each patient increases their sense of empowerment and therefore the likelihood of adherence to self-management. An occupational therapist gave the example of identifying what motivates patients to take action and get to a place where they can be discharged from hospital or an inpatient setting (particularly where they might be getting overly settled): Sometimes motivation is the problem really. And sometimes they, as D said, sometimes patients get so comfortable here, they actually really enjoy it here. Sometimes you need them to see that they’re only here for a short time. So sometimes the motivation might be, well we’re looking at discharge now, and discharge is going to be in the next two weeks. So it might be the shock they need in terms of ‘I’m not going to be left here forever’. (Occupational Therapist)
What makes life meaningful
HCPs stated the importance of identifying what was personally meaningful to each patient and provided incentive and motivation to engage with condition management: You kind of need to see for each patient, what motivates them. One patient might need to get out cos they’ve grandchildren. You have to see what you can use as motivation for each patient. (Speech and Language Therapist)
PwMs also described what they valued in life and what gives them joy: Seeing family. I love chatting [laughs] you know. That would be my pastime. (IE-01-0012, Female, 76)
And helping people – I like helping people… and I like to keep them happy by telling them stupid jokes and that sort of thing, you know. (IE-01-0014, male, 82)
Encouragement to keep going
HCPs and PwMs spoke about the importance of persevering and doing what needs to be done in order to manage conditions and get on with day-to-day life. One HCP emphasised the importance of encouraging patients and reminding them of how well they are doing: It's perseverance. You have to encourage them, say you’re doing great. (Dietician)
One participant spoke about how he needed to avoid sitting around and push himself to ensure he was doing the things that needed to be done and creating targets to meet: The challenge for me is to push myself. Is to, you know, not sit on the sofa (laughing). The big challenge is actually getting up and doing things, and setting targets and making a list of things that need to be done, and doing them. (IE-01-0013, Male, 66)
Similarly, another PwM also spoke about the importance of pushing herself to do things and staying active in order to maintain some quality of life: Like it's just – it's a big change, you know. But I will try and keep going as long as I can. I won’t be one of these sitting at home…. I have a sister who just sits in the same chair the whole day smoking, you know. And I won't be like her… But she'd no quality of life I wouldn’t like to become one of them so that's why you try and keep active, keep going – as long as I can, you know. (IE-01-0012, Female, 76)
Empowerment in managing conditions
Encouraging patients to take ownership of their conditions and have the necessary knowledge to self-manage (or seek help when needed) led to an increased sense of empowerment for them: We would get them to weigh themselves at home… and to ring us if they are unwell, and to monitor their own symptoms and really try to empower them to look after their own health, give them the knowledge to look after their own health and to recognise when they are unwell and that they may need to be seen. (Clinical Nurse Specialist) I think we would all be striving to empower the individual patient. Obviously ethics comes into it as well, if you want to involve family. At the end of the day, once the patient has consented, you have to ask them if its ok to involved. But I think we do all try as much as possible, unless there's a real cognitive impairment where you would be worrying about something, in terms of if you’re educating a patient and you really feel they’re not going to be able to manage something. Unless it was something like that. (Occupational Therapist)
One PwM spoke about how he felt a sense of confidence and control around managing his condition but would still like to have the option to look for information online: I could probably be doing other things, you know, like using the internet and things like that – if it were available, I would use it probably. But as things stand, I, I feel I am in control of what I am doing, you know. (IE-01-0005, Male, 80) Oh I do because I am a very independent person. I would be kind of feeling that people were interfering with me if I was, you know. As long as I am able to do it you know. I mean if I am not able to do it that would be a different thing, you know. (IE-01-0010, Female, 75)
Importance of social support for well-being
HCPs emphasised the importance of social support and staying socially active for patients’ overall mental health and physical well-being: … the more socially active you are the better your quality of life or your wellbeing, so your social context, do you get out and about to meet like active retirement or girls for coffee or something like that, or that social interaction. And also family you know, have you a good family network, that makes a huge difference as well, so all that social thing is very, very important. (Clinical Nurse Specialist). And it's a social thing as well. Because apart from trying to get people physically healthy, it's a mental thing as well that you’re trying to. And you’re encouraging people then to get together as a group in the community. So it's a win–win. (Pharmacist 2).
One PwM also spoke about how socialising and going out to meet people was very important for her quality of life, particularly as she frequently felt lonely at home following the passing of her husband: You get in the company and you are having the craic (fun) and then you realise you are going home to nobody, you know that kind of way. (IE-01-0012, Female, 76).
Subthemes that fell under the theme of Social Support included Concern About Burdening Others; Isolation and Loneliness; and Compliance Improves If Supported, and are discussed in detail below.
Concern about burdening others
Fears of burdening family members, carers or even HCPs made many PwMs less likely to reach out or ask for help when needed. PwMs frequently reported that they were unlikely to seek help or support from their families as they did not wish to worry them: Well it was made for me more or less, I came out of hospital, that is your room now, and I couldn’t put my family like to worrying you know, it's alright. (IE-01-0003, Female, 84) Well the way I look at it is, they all have their own families, they all have their own problems, and I’m not going to put more on them. (IE-01-0010, Female, 75)
One PwM also reported she was less likely to seek medical help due to concerns around burdening doctors: No, well I suppose I never really mentioned it to her too, you know. You just try and carry on, you know. You don’t like to be complaining all the time, you know that kind of way. (IE-01-0012, Female, 76)
HCPs echoed this, with the occupational therapist stating that they frequently noticed older adults were less likely to seek out support and do the things that they wanted to due to feelings of being a burden: The problem sometimes is the older person actually feeling as they’re ageing or becoming more elderly, that they’re more of a burden. So they actually might be interested in attending a support group or a day centre because they don’t want to put the burden on sons and daughters cos they feel they have their own busy lives. (Occupational Therapist)
However, they noted that typically when the PwM asked for support, family or carers were happy to help. Therefore, encouraging PwMs to ask for help and undermine unhelpful beliefs about being a burden was very important: And sometimes then you’d ask well have you ever asked them? But they might say they’re already bringing them their dinner every day, so they don’t want to be asking them to bring them to the day centre. And you’d say well did you ever think of asking your son? And it's never usually a problem. Maybe it's just trying to get that communication going, setting the ball in motion, but not being too evasive and nearly taking it upon yourself to say, would you ever bring your Dad to the day centre? Sometimes that's the problem, they think they’re a burden and have to be brought everywhere. Sometimes that's maybe the obstacle. Quite often it's just breaking that mindset. (Occupational Therapist)
Isolation and loneliness
Social isolation and loneliness were reported as considerable issues in older adults with both HCPs and PwMs emphasising the importance of having some form of social support for well-being. One PwM spoke about how she got along well with her carer which she particularly appreciated as her neighbours did not mix with her: Because I like her, she's lovely, we get on well, but just to know there was somebody coming in every morning and as I say to you, they don’t mix here, everybody keeps to themselves, I would feel secure. (IE-01-0010, Female, 75) Have friends but they don’t visit very often. I don’t get invited to parties any more. At the beginning I did but I suppose they were always watching me and worrying when I would be coughing and then they stopped inviting me. I suppose I understand but I wish they visited more often. (IE-01-0017, Female, 60)
A further PwM talked about how a phone support service helped when he felt isolated: No I think the other thing is the calls, like if I really felt isolated, that morning call thing they have. (IE-01-0013, Male, 66) So it's a load of physical, social then you kind of also checking then socially are they isolated, you know is there anybody going there, the poor dear are they getting out at all, or is there plenty of family support or whatever. And also then have they got the carers in, have they got access to day care respite if they want you know as well. (Clinical Nurse Specialist)
Compliance improves if supported
HCPs reported that if a PwM had a good source of support, via their family or wider care network, they were more likely to comply with condition management: I think that helps people be more compliant with their treatment if they feel somebody is on their side and trying to help them out a bit as regards not just saying you have to come here and you have to be here at such and such time, getting them on board, you know you have to (Clinical Nurse Specialist). Taking their medication and we find patients who have good family support do better in the long run, just our observation. (Clinical Nurse Specialist).
One pharmacist also noted that family members could also provide support in cases where confusion and related issues may impact patient compliance by checking blister packs to see if medication is being correctly taken: Not that they may not want to or they don’t properly adhere, but they may be just confused with it. So the handiest way is just put it in a blister pack, and then you can keep a better eye on compliance. Or a family member can keep an eye on compliance by checking everyday. (Pharmacist 2).
Support from one's clinical network was also important for ensuring patients developed a trustworthy relationship with HCPs and were honest about whether or not they had been taking medication correctly: I suppose if you are building up a trustworthy relationship and a lot of elderly people depend on the pharmacist because they are there in the local community and you build up a rapport with them, that trust in the relationship, you are relying on the person telling you if they have taken their medication. (Pharmacist 2)
Discussion
This study aimed to explore the experiences of older PwMs, the challenges that come with managing multimorbidity and their potential impact on mental health, and moreover, how poorer mental health and well-being may lead to issues around disease management and coping. Relevant HCPs were also involved in this study to gain a more holistic understanding of the challenges PwMs are faced with. Conducting a thematic analysis of the one-to-one interviews and focus groups with these populations of interest, the following key themes were identified in the data: patient feelings of anxiety leading to inability or unwillingness to access essential information and not wanting to know details pertaining to one's condition; the various mental health challenges faced by those with multimorbidity and how they were managed; the importance of personal values in providing motivation and an incentive to better self-manage; and the importance of access to social support for well-being.
These findings were consistent with previous investigations, which also found patients were likely to avoid potentially distressing information or activities that are essential to condition management,25–27 while greater feelings of control around one's condition and connection with personally held values have been linked to better disease management.24,25 Both PwMs and HCPs spoke of feelings of anxiety around monitoring, fear of honest communication with HCPs and avoiding information about conditions, all of which are important for effective day-to-day self-management. As Barlow et al. 16 note: ‘efficacious self-management encompasses ability to monitor one’s condition and to effect the cognitive, behavioural and emotional responses necessary to maintain a satisfactory quality of life’. Furthermore, successful self-management requires people to have sufficient knowledge of their conditions as well as how to perform the necessary activities for self-management. 59 However, it is well understood that self-management of multiple chronic conditions is particularly challenging and can be overwhelming, particularly when anxiety is also present. 60 Therefore, solutions are required to address participant fears and anxiety in relation to chronic conditions and self-management activities. It should also be noted that while HCPs reported concerns regarding patient avoidance of details regarding their conditions, perspectives from PwMs indicated that this was not necessarily always linked to anxiety or fear of hearing something they did not want to. Rather in some cases participants reported they did not necessarily understand all of the information provided to them and did not find unnecessary details helpful. This is an important finding as while it is critical to ensure patients engage with all pertinent information, where possible information must be delivered in an accessible and manageable manner.
Social support has also been identified as important for both mental well-being, better disease management and compliance in previous studies.61–63 While disease self-management places a high level of responsibility and control on the individual, the importance of one's context, in particular, one's social context cannot be underestimated. Positive, supportive interpersonal relationships play a considerable role in better self-management and overall disease outcomes, by providing means of both emotional and illness-specific support.61,64,65 Likewise, the deleterious impact of loneliness and social isolation on the physical health and overall well-being of older adults has been widely documented.66,67 Findings from the current study further emphasise the importance of assessing a PwM's social context and identifying ways in which to increase social engagement wherever possible.
Furthermore, as with previous research,5,6 some PwM participants reported feeling like they could cope with difficulties brought about by multimorbidity or other aspects of ageing, particularly if they had access to psychotherapeutic support, while others reported that they were struggling to cope indicating a need to equip older adults affected by multimorbidity with effective coping strategies. Regardless of the presence of chronic health conditions, the experience of ageing is associated with considerable losses across a variety of life domains (death of loved ones; decreased socialising; reduced health and functioning; and cessation of working life and past-times) all of which may considerably impact the quality of life.68,69 Studies indicate that reactions of older adults experiencing such events vary considerably depending on individual attitudes and ability to cope, with a willingness to accept thoughts and feelings associated with these life changes identified as particularly important.70,71 These findings highlight the importance of implementing effective coping skills in older adult populations regardless of health status, in order to improve the overall quality of life and well-being.
The importance of motivation and personal empowerment has also been widely documented in the literature, with managing one's condition in a manner consistent with one's personal values and preferences associated with greater disease understanding and acceptance, and better coping for affected individuals.72,73 In order to meet the complex needs of those with multimorbidity and improve their mental well-being and adherence to positive self-management behaviours, an effective psychotherapeutic intervention is needed that reduces avoidance behaviours (e.g. avoid monitoring), undermines unhelpful beliefs (e.g. ‘I’m a burden’), and increases valued directed behaviours (e.g. spending time with family or friends). To address these key issues identified in the present study, this article proposes that designers of digital health platforms that aim to support self-management of single or multiple chronic conditions should consider the integration of an acceptance-based, transdiagnostic (i.e. universally applicable regardless of symptoms or diagnosis) therapeutic approach, such as Acceptance and Commitment Therapy (ACT), 74 for which empirical support has been observed for its use with a plethora of conditions, including chronic illness.75–77 Such an intervention can help foster a process known as psychological flexibility, which creates lasting behaviour change by increasing committed action in the service of personally held values, while allowing for and accepting (rather than changing) difficult or unwanted thoughts, feelings and self-evaluations that may arise as a result. Future investigations should explore the feasibility and effectiveness of such a digital therapeutic intervention for older adults with multimorbidity. Should this be found to be suitable, such an intervention would answer the call for evidence-based, but accessible and wide-reaching treatment to improve management of multimorbidity, well-being, and overall quality of life.
Strengths and limitations
This study involved a large and diverse sample of older adults with a broad age range, a wide array of health conditions and relatively balanced for gender. A wide range of HCPs were also recruited ensuring a range of diverse perspectives. Future studies could add further insights by also examining the views of patients’ formal and informal carers, such as family members. Given the findings from this exploratory study, it would be beneficial to examine further the perspectives of mental health professionals (e.g. psychiatrists, psychologists, etc.) who work with older adults affected by multimorbidity.
Future studies may provide more in-depth insights through a more detailed examination between older adults and older old adults (e.g. adults in their 60s compared to adults in their 80s and 90s), given the reported steady decline in quality of life as one ages. Likewise, a detailed examination of the experiences of those who have been diagnosed with a clinically significant mental health concern compared to those who have not would be particularly valuable. Future studies should also involve larger samples with data collected longitudinally where possible to account for potential ongoing changes in experiences and reduce the risk of bias (e.g. participant was having a bad day and therefore reported more negatively than normal). Finally, given that the current study was conducted entirely within an Irish context, future investigations should strive to explore these issues across various international samples to account for differences in cultural contexts.
Conclusion
Study findings highlight the role of mental health for quality of life, treatment adherence, and self-management in older adults with multiple chronic conditions. Digital health applications that support monitoring and self-management of chronic conditions should also explore the inclusion of a psychotherapeutic component that targets avoidance behaviours and increases more effective coping and self-management behaviours, such as ACT.
Footnotes
Acknowledgements
We would like to sincerely thank all of the participants of this research for their valuable time.
Ethical approval
Ethical approval was received from the School of Health and Science Research Ethics Committee at Dundalk Institute of Technology, the Health Service Executive North-East Research Ethics Committee and the Faculty of Health Sciences Research Ethics Committee, Trinity College Dublin.
Contributorship
JDo and JDi conceived and designed the study, developed the interview and focus group protocols and were responsible for gaining ethical approval for the study. JDo, SS, and JDi were involved in data collection. OM, JDo, SS, and OG were involved in data analysis and interpretation. OM and JDo wrote the first draft of the manuscript and all authors were involved in reviewing and refining the text.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the European Union’s Horizon 2020 research and innovation programme, EU’s INTERREG VA program (grant number 689996).
Guarantor
JDo.