
Abstract
Background
NHS staff are disproportionately impacted by workplace stress, threatening not only quality of service delivery, but the sustainability, of this vital healthcare system. There is an urgent need for accessible and cost-effective interventions that promote the wellbeing of this integral workforce.
Aim
The aim of this study was to explore the potential propensity of a short virtual reality (VR) nature experience, delivered during the workday, to induce positive mood states NHS clinicians.
Method
NHS clinicians working in a fast-paced trauma service were offered the opportunity to take part in a short virtual reality (VR) relaxation session, during their working day, in which they were able to explore the “Green Meadows” experience available within the Nature Treks application. An indication of physiological arousal (heart rate) was obtained, and subjective measures of emotional state were employed to assess the effect of the intervention on participants’ mood. Further, feedback was gathered to provide an initial indication of the acceptability of the experience.
Results
Analysis of data from 39 clinicians revealed that, following the VR experience, participants reported significantly increased feelings of happiness (p < 0.001) and relaxation (p < 0.001), and significantly decreased feelings of sadness (p = 0.003), anger (p < 0.001) and anxiety (p < 0.001). No significant differences in reported levels of surprise (p = 0.603) or vigour (p = 0.566) were found. Further, the experience was associated with a significant reduction in heart-rate (p = 0.025), and had high acceptability ratings, despite participants’ varied experience with computers and VR technology.
Conclusions
The findings of this study indicate that the administration of VR for the promotion of NHS staff wellbeing in the workplace is a potentially fruitful avenue of exploration that warrants further investigation.
Introduction
Work-related stress, defined as “a harmful reaction that people have to undue pressures and demands placed on them at work” 1 is one of the most important emerging risks in occupational management and health. 2 Aside from the moral and social obligation to reduce the prevalence of workplace stress are the associated substantial economic consequences which can manifest through factors such as absenteeism, loss of productivity, higher staff turnover and a larger number of accidents and injuries. 2 Estimates indicate that 17.9 million working days were lost due to work-related stress, depression or anxiety, accounting for 51% of work-related ill health in 2019/20 alone. 1
As the provider of publicly funded healthcare in the UK, the National Health Service (NHS) can serve as a role model in workplace health. 3 The NHS is the largest employer in England, with around 1.1 million full-time equivalent staff in hospital and community services 4 and its workforce constitutes the system's greatest asset. 5 Yet, on many measures of staff health the NHS performs poorly in comparison to the public and private sector. For example, the category of professionals defined as ‘human health and social workers’ were found to have 2350 cases of work-related stress, depression and anxiety per 100,000 workers, a statistically significantly higher rate than the average for all industries. 1 NHS staff have recounted stories of unmanageable workload, intolerable stress, and loss of control by workers during confidential listening events. 5 These factors contribute to a worsening staff retention which reduces the number of NHS staff, decreases continuity for other staff and can result in increased provider costs in recruiting and training more staff. 6
Throughout the COVID-19 crisis, many health-care workers have worked long hours in high-pressured circumstances characterised by trauma and moral dilemmas, whilst also contending with the risk of infection, and by extension infecting their families in addition to the challenges of remote working for some. 7 Although staff may thrive in such circumstances, it is important to plan how to identify and support those who do not. This is particularly pertinent given that the NHS is already an under-resourced system, and that the health of the workforce has a direct impact on people's care. 8 Thus, the scale of workforce challenges facing the health system poses a threat to delivery and quality of care as well as the sustainability of the system. 6 Accordingly, the importance of health and wellbeing in the workplace is recognised increasingly among companies, local authorities and the government. 9
Challenges associated with workplace-wellbeing interventions
Subjective wellbeing as a multifaceted concept includes positive emotions, motivation and engagement, self-awareness, and mindfulness. 10 Although a variety of wellbeing strategies have been introduced into NHS contexts to foster these positive states, several barriers to implementation exist.
An obvious, but perhaps often unspoken barrier to the implementation of workplace wellbeing activities is that employees are expected to focus solely on their work during working hours. The implicit expectation for employees is that “resting is what they should do in their ‘‘own time” with non-paid lunch and coffee/tea breaks exemplifying this. 11 They point to a common employer assumption that ‘‘after work’’ is the time in which people should recover from their daily strains. In the NHS pressure may also come from an accepted workplace culture that includes working through breaks, working long shifts, coming to work when ill (presenteeism) and even skipping annual leave, particularly where staffing is under-resourced. 12
Yet, resting during the working day is a beneficial self-care strategy that can temporarily provide relief from demands, allow resources to be replenished, and reduce fatigue. 11 Resting allows arousal levels (as indicated by adrenaline excretion rate and heart rate) to return to a ‘‘baseline level’’ again. 13 The anticipated positive psychological effects of taking a short rest during the day are that people feel capable and ready to meet new demands or continue with current job demands.
Another difficulty with workplace wellbeing initiatives is that many interventions such as relaxation, can involve techniques that are difficult to learn and are usually taught by a therapist making them difficult to engage with during the working day. 14 For example, mindfulness-meditation has been widely used throughout the last several decades in medical practice as a stress-reduction tool. 15 However, such practices are not easy to integrate into a daily routine as they require time, ongoing practice and effort. 16 A recent randomised control trial (RCT) highlighted significant challenges of applying both heart rate variability-biofeedback (HRV-Bfb) and mindfulness-based interventions (MBI) in a workplace context. 17
An interesting avenue of workplace wellbeing exploration is linked to harnessing the known benefits of nature exposure. Exposure to natural scenes mediates the negative effects of stress by reducing negative mood states and enhancing positive emotions 18 and such environments have proven efficacy in reducing stress.19–21 The underlying mechanism for this might be explained by Attention Restoration Theory (ART22,23) which posits that nature constitutes an environment offering physiological, emotional and attentional restoration more so than urban environments. 18 This is achieved through reduced directed attention, which takes up greater resources and effort and instead utilises involuntary attention, or ‘soft fascination’ capturing involuntary attention without monopolizing attentional channel capacity’. 24 Given the widespread agreement regarding the favourable effects of nature exposure, nature-based interventions (NBI) in the workplace have been proposed as a cost-effective approach to promote good health among employees. 25 Initial evidence suggests that exposure to natural settings such as parks during the working day has positive effects on mental health indices and cognitive ability. 25 However, access to such spaces may be impractical for many. This is, in part due to substantial increases in urbanisation, to the effect that, in 2018, over half (55%) of the world's population lived in urban areas – a proportion that is expected to increase to 68% by 2050. 26
These challenges to the implementation of workforce wellbeing initiatives may be even more pronounced in NHS workplace contexts given that staff seldom have designated, uninterrupted break times and access to private, appropriate and calm physical spaces in which to relax. Unfortunately, NHS staff are commonly faced with working environments characterised by noise, poor ventilation, lack of windows and no access to green space. Thus, there is a pressing need for new approaches to cost-effective as well as accessible interventions in stress-reduction in the workplace. 17
The rise of positive technology
Recently, human-computer interaction (HCI) researchers, designers, and technologists have started focusing on technology as a potential source of subjective wellbeing and positive support in their users’ lives. 27 This has led to the emergence of fields such as “Positive Technology” and “Positive Computing”, which aim to develop technology designed to foster well-being in individuals and groups. 28 Such practices typically rely on guided sessions delivered through applications such as Headspace or Smiling Minds for example, or leverage social networking features delivered through web or mobile applications. 27
In the context of the NHS specifically, the range of technology that might be used for wellbeing activities could be limited by factors such as organisational firewalls and variable access to WIFI. In a survey of NHS staff that were members of the British Medical Association (BMA) 29 over a third (32%) of respondents believed that they rarely had all the necessary IT equipment to perform their job to the best of their abilities or without disruption. A lack of computers/laptops, smartphones, tablets and access to Wi-Fi & broadband, with adequate speed and coverage was reported, and less than a quarter (22%) of respondents believed that IT systems at their place of work were fit for purpose. Moreover, over a third of this sample of NHS staff, inefficient IT was reported to be linked to their stress levels, and the impact on other NHS staff is likely similar. 29 Given that the dissatisfaction with current technological infrastructure within the NHS, perhaps wellbeing interventions delivered over Wi-Fi might be impacted by the equipment and infrastructure available to workers. As such an alternative, cost-effective technological solution independent of the existing infrastructure with built-in internet connect is a viable alternative for the delivering of wellbeing interventions.
VR for relaxation
Virtual Reality (VR) is becoming an increasingly popular technology, likely due to the more recent availability of affordable headsets that deliver high quality immersive experiences. 30 What makes VR so fascinating is its ability to induce “presence”. 31 Using VR, people can “experience the synthetic environment as if it was ‘their surrounding world’ (incarnation: the physical body is within a virtual environment) or can experience their synthetic avatars as if they were ‘their own body’ (embodiment: the physical body is replaced by the virtual one).’’ 32 Notably, these qualities mean that VR can give the sense of transporting a viewer to another place, in another physical form, irrespective of their physical environment in the real world and without much cognitive effort. Further, modern Head Mounted Displays (HMDs) are light-weight, portable, and can store downloaded content. This means they can store a range of experiences that can be accessed from any location, irrespective of workplace internet connectivity.
Whilst VR is often associated with gaming, many virtual environments feature contents that are associated with peaceful, pleasant, non-arousing nature-based sceneries (e.g. parks, islands, gardens). 33 Such experiences, which often are inspired by, or directly derive from, classical relaxation techniques are categorised as “relaxing VR” or rVR, and have been successfully employed to promote relaxation, reduce both cognitive and physical stress and show relevant potential in improving and regulating emotional wellbeing. 33 VR-induced relaxation states, achieved through lowered general arousal, are proven to have positive effects on cognitive overload. 18
Rationale
Although VR has been used effectively to promote relaxation and reduce stress
33
its application for these purposes in workplace settings are largely unexplored. A recent scoping review aimed to identify and evaluate studies that examined stress management and/or the promotion of relaxation in nonclinical populations through VR.
34
Of the 22 studies which eligible for inclusion, only four focused on stress in the workplace.35–38 The authors
39
also conducted an initial feasibility study to compare the effect of two VR relaxation interventions on measures of physiological arousal and affect, as compared to a control condition. The results suggest VR interventions to be promising in workplace contexts given the small number of studies that focus on VR for stress in the workplace, there remains a gap in the literature. Further, to our knowledge, no studies assessing the efficacy of VR for stress reduction in the workplace have focused on frontline healthcare professionals in the NHS. Given that NHS staff are an integral workforce in maintaining the health and wellbeing of the UK population and disproportionately affected by workplace stress, particular attention to this group is warranted. Accordingly, the aim of this study is twofold:
To explore the potential propensity of a short virtual reality (VR) nature experience, delivered during the workday, to induce positive mood states NHS clinicians. To provide an initial indication of the suitability of VR for use with NHS clinicians in a fast-paced work environment.
Method
Participant recruitment
Participants were NHS staff working in a fast-paced trauma service. All staff within the service were invited to take part in a 10-min relaxation experience within virtual reality via an email distribution list. Information was provided about the nature of the study which focused on it being a relaxation experience using VR. An email was sent to all staff members which included the following: “You are invited to take part in a short (half an hour in total) relaxation session. This session will provide you with a break from your workday and, via a virtual reality headset, you will be transported into a relaxing, natural environment (a meadow). We will also take simple measurements of your heart rate before and after the session and ask you to complete some short questionnaires”. Staff were provided written informed consent a week before the experience and had the opportunity to ask questions before participating. Staff were asked to complete basic demographic data along with information about their job role and baseline information about their current self-care practices. All participants were made aware that participation was voluntary and they could stop at any time without explanation.
Context
Staff were able to choose from a number of available time slots that were sent to them via email. Additionally, participants were asked to get in contact if they wanted to take part but were unavailable at the proposed time slots as this could be accommodated for. Sessions took place during usual working hours in a designated wellbeing room on the hospital site where staff worked. The majority of sessions took place during a particularly stressful two-week period for the service and staff. This was identified as a time when staff wellbeing warranted particular attention. Further sessions took place over the 5-week period that followed to maximize participation opportunities for staff. Staff were not required to do any preparation for the session and were able to eat and drink as they normally would.
Procedure
Upon arrival to their session, participants were given a wearable heart-rate monitor (Fitbit) and their initial heart rate was recorded (HR1). Participants were then left alone in the room for a period of 10 min, allowing them to rest in passive state of relaxation without any direct intervention. The purpose of this was to identify a resting baseline heart rate against which VR intervention could be compared. Further, participants responded to the baseline questionnaire, via pen and paper, to capture participants self-reported mood state.
The researcher then took some time to explain the VR equipment, the specific experience – the virtual meadow – and the interactivity available within it. The researcher guided participants to navigate the experience, allowing them to familiarise themselves with the controls and ask any questions. When participants felt comfortable with the technology (usually after around 5–10 min) the researcher took another heart rate measure (HR2) and participants began a 10 min, uninterrupted, VR session. All participants remained seated throughout the experience, but were able to explore and interact with the environment, using the controllers. Participants level of interactivity with the environment differed, with some opting to navigate through the whole scene, adapt the environment (for example, by planting “virtual trees” or changing the weather) and others did not move around, but instead spent the time looking around the scene and listening to the peaceful sounds (gentle music, sounds of animals). The researcher remained present in the room with the participant for the whole session, and was thus available for questions and support.
When the 10-min time period ended, participants were gently notified by the researcher and they removed the VR headset. Participants’ heart rate was then taken immediately, for the third time (HR3) and they filled in the follow-up questionnaire to once again capture their emotional state as well as their perceived acceptability of the experience. Open written and verbal feedback about their experience was also captured.
Technical apparatus
The VR experience was administered using a virtual reality head mounted display, the Oculus Go, with Single Fast-Switch LCD 2560 × 1440 screen. The Oculus Go has in-built speakers, meaning no additional audio hardware was required in this study and it was paired with a single wireless controller. The controller requires only one hand to operate, and can be used equally well by left- or right-handed users. The VR experience selected was Nature Treks VR, developed by Greener Games (https://naturetreksvr.com/). Specifically, the “Green Meadows” single-user scene option within Nature Treks was administered to all participants.
Measures
Participant characteristics
A demographic questionnaire gathered information about participants; age, sex, ethnicity, first language, NHS grade, working hours and responsibilities. Further, participants’ experience with computers and VR systems was assessed using the Independent Television Company SOP Inventory, (ITC-SOPI40,41). Here, participants indicated their (1) Experience with computers (answer choices were: none, basic, intermediate, and expert); (2) Knowledge about 3-D images (none, basic, intermediate, and expert); (3) Frequency of playing video games (a) never, (b) occasionally (once or twice a month), (c) frequently, but less than 50% of the days, (d), 50% of the days or more); (4) Knowledge about VR (none, basic, intermediate, and expert).
Heart rate
Heart rate (BPM) was measured using a wearable Fitbit Charge 2, which participants wore on their wrist throughout the entire 30 min session. Heart rate readings were recorded at 3 time periods; ‘Time 1’ (T1) upon arrival to the session, ‘Time 2’ (T2) after a ten minute rest period, and ‘Time 3’ (T3), immediately after the virtual reality experience. Recording participants’ heart rate across these three time points allowed us to identify participant's baseline heart rate following a period of rest with no intervention, which could then be compared to their heart rate following exposure to the VR experience.
Emotional state
The Visual Analog Scale (VAS 42 ) was employed to evaluate the intensity of different emotions before and after the VR intervention. As in previous studies, 43 we used a brief (7 item emotion) version of the original (16 item emotion) measure to reduce the time burden on participants. Participants were asked to rate on a 1–7 points Visual Analog Scale (1 = not feeling the emotion at all; 7 = feeling the emotion extremely) how they felt at that moment for the following emotions: happiness, sadness, anger, surprise, anxiety, relaxed/calm, vigour/energy.
Acceptability of the intervention
To collate feedback on the experience overall, we administered an adaption of the Credibility/Expectancy rating scale 44 following the VR experience. The adapted questionnaire was composed of 4 items which participants rated from 0 (‘not at all’) to 10 (‘very much’). The items assessed participant's: level of satisfaction with the intervention; how logical and recommendable they thought the intervention was; the extent to which the intervention was considered useful for practicing mindfulness; and the extent to which the participant found the intervention difficult to manage or aversive.
Qualitative feedback
Participants were provided with open space to write any comments or feedback they had about the experience at the end of the session. Additionally, the researcher made a note of any spontaneous verbal feedback.
Other measures
Additional data were collected which pertained to participants’ self-care strategies, trait mindfulness and sense of presence following the VR experience. This data will be presented in a separate paper.
Ethical considerations
All participants were aware of the potential risks of using VR technology, and gave fully informed written consent to participate. The nature of the experience and the use of the equipment was explained to participants in detail before they entered the experience, and participants were encouraged to ask the researcher any questions they had. Participants were informed that they were to remove the HMD straight away should they experience any feelings of nausea, anxiety or if they felt uncomfortable in any way. Participants were also aware that they could stop the session at any time, without providing a reason.
Ethical approval was granted by the service's research panel, with approval from CNWL's Chief Psychologist and following guidance from NHS Health Research Authority. The study was carried out in line with BPS Code of Human Research Ethics. 45
There are cautionary measures that need to be taken when using VR. For example, VR environments need to be carefully designed in order to minimize sensory conflicts (e.g. between visual and vestibular systems) to avoid cybersickness46,47 and for this reason a gentle nature experience was selected. Participants were screened to ensure they did not have any medical contraindications (e.g. epilepsy) and remained seated in a comfortable position for the duration of the experience, to minimise the chance of suffering an injury through reduced vision whilst wearing the HMD and to also ensure that the equipment was not damaged. During the experience the researcher (CLK), a cognitive neuroscientist and expert in VR technologies, stayed with participants throughout. The researcher was experienced in administering VR experiences and ensured that the HMD was fitted correctly and comfortably. The researcher checked for the comfort of participants and adjusted accordingly if needed. Several measures were employed to ensure that no contagious conditions were transmitted through the use of shared equipment. Firstly, participants were screened before partaking in the experiment to ensure that they did not have any conditions/infections that would be transmissible by the equipment (e.g. impetigo, conjunctivitis). Secondly, a wipeable face mask was attached to the inside of the HMD, which the researcher disinfected, using disinfectant wipes, between every use. Additionally, a Psychologist (JSA) was available at all times should any adverse effects of the experience occur.
Data analysis
Descriptive statistics were calculated to explore demographic characteristics, sense of presence, and acceptability of VR. Whether or not the data met the requirements for the performance of a parametric test was established. Paired t-tests were used to assess the effects of VR mindfulness intervention on emotional state outcome measures. A one-way repeated measures ANOVA was conducted to assess the effect of time point on heart rate. All analyses were conducted based on completers using IBM SPSS statistics 23 for Windows.
Results
Sample characteristics
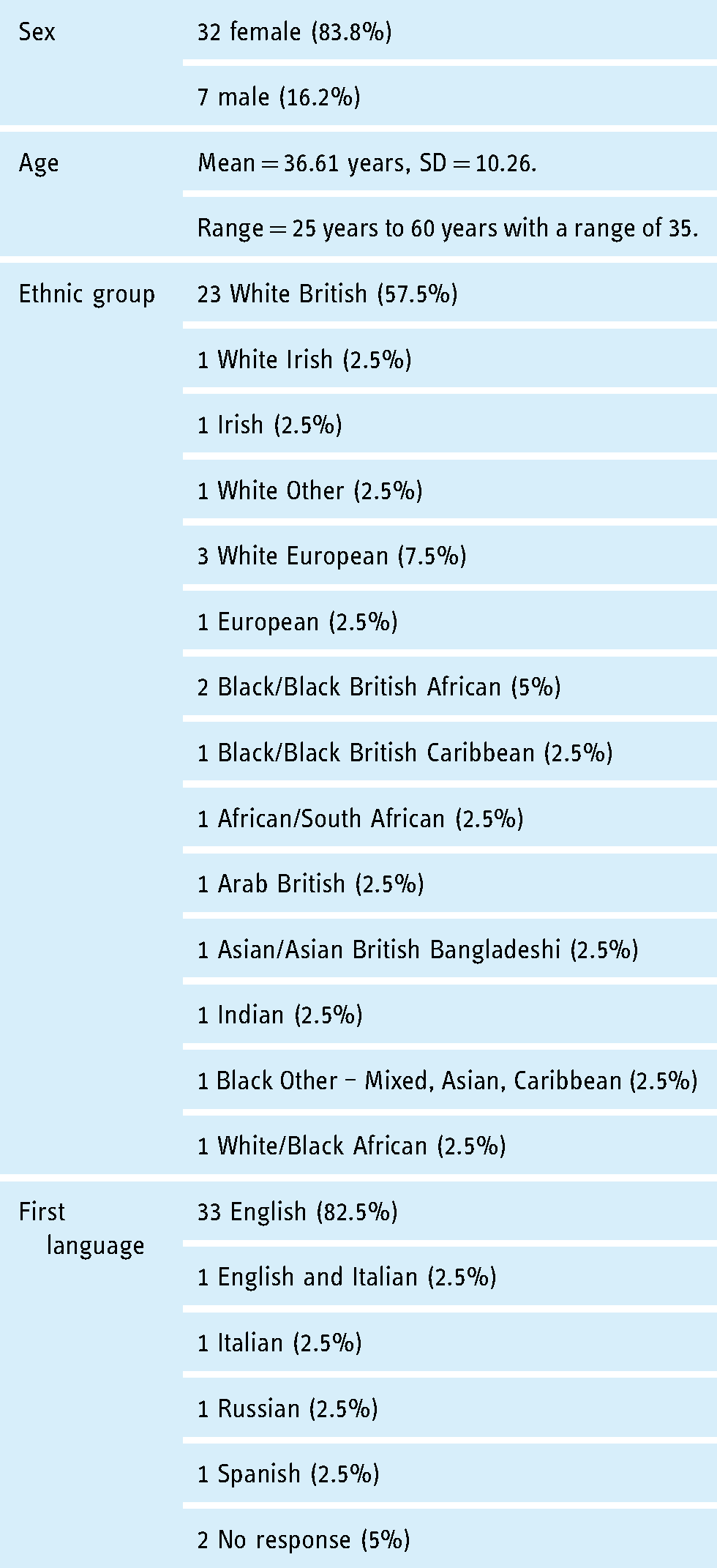
49 clinicians signed up to partake in the study, however, 10 participants did not attend their session and did not provide any reasons for non-attendance. The final sample constituted 39 clinicians, the demographic profile of which can be seen in Table 1. The mean age of participants was 36.61 years (SD = 10.26) ranging from 25–60. 32 participants were female (83.8%) and 7 male (16.2%). The sample represented a broad range of staff across pay bands 4 to 8 reflecting both junior and more senior clinicians. The majority of participants worked full time and 38% of the sample reported supervisory responsibilities. As can be seen in Table 2, most participants reported an intermediate amount of experience using computers and basic (little) or no knowledge about VR and 3D images. Moreover, most participants did not usually play video games, reflecting a staff group that mainly used computers but had relatively little experience of gaming or VR.
Participant characteristics.
Experience with computers and VR systems.

Effect of VR on emotional state
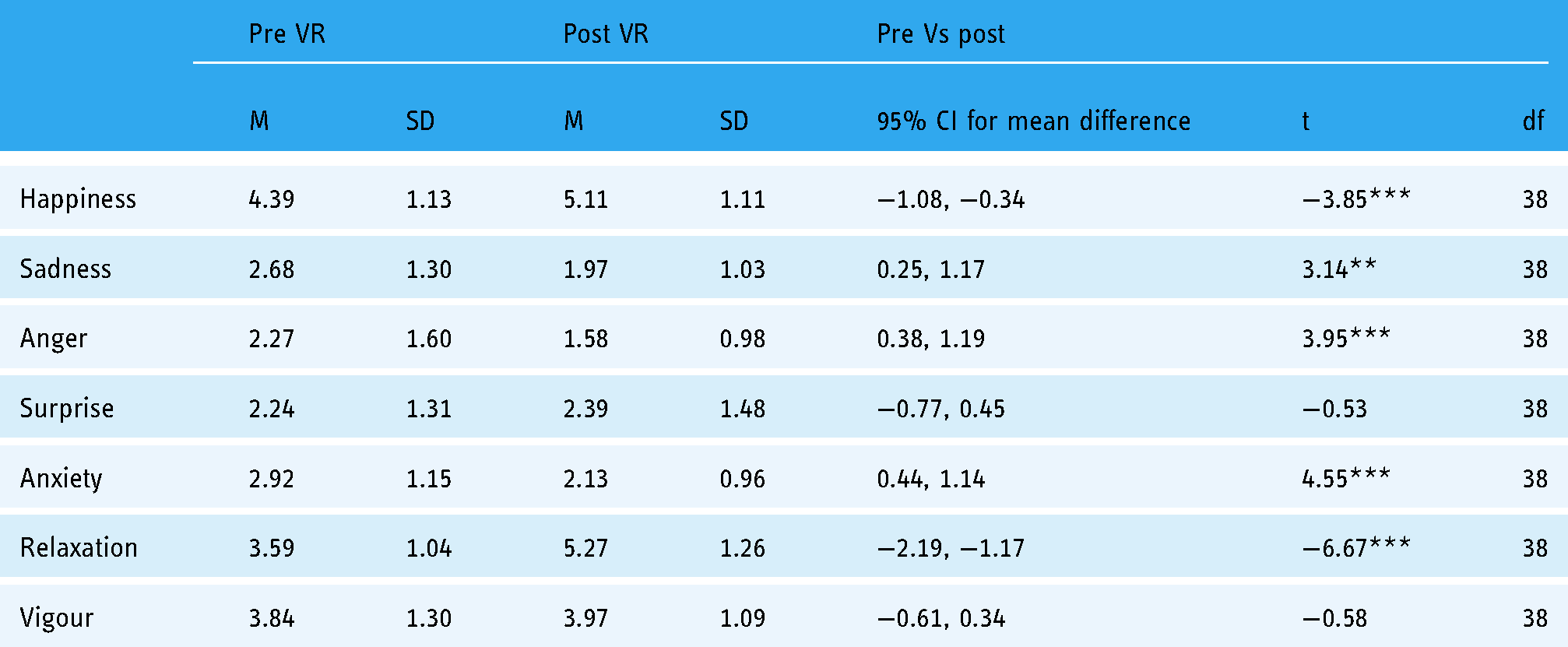
Results revealed significant changes from pre- to post-VR exposure on 5 of the 7 emotional state outcomes (see Table 3 for details). Specifically, paired t-test comparisons showed that, following exposure to the VR experience, the participants reported significantly increased levels of happiness (t(38) = −3.85; p < 0.001;) and relaxation (t(38) = −6.67; p < 0.001) and significantly lower levels of sadness (t(38) = 3.14; p = 0.003), anger (t(38) = 3.95; p < 0.001) and anxiety (t(38) = 4.55; p < 0.001) as shown in Figure 1. No significant differences in reported levels of surprise (t(38) = −0.53; p = 0.603) or vigour (t(38) = −0.58; p = 0.566) were found.

Percentage change in emotional states following VR experience.
The effect of VR on emotional state note: M = mean; SD = standard deviation; t = t-value; df = degrees of freedom; CI = confidence interval. *p < 0.05, **p < 0.01, ***p < 0.001.
Effect of VR on heart rate
A one-way repeated measures ANOVA was conducted to see if there was a significant effect of time point (arrival, pre-VR, and post-VR) on heart rate. Mauchley's test indicated that the assumption of sphericity had been violated χ2(2) = 7.44, p = 0.024, therefore, degrees of freedom were corrected using Huynh-Feldt estimates of sphericity (ε = 0.83). The results show that there was a significant main effect of time on heart rate (V = 0.38, F (2, 33) = 10.02, p < 0.001).
Post hoc comparisons using bonferroni correction revealed that the heart rate significantly reduced between time 1 (M = 75.4, SD = 15.64) and time 2 (M = 69.20, SD = 11.62) (p = 0.016) and again between time 2 and time 3 (M = 64.91, SD = 8.41) (p = 0.025) as shown in Figure 2.
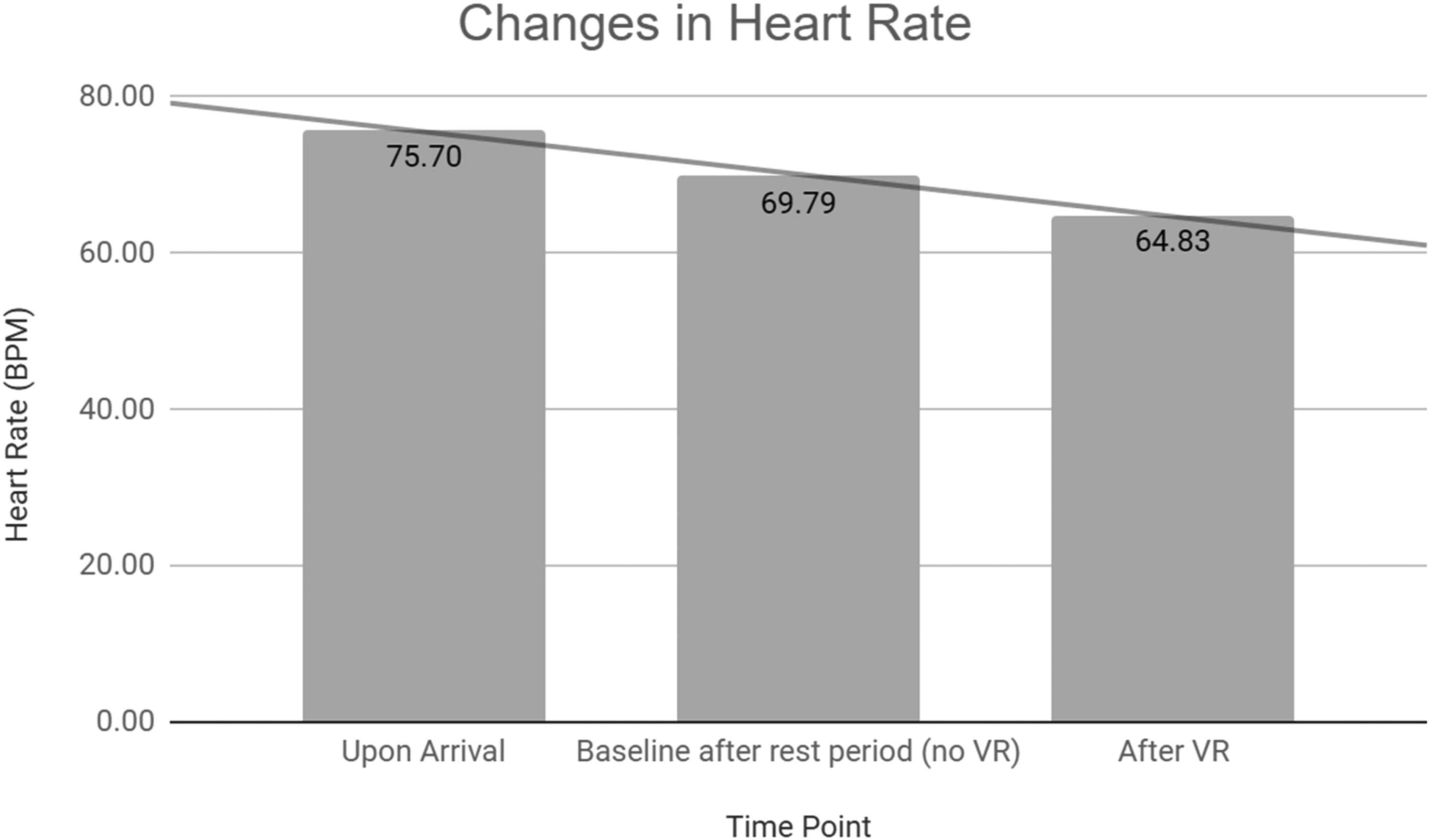
Mean heart rate (BPM) at time 1 (upon arrival), time 2 (after rest) and time 3 (after VR experience).
Acceptability of the intervention
Inspection of Table 4. reveals participant ratings (where zero = “not at all” and 10 = “very much”) pertaining to the acceptability of the VR intervention. Descriptive statistics indicate participants experienced a medium to high level of satisfaction with the experience, and low levels of aversion.
Reported satisfaction with the VR experience (where zero = “not at all” and 10 = “very much:”). M = mean score, SD = standard deviation of the mean.

Qualitative feedback
In line with quantitative data, increased feelings of positive emotions such as relaxation, calmness and happiness were apparent in the qualitative feedback. Many participants described the experience as “great”, “amazing”, “very relaxing”, “calming and peaceful” and expressed that they “feel calm now”. Furthermore, as well as reporting increases in relaxation and calmness, participants wrote about a decreased feelings of stress, for example that the experience took their “mind away from stress”.
Multiple participants suggested that it was a “really good experience during the working day just to take a few minutes out to relax” and would welcome this type of experience as a regular part of their work day. One staff member expressed that they would “really love to be able to do this during my workday” and another wrote “That was amazing, I feel great. That three times a day would be a game-changer.”
The experience also prompted staff to reflect on their overall wellbeing at work. One participant wrote “great experience. We need more of this and more time to think about our wellbeing. Good for patients and staff. I think a regular, varied VR could be beneficial to manage stress and help us to feel calmer. Enjoyed it. Thanks!”
Furthermore, many expressed that the intervention “would be great for mindfulness” and overall wellbeing at work, for example one participant wrote “Thank you! I could imagine this being really helpful to promote wellbeing/relaxation and mindfulness”. This was also the case for participants who usually found mindfulness practices difficult, expressing that “I don't find mindfulness helpful at all but I did enjoy this experience.”
The experience conjured memories of nature experiences that participants had had in real life, with one participant writing “It reminds me of being at the Isle of Aaron, my favourite place in the world. I could stay in here forever.” Notably, participants also spontaneously expressed that the experience motivated them to seek nature experiences in real life more often. For example, one participant wrote “I really liked it. It has reminded me to spend a bit more time in the real countryside whenever I can”.
Discussion
Taken together, our findings lend support to the growing body of literature positing that VR can be an effective tool for the promotion of relaxation and the reduction of stress. 33 More specifically, we add to the few studies which examine the promotion of relaxation in the workplace in nonclinical populations through VR.
The first aim of this study was to explore the potential propensity of a short virtual reality (VR) nature experience, delivered during the workday, to induce positive mood states NHS clinicians. Self-reported measures of affect revealed that the VR experience was associated with a significant increase in feelings of happiness and relaxation, and significant decreases in feelings of sadness, anger, and anxiety. No significant differences in surprise or vigour were observed. Additionally, the VR experience was associated with a significant reduction in participant's heart rate.
The second aim of this study was to provide an initial indication of the suitability of VR for use with NHS clinicians in a fast-paced work environment. The sample constituted people with an intermediate amount of experience using computers and basic, little or no knowledge about VR, 3-D images or gaming. Despite their limited and varied experience of technology, participants reported overwhelmingly high ratings of satisfaction with the experience. Measures of acceptability revealed that participants found the experience logical, recommendable, and useful for practicing mindfulness. Additionally, participants reported low levels of aversion or difficulty.
Qualitative feedback supported the quantitative results, and provided a deeper understanding of participants thoughts and feelings about the experience. Participants reported feeling more relaxed and positive following the experience, and many indicated that they thought that access to this technology, on a regular basis, during their working day would be of benefit to their overall wellbeing at work. An unexpected finding was that participants spontaneously expressed increased motivation to make positive behavioural changes outside of their working day, for example, to take more time to focus on their wellbeing and to spend more time in natural settings. Participants’ self-reported motivation to spend time in nature following the VR experience supports suggestions that technological nature may not just be a mere replacement of real nature, but rather be part of the solution to increase human-nature interactions. 48 It has been suggested that immersive nature may do this by (1) prolonging the positive effects of nature-interactions after leaving an outdoor natural setting; (2) providing access to nature for individuals who may not be able to access it directly; (3) increasing feelings of connectedness with the natural world and (4) eliciting greater awareness of environmental issues and sustainability. 48
Limitations and recommendations for future research
An obvious limitation of the present study was that there was no control group to which the VR intervention could be compared and, thus, a causal relationship between the VR experience and participants’ mood could not be established. A Randomised Control Trial (RCT) would address this, as well ensuring that a more representative population sample than in the current study. In this study participants comprised of mostly middle-aged white British females, reflecting the demographics of the staff group working within the trauma therapy service. The self-selected sample could have resulted in a ‘healthy worker bias’, whereby those most interested in their wellbeing and self-care chose to take part. In future studies, feedback should be sought on why the experience was not taken up by some staff and to seek a more representative sample across a larger sample of healthcare professionals, attending to possible differences between the sexes.
The limitations of self-reporting internal states were partially mitigated by also measuring heart rate – an objective indication of physiological arousal. Although reductions in heart rate are associated with relaxation, it is possible to feel happy and content but have higher heart rate due to engagement and/or interactivity. In retrospect, other biometric data such as heart-rate-variability, galvanic skin response or cortisol levels would have provided a much better objective indication of physical stress. Future research would benefit from utilising these methodologies.
A longitudinal approach would present the opportunity to investigate the effects of regular VR relaxation during the working day on a multitude of factors such as staff retention and work satisfaction, as well as other possible benefits such as generalisation of relaxation practices outside of VR. Of particular interest is to observe whether reports that participants felt motivated to immerse themselves in nature, outside of work, would manifest in positive behaviour change. This approach would also elucidate to what extent such effects persist over time.
Implications
This study contributes to the emergent body of literature investigating the efficacy of VR for the promotion of workplace wellbeing. Specifically, the results of this study provide the first indication that a short VR relaxation experience may be an effective tool to mitigate workplace stress in NHS contexts. We hope that our work sparks further interest and research activity in this area, and opens a fruitful line of investigation. If future research replicates our findings, the employment of this, and similar interventions, could have far-reaching implications for not just the health of the NHS and its patients, but for other healthcare systems, public services and commercial organisations.
Conclusions
In summary, the findings of the study indicate that a short VR relaxation experience, administered during the working day, might be able to induce positive mood states NHS clinicians working in a high intensity trauma service. The experience was easy to use and a positive experience for the majority of participants, and took less than 30 min overall which made it feasible and accessible to this population. Our results suggest that VR for workplace wellbeing, particularly for NHS staff, is a fruitful avenue of investigation that warrants further exploration.
Footnotes
This study was a collaboration between The Fred Company, and Central and North West London CNWL Foundation Trust. We would like to thank Rosie Collins, Lucy Wood and Ross O’Brien for their assistance and guidance in this research.
Author contributions
Both authors (JSA and CK) researched literature and conceived the study and were involved in protocol development, assessing whether ethical approval was required, patient recruitment and data analysis. JSA and CK wrote the first draft of the manuscript. Both authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial registration
Not applicable, because this article does not contain any clinical trials.
Guarantor
JSA.