
Abstract
Objective
Evidence of virtual reality's (VR) efficacy in hospital settings coupled with the rise of inexpensive consumer devices have led to the development of social virtual reality (SVR) applications being incorporated in hospital settings. SVR provides opportunities for social interactions in virtual environments, allowing individuals to virtually socialize, regardless of geographic or mobility constraints. However, the full range of potential applications and the challenges of deploying SVR in hospital settings remain unexplored. We conducted a scoping review to characterize SVR applications studied in hospital settings to better understand SVR use for inpatient populations overall and in preparation for a National Institutes of Health (NIH)-funded project investigating SVR use with a specific clinical population.
Methods
In this scoping review, we searched MEDLINE, Embase, Scopus, APA PsycInfo, CINAHL, IEEE, and ACM Digital Library. After screening 2334 studies and reviewing 146 full texts, we identified 12 studies as eligible for analysis. Eleven of the 12 were published in the past 7 years, with none older than 12 years.
Results
As this is an emerging field, many publications were case or pilot studies, with small sample sizes ranging from 3 to 200 participants, and with mean participant ages that ranged from 9 to 75 years. Patient populations included those with stroke, cancer, COVID, as well as other health conditions.
Conclusion
Discussion of privacy and accessibility concerns was limited, as was the reported influence of SVR on measures associated with inpatient medical treatment (such as, adherence to clinical treatment while in the hospital while in a SVR intervention), which we highlight as critical issues for SVR's clinical use. We discuss our findings in the context of potential future directions for research in this area.
Background
The health applications of virtual reality (VR) have been widely studied for decades, such as for its use in pain control among burn patients, 1 children with acute burn injuries, 2 adults undergoing surgical drainage, 3 adults with schizophrenia,4,5 and people with autism spectrum disorder.6–8 VR has also been studied as a tool in the treatment of posttraumatic stress disorder following the World Trade Center attacks of 11 September 2001,9,10 management of various phobias,11–13 dental care and anxiety,14,15 chronic pain management, 16 and among patients receiving palliative care.17–19 Increasingly, the use of VR applications has also been studied with older adult populations20–23 to address exercise effort, anxiety, enjoyment, mood states, loneliness, and social engagement, which have been linked to health outcomes in older adults.
VR can be experienced alone, without others present in the physical or virtual environment, but VR also allows for multiple individuals to communicate and socialize in virtual environments together, even when apart in the physical world. For example, there are four ways VR can be experienced: alone physically and alone virtually (i.e. solo VR experiences); together physically and alone virtually (e.g. when two people play different games in their own headsets in the same room), alone physically and together virtually (e.g. when patients connect through social virtual reality [SVR] with a friend or family member at home), and together physically and together virtually (e.g. when participants in a hospital room play a game together in VR). Individuals are represented by avatars, which are the digital representation of users in virtual environments. 24 Avatars are controlled by the user's movements and can be customized or personalized to resemble the user through appearance. 24
The rise of consumer devices and decrease in prices has made VR more popular and easier to use with others. SVR allows users to interact with friends, strangers, or even computer-programmed agents to play games and converse in virtual environments, regardless of geographic or mobility constraints that may prevent face-to-face interaction. The broader availability of SVR affords a range of possibilities to improve experiences for hospitalized patients. For example, SVR applications may help address problems such as social isolation or loneliness that many hospitalized patients experience.
Existing research has examined health-relevant outcomes from SVR interventions, identifying effects on pain, well-being, and quality of life.25–27 For example, one study found increased pain tolerance for an induced pain task among young adults in a lab setting when participants used SVR compared to solo VR. 27 Another study found a significant increase in quality of life and social engagement for older adults in residential care homes throughout a 6-week virtual tourism pilot study with social elements. 25 Lee and colleagues explored the link between SVR game involvement and well-being and social connectedness. 26 In these studies, participants’ prior experience with VR ranged from current users to first-time users. The locations of studies also varied widely, including lab settings and residential care settings.
To better understand the use of SVR across diverse settings and populations, and provide insight into potential future uses, we aimed to conduct a scoping review. As VR technology continues to develop, systematic and scoping reviews have provided insight into recent applications. Scoping reviews are appropriate when aiming to identify knowledge gaps and understand how research is currently being conducted in a particular area. 28 For example, Dhar and colleagues’ 2023 scoping review examined VR use in medical education and clinical care focusing on studies published after 1 January 2017. 29 Such reviews shed light on advances in a given domain and help to identify key knowledge gaps that should be addressed by future research. We conducted a scoping review in preparation for a National Institutes of Health (NIH)-funded project investigating the use of SVR among older adult trauma patients to provide social support while they are hospitalized and away from family and friends. Our scoping review examines SVR with clinical populations in the hospital setting. We characterize the various SVR applications studied in hospital settings for inpatient populations and identify key knowledge gaps that should be addressed by the research community.
Objectives
The literature in this field is growing but still not sufficient for a systematic review. Thus, we conducted a scoping review of SVR applications in inpatient hospital settings. Understanding which SVR applications have been studied in the inpatient setting (e.g. in hospitalized patients) can lead to new insights into intervention successes, such as improved social connection, and future directions, such as targeting understudied populations. We chose to focus solely on inpatient settings because of their unique impact on socialization and connection, and the challenges that come with the hospital environment. For example, patients are often hospitalized as inpatients for days at a time and are often geographically distant from their normal social network. In addition, while inpatient settings may offer visiting hours, these hours are often limited making it difficult for many family members (e.g. those with jobs) to visit a hospitalized family member. Patients are admitted to hospitals for different reasons than other sites such as senior living centers and may have more acute conditions. In addition, hospitals offer particular challenges for implementation such as turnover of patients, staff changes, the need to accommodate emergency interventions, and other aspects that differentiate it from a more residential setting. Interventions that can succeed in a hospital setting will need to solve problems that may also apply, if less intensely, to other settings, so we focused on how these interventions were implemented, issues that arose, and outcomes that were measured to understand what findings might be generalized and which might be specific to the in-patient experience.
VR devices typically include a wearable head-mounted device and a set of hand controllers; people's movements are tracked with the wearables and rendered within the virtual environment, creating a higher sense of presence and allowing for physical interactions like game play.
30
We did not include tablet-based or video-conferencing interventions such as Zoom because they do not provide virtual embodied experiences.31,32 We defined VR as an immersive experience that includes embodied behavior rendered in a virtual environment. To provide a more unified definition from the literature, we aligned our VR definition with Miller's and Bugnariu's virtual environment characteristics by level and aspect of immersion.33,34 Specifically, we included VR that qualified as moderate-to-high levels of immersion on at least four aspects in their outlined virtual environment characteristics.
34
We outline our aligned VR definition as follows:
Inclusiveness (some to limited signals of presence in the physical world) Extensiveness (more than one sensory modality) Surroundings (extended or surrounded field of environment view, which included computer monitors but not tablets for size difference) Vividness (moderate-to-high fidelity, visual/color resolution, and detail in simulated environment) Matching (motion capture and matching visual experience with proprioceptive feedback based on movement)
The scope of our social component for SVR eligibility entailed interacting with others (humans, computer agents, or virtual avatars) in a VR environment. We did not include studies where participants were physically together in a space but alone in a virtual environment.
35
We included studies where participants were virtually together with others, whether they were physically alone or not.
Studies that evaluated social training experiences, for example, interventions designed to improve social skills or treat social anxiety disorder, were also not included because this literature has been previously reviewed systematically.36,37 For example, there are existing systematic reviews, comprehensive reviews, and case studies on augmented reality and VR interventions for people with autism spectrum disorder.38–40
We categorized an intervention as taking place in the inpatient setting if a study clearly described a hospitalized population participating in a SVR intervention. Studies on aged care or assisted-living populations that used technological interventions for social purposes have also been recently examined in a scoping review 41 and a systematic umbrella review. 42 Therefore, we excluded studies on aged care and assisted-living populations from our review.
Within our scoping review, we proposed eight research questions (RQs):
RQ1: How is the healthcare field using SVR in hospital settings? RQ2: What types of empirical study designs have been employed to study SVR within hospital settings? RQ3: How do social interaction interventions differ for inpatient populations by study design? RQ4: What types of virtual environments have been used by inpatient populations, including different consumer or custom designs? RQ5: How do virtual environments impact physical-world social interactions for inpatient populations? RQ6: Does SVR influence therapeutic or clinical treatment outcomes? RQ7: What outcome variables have been used to measure the effects or quality of social interactions across inpatient populations? RQ8: What are the barriers to using virtual environments in the hospital setting?
Methods
Search process
We searched the following databases: MEDLINE (Ovid), Embase (Ovid), Scopus (Elsevier), APA PsycInfo (EBSCOhost), CINAHL (EBSCOhost), IEEE Xplore, and ACM Digital Library. We used a combination of controlled vocabulary and keywords to represent the concepts of VR and social interactions. Our combined database search strategies are detailed in Supplemental File 1. For nonbiomedical databases, we included healthcare, therapeutic, and medical terms to focus results on the healthcare field. The list of all included terms is available in Supplemental File 1 (Combined Database Search Strategies). We limited our results to English-language studies. Only peer-reviewed empirical studies were included to help verify credibility in our analyzed articles. Other publications, such as conference abstracts, dissertations, case studies, protocol papers, and editorial letters, were removed because these publications were shorter in length and did not allow for the same level of data extraction. We also did not include any gray literature. We used the Covidence software for publication storage and as review tool management. Covidence helped identify duplicate publications, and automation tools were used to help screen publication credibility.
All records were screened for eligibility by two independent reviewers at the title/abstract level. Consensus discussion settled any conflicts regarding inclusion or exclusion. At the full-text level, studies were reviewed by two independent reviewers, and 12 studies were deemed eligible. These 12 studies underwent full data extraction on study characteristics by one reviewer. The other reviewer involved in the full-text level review also verified the tables and documents to ensure the validity and accuracy of the extraction's results, and these two reviewers addressed any discrepancies through discussion to reach consensus. The search and screening process took place from October 2022 to October 2023. This scoping review used secondary data from peer-reviewed publications and did not work with human participants. A patient consent form was not required for this research.
Eligibility criteria
Our scoping review focused on peer-reviewed empirical studies. We included only inpatient populations. Our reasoning was that the hospital setting would greatly influence what intervention styles were possible and desirable, such as affiliations between hospitals, daily patient routines, and available meeting times/spaces with friends and loved ones. Outpatient populations, such as those treated with home-based interventions, were excluded. Additionally, studies were removed if the intervention being tested was insufficiently described (e.g. did not provide sufficient information to determine its eligibility status for current review), did not take place in a virtual environment or virtual world, or was a training or education session rather than an intervention. Our eligibility criteria are bulleted below, and Figure 1 summarizes the study identification and selection process in a flow diagram modified from the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram. We also included the PRISMA extension for scoping reviews (PRISMA-ScR) checklist document in Supplemental File 2.43,44
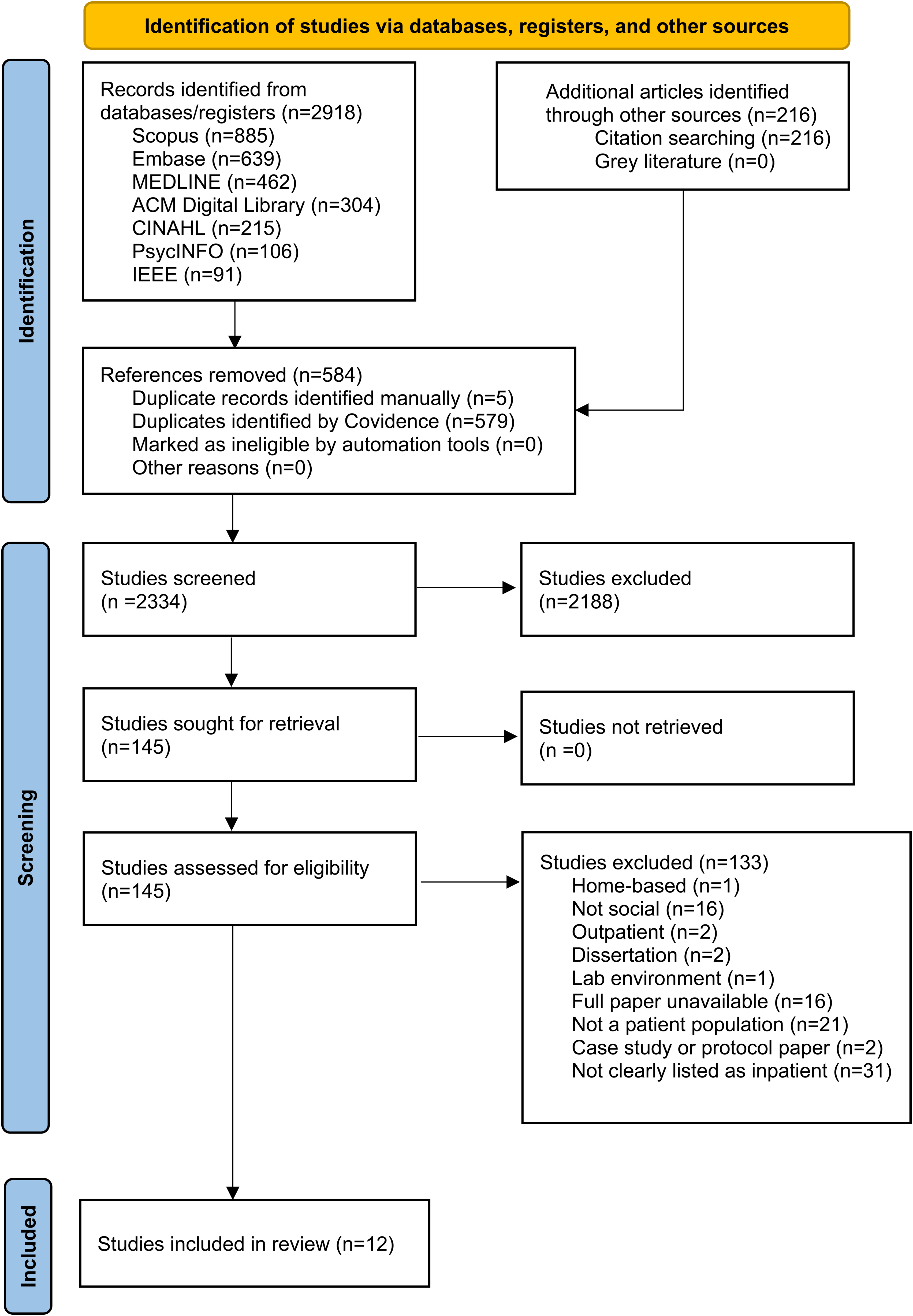
Study identification and selection process flow diagram modified from PRISMA.44
Inclusion criteria:
English-language paper Peer-reviewed papers An empirical study Includes SVR (SVR = social interaction, support, presence, or action within VR), such that patients are interacting with others (humans or agents or avatar) SVR interventions used for patient populations (used for therapeutic intent for people with a diagnosis [at home, hospitals, hospice, nursing homes, long-term care]); inpatient Full paper available Completed data collection Social interaction is the intervention Non-English-language paper Non-peer-reviewed papers, dissertations, theses, and conference proceedings/abstracts, editorials, gray literature Systematic or meta reviews (tagged for literature review) “Social” is used for social media platforms that post primarily 2D content, not VR, virtual worlds or games; No SVR (SVR = social interaction, support, presence, or action within VR) Does not describe SVR use in clinical contexts; not clearly listed as inpatient Cannot find full text Incomplete data collection: protocol papers (with future tense—indicating that data has not been collected), case studies Social interactions that are training experiences, such as interventions that teach social skills or are designed to aid in social interaction styles
Exclusion criteria:
Results
Overview
The initial set of searches produced 2148 records after removing duplicate records. We also conducted a reference-chasing process based on records that met the final eligibility criteria, adding 186 records for a total of 2334 records screened. Figure 1 shows the preferred reporting items for systematic reviews and meta-analyses flow diagram for details of record disposition and reasons for exclusion at the full-text level.
The data extracted from each article included study design, location for intervention use, use/context, devices used, intended intervention dosage, consumer VR type used, number of participants, participant age, participant inpatient diagnosis, participant gender breakdown, and intervention social interaction partner. Most of the studies were published within the past 7 years (n=11), and the remaining study was first published in 2012. Intervention locations for inpatient populations varied, including rehabilitation departments, children and pediatric hospitals, and occupational therapy units. Participant age groups ranged from hospitalized children and young people to elderly patients. Table 1 lists the study intervention patient population and intervention purpose, and Tables 3, and 4 list the detailed findings from our data extraction.
Study patient population characteristics.

VR: virtual reality.
RQ1: How is SVR being used in the hospital setting?
The manner in which SVR was incorporated in various clinical settings for inpatient use is summarized in Table 1. Use cases include rehabilitation purposes, such as COVID-19 rehabilitation, and for care continuity, such as reducing social isolation during frequent hospitalization.45,46 In addition, SVR was also used in tandem with other therapies, like therapeutic group singing interventions for people with spinal cord injury.
47
Specifically, there were three main categories of use across the 12 studies:
Rehabilitation purposes (related to stroke, COVID-19) (n=6) Music therapy delivery style (for motor function and respiratory/vocal exercises) (n=2) Connecting patients to environments outside the hospital (school, home) (n=4).
Study populations varied widely, ranging from hospitalized children48,49 to older adult patients with myasthenia gravis.
50
Within these different patient populations, their social interaction style and partners varied widely; from connecting with school classmates
45
to playing multiplayer rehabilitation games with other adult patients in the same hospital who were diagnosed with hemiparesis after a nontraumatic brain injury.
51
See Table 2 for more information.
Study design and intervention context.

RQ2: Types of SVR study designs employed with study descriptions
Study designs varied and included formative assessments, multisession evaluations, preliminary clinical studies, proof-of-concept processes, design studies, descriptive studies, open trials, interview studies, and experiment studies. The three most common were experiments, interview studies, and design studies (see Table 3 for more information).
Social virtual reality devices, types, and interaction.

HMD: head-mounted display; VR: virtual reality.
All 12 studies were published in the past 10 years, with 11 published in the last 7 years. Participant ages ranged from 9 to 70 years, and sample sizes ranged from three to 35 participants. Only one of the 12 extracted studies provided a breakdown of participant race and ethnicity. 49 Intervention applications ranged from social games for inpatient stroke participants’ rehabilitation, using SVR to connect pediatric inpatients with their family members at home, and music therapy sessions for people living with spinal cord injuries.47,48,52,53
RQ3: Social interaction by population/RQ4: Virtual environment setting by intervention
The SVR intervention designs differed by intervention purpose and patient population. For example, arm rehabilitation SVR interventions focused on gamified arm tasks with a wearable device, such as a Bimeo arm rehabilitation system. These interventions were multiplayer and involved playing with others. These virtual environment games were both competitive (classic Pong game) and collaborative (everyday kitchen tasks).52,53
Interventions for children and young adults focused on facilitating social interaction in schools and with classmates. 49 These interventions helped participants maintain relationships with ties outside the hospital. 49 A music therapy SVR study connected a person living with a spinal cord injury to their music therapist and to others in VR in the intervention's custom-built virtual setting of choice (campfire, sunset, eureka, house, urban, and space). 47 Participants reported singing together in VR gave a feeling of a shared experience, but it also reduced some social cues with the absence of visual “human” cues.
RQ5: Impact of SVR on the patient social experience
Overall, virtual environments helped patient populations maintain relationships with people and environments outside of the hospital setting.45,49 Specifically, the SVR interventions helped patients connect to loved ones at home and keep up with routines at school and achieve a smoother transition back to home life and school following treatment.45,49 See Table 4 for more information.
Patient inclusion and exclusion criteria listed per study.
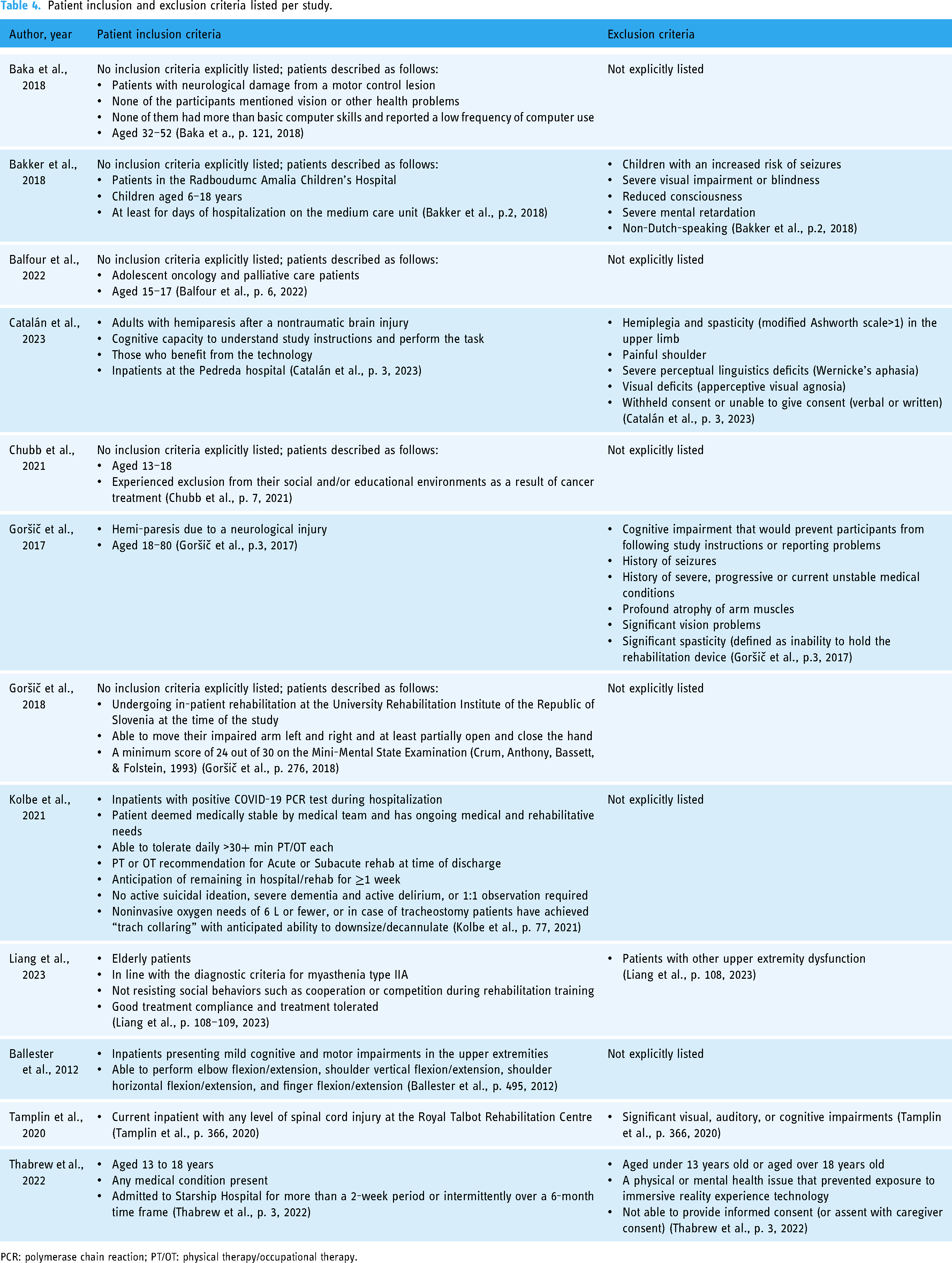
PCR: polymerase chain reaction; PT/OT: physical therapy/occupational therapy.
For hospitalized children, who were participants in the VisitU program, using VR goggles to be elsewhere outside of the hospital was reported as the main benefit. The experience of being in their homes virtually allowed study participants to connect with friends, family, and pets. All participants shared that they would recommend the VisitU program to other patients and that they would like to use it again (pp. 4). 48
A 2022 open trial in New Zealand for hospitalized young adults paired study participants with their school classroom, teachers, and peers through an immersive reality experience. 49 Maintaining a connection with the school environment through the immersive reality experience while hospitalized was described as beneficial by all participants. Participants found that the ability to maintain relationships during their hospitalization made returning to school easier. The technology was perceived as improving the transition back to school through providing environment familiarity (from the caregiver perspective) and peer connection maintenance (from the teacher perspective).
RQ6: Influence on treatment
Study outcomes were generally psychosocial and usability oriented. No papers reported specifically on SVR's effect on adherence to the clinical treatment outside of the VR intervention. Study inclusion and exclusion criteria are detailed in Table 4 for more information.
However, interventions focused on rehabilitation purposes often merged the clinical rehabilitation treatment with VR. We categorized this as complementary to the inpatient's clinical treatment, whereas separating the SVR intervention from clinical treatment was categorized as supplementary to treatment. A stroke motor rehabilitation study found participants in the multiplayer VR game performed significantly higher elbow flexion movements compared to the single VR game.
54
In addition, two rehabilitation studies compared solo, collaborative, and competitive arm rehabilitation sessions to understand the intervention's impact on motivation, exercise intensity, and exercise duration.52,53 Furthermore, Baka and colleagues noted the affordances their therapeutic VR system allotted to stroke patient participants during their hand movement rehabilitation exercises, such as motivation.
55
“So, during the last exercise, despite its great difficulty, patients were so motivated to continue trying playing music that results were remarkable and unexpectable, even for the occupational therapists” (pp. 123).
55
We found no validated scales were used to understand the influence on treatment. However, one intervention studied VR in inpatient rehabilitation for COVID-19 patients and included a survey item focused on enhanced treatment (“Do you feel like VR added to, or enhanced, your treatment? [Y/N]”). The vast majority of patient participants (12/13) reported yes. 46
In addition, 100% of the patient participants responded that they would recommend the VR tool to other patients. Satisfaction with the VR tool in managing pain and anxiety was high (mean score of 8.42 and median score of 9; with the scoring as 1–10, 1 = “not at all satisfied,” 10 = “extremely satisfied”). All staff participants that used the tool (11/11) also reported that the tool enhanced their well-being at work and that they would recommend it to other staff members. The staff were also highly satisfied using the tool for stress management (mean score = 9.45 and median score = 10). This was the only study to include healthcare workers staff as study participants. 46
RQ7: Social outcomes: positives and negatives
Social interaction perceptions varied across studies. Several found benefits in socialization and connection,45,48,56 even if participants were initially apprehensive about VR. 49 Also, most participants across studies favored multiplayer VR games compared to single-player games for motivation or connection.50–54
Several studies reported mixed findings. For example, Thabrew and colleagues acknowledged that connecting did not always equate to connectedness. Sometimes, the connections could be superficial and largely depend on the connected people, such as the level of the VR buddy's engagement. 49 Further, having this opportunity may stir up feelings of obligation rather than desire. 49 Despite these drawbacks, participants in this study reported improvements in social measures. All participants (10/10) reported improvement in social connectedness, and the majority also reported improved well-being (8/10 participants) and improved social inclusion (7/10 participants). 49 Additionally, the study found the reported changes in social connectedness to be statistically significant. 49
VR use also had drawbacks for social connectivity. For example, another study included a singing intervention, using vTime, for people with spinal cord injury. 47 Thematic analysis of participant interviews revealed that VR may reduce social cues, such as nonverbal cues, needed for connection building. 47
Several studies reported benefits while acknowledging that some participants experienced difficulties, like treatment side effects (nausea) or an exhausting hospital environment (lethargy).
56
However, the authors also reflected that this codesign experience led to the work-in-progress design being a socialization opportunity for participants, as participants shared their creation (the virtual world) with their audience (family members and hospital staff).
56
One of the unexpected elements of the pilot, was the joy of the participants in sharing and becoming tour guides of their world to family members and hospital staff. The simple device of rigging up a monitor so that people in the room could watch how the immersant navigated the space, created a natural audience, and socialised the experience of the VR world (pp. 9).
56
RQ8: Barriers
We identified physical side effects, setup onboarding, technology apprehension, and privacy as barriers to SVR use. In addition, accessibility was mostly not addressed in this study. Technical problems and software issues were identified as additional implementation barriers. These were problems reported by both study participants and the researchers who conducted the studies. In one study, several hospital staff were initially skeptical of the technology but changed their perspective after learning from other staff members about the socialization opportunities. 46
Side effects from both treatment and using VR impacted interventions. For example, some participants experienced motion sickness, but symptoms were relieved when laptops replaced the head-mounted displays (HMDs). 45 In addition, headache, nausea, and dizziness were reported as physical side effects by 5/8 hospitalized participants using VR in a study with hospitalized children. 48 These symptoms are commonly related to cybersickness. However, despite these side effects, most participants continued to use VR. Authors reported that “noteworthy is the comment of one patient that he felt “depressed” right after the usage because he did not want to quit” (pp. 4). 48
Environmental awareness and thoughtfulness surrounding existing care routines (for example, nurse staff visits for observations and infection control checks) were deemed necessary, and flexibility with scheduling and responsiveness was crucial for sustained engagement in a study of young adults hospitalized due to a serious illness. 56
Concerns about privacy constituted another implementation barrier, specifically hesitancy around recording participants in the study and capturing them on camera. Privacy was not commonly discussed in the reviewed literature. Specifically, it was rarely reported if or how participants or study staff discussed patient privacy, data privacy, or device use privacy with these emergent technologies.
One study, focused on connecting hospitalized participants to their paired social interaction partners in school or home settings, acknowledged filming in the classroom as a privacy concern, but the fact that their study technology did not allow for recording helped address these concerns.
45
Thabrew and colleagues noted that privacy concerns are not well-discussed in the literature. They also stress the importance of providing education on the purpose of the intervention and the virtual delivery method. In their study educational conversations helped alleviate potential misunderstandings.
49
For example, they stated that: Both teachers and caregivers noted initial concerns about who else would see into the classroom, whether the sessions were being recorded, and whether the teacher was being judged by onlookers. The Patience Project was designed for the child's eyes only, and after speaking with the project custodian, teachers and students in the classroom felt assured that privacy would be uphel” (pp. 9).
49
Physical privacy was addressed in a study that codesigned a virtual space with inpatient participants. 56 Specifically, they addressed spatial conditions when working with patients and how to appropriately approach their space as it is outside the norm of traditional group workspaces. 56
In addition, a study conducted in a COVID-19 rehabilitation recovery unit addressed response privacy. 46 The study authors acknowledged that bias or observer-expectancy effect was a limitation. Hospital unit staff members often had to record feedback because the participants’ illness limited their ability to privately complete assessments. 46
Discussion
Our study identified three primary use categories in SVR interventions for inpatient populations: rehabilitation purposes, music therapy, and social connection. Study designs varied widely within our sample, but the three common study designs were experiments, interviews, and codesigning virtual environments. Overall, patients’ hospital experiences improved with SVR interventions by providing social connection, especially to ties existing outside of the hospital, such as family members, classmates, and friends.45,48,49 Further, the diagnoses of inpatient populations largely shaped the SVR intervention experiences; for example, multiplayer games were used for arm rehabilitation purposes by inpatients with hemiparesis. 51 Psychosocial outcomes were often shared during interview studies or self-reported. However, adherence to or impact on clinical treatment was not commonly or consistently reported by studies. Variance in reporting was also found in a systematic review on safety of VR use in children; the review findings included that safety data was rarely reported and adverse events were often unclearly reported. 57 Incorporating an existing framework developed by Birckhead and colleagues could help to improve consistent reporting in studies that evaluate VR treatments. 58 The SVR interventions were often supplementary rather than complementary to the inpatients’ clinical treatment, except for when studies used SVR games for rehabilitation purposes. The rehabilitation-focused studies had overlap between the SVR intervention and the clinical rehabilitation treatment,52–55 whereas for the other studies the SVR intervention was not paired with the medical treatment. There were both positive and negative aspects of the social outcomes of SVR use: the interventions often led to socialization, but socialization quality varied by social pairing.
The SVR technology often brought people together, such as across locations (bridging the gap between hospitalized patients and their existing ties in the classroom) and within locations (fellow inpatients competing or collaborating in multiplayer games together).45,49,52,53 Two studies included virtual environments that were custom-built but combined with commercially available devices (VR headsets, Oculus Rift, HTC Vive, Samsung Gear, and Jacktrip, and application (vTime).47,56 Three studies, focused on inpatient rehabilitation, used rehabilitation systems for the study device: Bimeo rehabilitation system and the Rehabilitation Gaming System.52–54 The seven remaining studies used a variety of off the shelf devices and platforms, including Oculus Go and 360-degree cameras. As a result, most of the devices and virtual environments were off the shelf and commercially built, without additional technology development. This helps demonstrate that existing SVR technology may be useful for study interventions in clinical settings because it is already commercially available, which may help streamline development and technology onboarding. However, barriers to use in SVR technology included treatment side effects, technology apprehension, privacy discussion, and technical onboarding. These barriers exist within the clinical and healthcare field, as reported in recent scoping reviews.59,60
A recent scoping review identified information on VR clinical effectiveness in palliative care as limited due to small sample size and the use of self-report measurements. 18 This is in line with our findings where data on level of adherence and outcomes associated with SVR use were infrequently reported. Future studies should track adherence to clinical treatment with SVR interventions longitudinally to understand if SVR influences treatment outcomes. In addition, another recent scoping review examined the utility of VR interventions to promote the health and well-being of people living in residential aged care without cognitive impairment. 61 Although we examined different populations, our future research suggestions are similar in terms of areas that would make VR technology most useful: prioritizing meaningful engagement and connection, considering individual capabilities and preferences, and addressing staffing and technological requirements. 61 Codesigning was a featured study design factor in our scoping review's extracted studies, and a study found that the structure of codesign within the hospital led to the socialization of participants. 56 Identifying user preferences and accounting for their capabilities could be future areas of user-centered design work in this area with both inpatient and outpatient populations. Customizing VR programs and software plus having ready access to VR software developers and design experts were reported as enablers in a recent study that surveyed health care professionals on VR use within the hospital setting. 62 In addition, our extracted studies varied in the social partners matched within the SVR interventions. As Thabrew and colleagues discussed, the connection can also largely depend on the social partner's engagement as well as the participant's engagement. 49 Future work could measure clinical outcomes with SVR interventions categorized by social pairing and preference to better understand how meaningful connections can be built by populations within SVR. Finally, setup onboarding and technology apprehension were both identified as barriers within our review. This finding stresses the importance of developing strategies to facilitate a smoother VR experience, which has also been underscored by others. 61
Our findings have implications for future research and the development of real-world applications. The fact that commercially available technology was used in many of these studies showcases its potential (noting areas for improvement including technology onboarding) for making SVR accessible to more potential users. For example, the Oculus Go, included in the 2022 intervention from Thabrew and colleagues, is available for purchase on Amazon, Walmart, and eBay. In addition, the range of VR devices and platforms for social use demonstrates the implementation possibilities and fit within various study designs. For example, a qualitative preliminary clinical study used the HMD Oculus Rift and Leap Motion device for neurologic music therapy intervention with stroke patients at a hospital in Athens, Greece. 55 Another study, with an intervention focused on integrative care delivery model for COVID-19 recovery, used a headset and AppliedVR's SootheVR program with inpatient COVID-19 patients in a New York hospital in the United States. 46 These studies overlap with the use of an SVR intervention for inpatient populations. However, their difference among all other variables (geographic area, device, population diagnosis, intervention purpose) show the breadth of possibility for application in real-world settings within this emerging field for clinical use.
Our scoping review provides information on areas for growth and the types of studies needed to move the field forward regarding clinical applications of emerging technologies, such as SVR. For example, future research could measure social inclusion, well-being, and social connectedness between participants and their pairs to understand if there is a difference in social connection between pairs before and after technology use. In addition, barriers were commonly reported in these studies, and continued reporting of barriers can help future studies account for these issues and minimize them moving forward. For example, in a study connecting hospitalized adolescents with teachers, students, and caregivers, having project staff address privacy issues with study participants helped alleviate participant privacy concerns. 49 Identifying privacy as an essential onboarding topic may also help address any misunderstandings or confusion about introducing the emerging SVR technology. Additionally, these concerns may fluctuate as people continue to navigate the rise of technology presence in new spaces.
Limitations
We conducted a scoping review on SVR interventions for inpatient populations. As a result, we suggest future studies review outpatient SVR interventions as an additional research avenue. SVR interventions where people are physically together but virtually alone (the activity of using VR in the same physical space but exploring the world independently) could also be studied moving forward.
The emerging state of the field limited our sample size. As more studies are published, future work could conduct larger-scale systematic reviews. Another limitation is that we only reviewed English-language papers. Also, of the 12 extracted studies, only one reported participant race and ethnicity breakdowns, meaning that we are unable to determine how representative these participants were of hospitalized patients in general. As a result, our paper provides an introductory understanding of this area, but our sample size and review of only English-language articles limit generalizability. In addition, our review focused on inpatient hospital settings to narrow the scope. This helped provide homogeneity to understand the nuances among these interventions, such as difference in intervention duration while in the hospital and with medical treatment. However, the sample size was still heterogeneous, such as with the variance in measuring influence on clinical treatment, which impacted generalizability.
Despite these limitations, the results of our study strengthen the understanding of using SVR with inpatient populations by addressing the strengths, setbacks, and future directions of SVR use cases in clinical settings. Studying SVR in clinical settings helps highlight potential social opportunities for patients across diagnoses and hospital settings. The emerging nature of this field is often fast-paced, and our findings help establish the benefits and drawbacks of research within this area thus far. Our results support future research that aims to understand what VR technology is feasible within this context and where further research is needed.
Conclusion
SVR can provide opportunities for socialization when geographic barriers or hospital policies (e.g. visiting hours) limit in-person socialization. However, various considerations, including privacy concerns, can impact SVR outcomes before, during, and after using SVR. Understanding the range of these variables will help shed light on how SVR can influence social support and therapeutic outcomes for patient populations, highlighting the need for future studies to report on specific protocols of SVR interventions to provide blueprints for additional work.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241306460 - Supplemental material for In sickness and in health—A scoping review on social virtual reality clinical applications
Supplemental material, sj-docx-1-dhj-10.1177_20552076241306460 for In sickness and in health—A scoping review on social virtual reality clinical applications by Stephanie P Belina, Sara J Czaja, JoAnn Difede, Kevin J Pain, M Carrington Reid and Andrea Stevenson Won in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076241306460 - Supplemental material for In sickness and in health—A scoping review on social virtual reality clinical applications
Supplemental material, sj-docx-2-dhj-10.1177_20552076241306460 for In sickness and in health—A scoping review on social virtual reality clinical applications by Stephanie P Belina, Sara J Czaja, JoAnn Difede, Kevin J Pain, M Carrington Reid and Andrea Stevenson Won in DIGITAL HEALTH
Footnotes
Acknowledgments
The authors list no acknowledgements.
Contributorship
Authors 1, 2, 3, 5, 6 conceptualized the study. Authors 2, 3, 5, 6 acquired funding. Authors 1, 2, 4, 5, 6 developed the methodology. Author 4 managed data curation and software. Authors 1, 2, 5, 6 conducted the investigation. Author 1 wrote the original draft. Author 6 supervised. All authors reviewed and edited the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
No ethics approval was required for this review article.
Funding
This article was supported by the grant R03 AG080413-01 from the National Institute of Aging of the National Institutes of Health, U.S. Department of Health and Human Services.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.