
Abstract
Breastfeed4Ghana was a social media-based campaign implemented to address identified gaps in the protection, promotion, and support of breastfeeding in Ghana. This paper describes the process of campaign materials development and testing to ensure their cultural and content appropriateness. The 60 campaign materials, each consisting of an image and text message, underwent a process of creation, testing, revision, and finalization. Existing research evidence and infant and young child feeding communication tools that were culturally relevant for Ghana were used to develop the materials. All materials were tested and finalized through an iterative process that incorporated input from six focus group discussions (FGDs) with mothers, and content and technical experts. The materials were revised to ensure scientific accuracy, understandability, and cultural appropriateness of the messages, as well as alignment of the messages with the images. Finalized materials were reviewed and approved by the Ghana Food and Drugs Authority. Analysis for this paper involved summarizing and categorizing the types and sources of input as well as the research team’s responses to the input received. The 60 campaign materials received a total of 132 inputs. Most inputs came from FGDs (78.4%); and most inputs were on the campaign material images. The evidence-informed process of materials creation, use of multiple input sources, and a broad-based iterative process allowed the creation of 60 evidence-based and culturally appropriate materials for a breastfeeding social media campaign in Ghana. This paper could serve as a guide for other social media campaign efforts looking to develop culturally appropriate materials.
Introduction
Social media online communities that enable users to create and share electronic content 1 are becoming ubiquitous among new mothers, especially those seeking information and support. 2 Connecting on social media can provide new mothers with external validation of their motherhood. 3 Indeed, breastfeeding mothers have reported using social media to make connections, find information, and be entertained.4,5
While the majority of research regarding social media and parenting has been conducted in high-income countries, the rapid uptake of social media has been a global phenomenon. 6 Specifically in Ghana, use of social media has increased among adults 18 years and older by an impressive 60% between 2015 and 2017, (20–32% of all adults).7,8 Use is higher (43%) among young adults (18- to 36-year-olds), but specific data on Ghanaian mothers is not currently available. If the adoption of social media in Ghana continues at the rate suggested by the Pew Research Center data, we would anticipate market saturation by 2023.7,8 Therefore, it is important to identify how best to harness social media platforms for public health campaigns in contexts akin to Ghana.
Social media-based health promotion campaigns can have a direct and positive effect on behavior.9,10 Over the last 15 years, social media has increasingly been used as a platform for health promotion, particularly in high-income countries.10,11 However, little research has been conducted on the effect of social media-based campaigns for protecting, promoting, and supporting breastfeeding. 12 As a result, the 2016 Lancet series on breastfeeding called for further research on the role of social media in breastfeeding promotion, noting the limited guidance on how to develop such campaigns.13,14
The benefits of optimal breastfeeding practices are widely documented.13,15 Specifically, the World Health Organization (WHO) recommendation of exclusive breastfeeding (EBF) through the first 6 months,16,17 is linked with child survival, optimal physical growth, and cognitive development. 15 Despite tremendous progress in achieving optimal breastfeeding practices across Ghana, the rate of EBF has decreased without clear explanation.18,19 In response, a committee of breastfeeding stakeholders in Ghana implemented the Becoming Breastfeeding Friendly (BBF) initiative in 2016, which resulted in recommendations and action plans to scale up breastfeeding policies and programs nationally.20–22 Key recommendations that emerged included 1) fostering strong advocacy for breastfeeding, 2) harnessing support for maternity protection legislation, and 3) effectively disseminating accurate and actionable breastfeeding information to the public. 20 The committee of stakeholders who implemented BBF proposed that a breastfeeding social media campaign be designed as a low-cost and novel health communications intervention to help implement these recommendations.
In response to these key evidence-informed recommendations, and the lack of evidence on how to develop a breastfeeding campaign via social media in this context, methods designing such a campaign were needed. Such a design needed to integrate strong existing evidence from multiple disciplines. For instance, well-established frameworks for social marketing exist, such as the social marketing wheel.23,24 Traditional social marketing practices have been applied for breastfeeding promotion, 25 and the social ecological model 26 has repeatedly been applied in the context of breastfeeding protection, promotion, and support. 27 A user-centered, person-based approach to designing interactive digital health interventions has been lauded as complementary to such interventions with a theoretical underpinning, and has also been proposed specifically for interventions that target user engagement.28–30 Despite existing social marketing and social media frameworks, there is a lack of evidence on the development of health-focused social media campaigns such as breastfeeding. Indeed, no examples of the development of such social media campaigns in sub-Saharan Africa have been reported in literature.
Therefore, to fill this gap in the literature in sub-Saharan Africa, we present the development and testing process of campaign materials for Breastfeed4Ghana, a Facebook- and Twitter-based campaign designed to improve breastfeeding knowledge and perceptions among Ghanaian adults. 31 We detail the iterative, user-centered development of evidence-based and culturally appropriate materials for this campaign that was grounded in the social ecological model, 26 and utilized inputs from multiple sources (Box 1). We also present descriptive results to outline this process.
Materials and methods
The study was implemented in an iterative stepwise process. First, campaign materials composed of a text message accompanied by a complementary photograph were designed (Box 1). Next, the campaign materials were tested in focus group discussions (FGDs) and their feedback was used to revise and improve the simplicity, cultural appropriateness, and acceptability of the materials. In addition to the FGDs, inputs for revision were obtained from a diverse group of content and technical experts including experts in maternal–child nutrition and lactation (Breastfeed4Ghana advisory group), the BBF committee, and the Food and Drugs Authority (FDA) (Box 1). The experts reviewed the materials for validity (e.g., confirming that the messages were consistent with national and global recommendations for breastfeeding), alignment (e.g., confirming that messages corresponded with the images used in terms of infant age), and clinical appropriateness (e.g., confirming that the images depicted appropriate breastfeeding technique, including positioning and latch). All inputs were reviewed and incorporated, iteratively, to enhance both the acceptability and validity of the materials prior to finalization. Details of this study approach are provided here. Description of terminologies and acronyms
Formative development of campaign material
The Breastfeed4Ghana social media-based communication campaign was grounded in the social ecological model, a theory-based framework for understanding complex and multifaced determinants of behavior across four levels that reflect personal and environmental factors: intrapersonal, interpersonal, community, and society levels. 26 Thus, the campaign provided messages targeting not only breastfeeding mothers, but also their close family and associates, as well as decision-makers who influence the broader breastfeeding environment. The overall campaign was designed to provide positive, simple, educational messages for breastfeeding protection, promotion, and support. Positively oriented messages emphasize the benefits of breastfeeding, and have been considered more persuasive than negatively oriented messages.32,33 Thus, all messages were designed to be brief, easily understood, culturally appropriate, and relevant for the target populations of breastfeeding mothers, their close family and associates, and decision-makers who influence the broader breastfeeding environment, so that users can easily apply them as a basis for behavior change. 34 Each material had a brief message that included between 7 and 31 words, paired with a single photo, to reinforce and complement the message. The messages were designed based on existing Infant and Young Child Feeding (IYCF) recommendations of the Ghana Health Service, WHO, United Nations Children’s Fund, and the Ghana BBF committee (Box 1).20,35,36
The first step was the development of an initial set of 11 campaign messages (Figure 1). Complementary images were selected and used to create this first set of campaign materials (Box 1). These initial materials were presented to mothers of young children (n = 19) who provided feedback in two community group dialogues prior to the formal launch of the research phase of the study. Based on this feedback, the materials were revised and submitted to the FDA for official approval. Input from the mothers who participated in the community dialogues and from the content and technical experts guided the development and subsequent finalization of 49 additional materials, yielding a total of 60 campaign materials.

Summary of the evolution of the Breastfeed4Ghana core campaign materials from multiple sources of input.
The digital design of the campaign materials was led by a digital creative agency with input from the study investigators as well as the content and technical experts. The creative agency was responsible for creating appropriate, high-quality photographs to complement the campaign messages.
Testing for acceptability and cultural appropriateness
Subsequently, all 60 campaign materials underwent a similar review and finalization process (Figure 1). Because the initial 11 materials had already received input from mothers in the target population, they were subsequently only reviewed again by the expert advisory group. In addition, the images of the initial materials were revised for cultural appropriateness, using original photos. The FGDs used for testing the materials aimed to assess understanding and cultural appropriateness of the materials in terms of 1) the message, 2) the image, and 3) message and image alignment, from the primary end-user perspective (i.e., social media users from the target audience). An interview guide was developed and pretested for use in conducting the FGDs (see Additional File 2).
Women who participated in the FGDs were recruited at selected health facilities or community-based child welfare clinics (CWC) in Accra, Ghana by the campaign coordinator, with assistance from public health nurses at the various CWCs. The women were included if they had delivered and breastfed a healthy infant in the preceding 2 years. A total of 48 women participated in the 6 FGDs conducted (Table 1).
Socio-demographic characteristics of focus group discussion participants.

Note: 1Data are presented as mean ± SD or n (%).
In each FGD, an average of 15 materials (range: 9–20) were displayed and discussed, one at a time, either electronically (using an LCD projector), or as a color-printed large poster (on A3-sized paper). The FGDs were facilitated by the campaign coordinator. Each FGD was audio recorded, and a notetaker was present both to record notes and to support the facilitator. The audio recordings from each FGD were transcribed verbatim. Through an ongoing process of material review, input received from FGDs and experts were used to revise the materials (Figure 1).
Finalization of the materials was carried out by the study investigators working closely with the digital creative agency, and harnessing all input from the FGDs and the content and technical experts, in accordance with the campaign design theory. Thereafter, color-printed versions of the 60 materials were submitted to the Ghana FDA for final approval, as legally required (Figure 1).
Data analysis
The quantitative and qualitative analytical approaches described here, utilized inputs obtained during the testing and finalization stages of the campaign material evolution (Figure 1). This analysis involved a two-stage process. First, campaign materials were organized into a database that allowed tracking of type, frequency, and source of inputs (i.e., from FGD, IYCF experts, BBF committee, or FDA), as well as the decisions made based on each input by the investigators. Types of input were classified on the three core elements of the materials: 1) image, 2) message, and 3) alignment between image and message. Revisions based on input were classified as 1) incorporating the input, or 2) not incorporating input. The latter only occurred with input from FGDs; the reasons for not incorporating inputs are reported in Additional File 3. One investigator conducted an initial classification and assessment of sources and forms of input and responses. Thereafter, two additional investigators independently reviewed and provided input. Review and final decisions on inputs were achieved via discussion and consensus between at least two investigators. The results present a descriptive assessment of the results.
Results
The initial stage of the analysis included recording the evolution of the materials during testing and finalization. Table 2 provides examples of campaign materials and illustrates the process involved in organizing, summarizing, and finalizing the materials (Additional File 3 provides the full output).
Examples of how inputs were used to modify campaign materials.
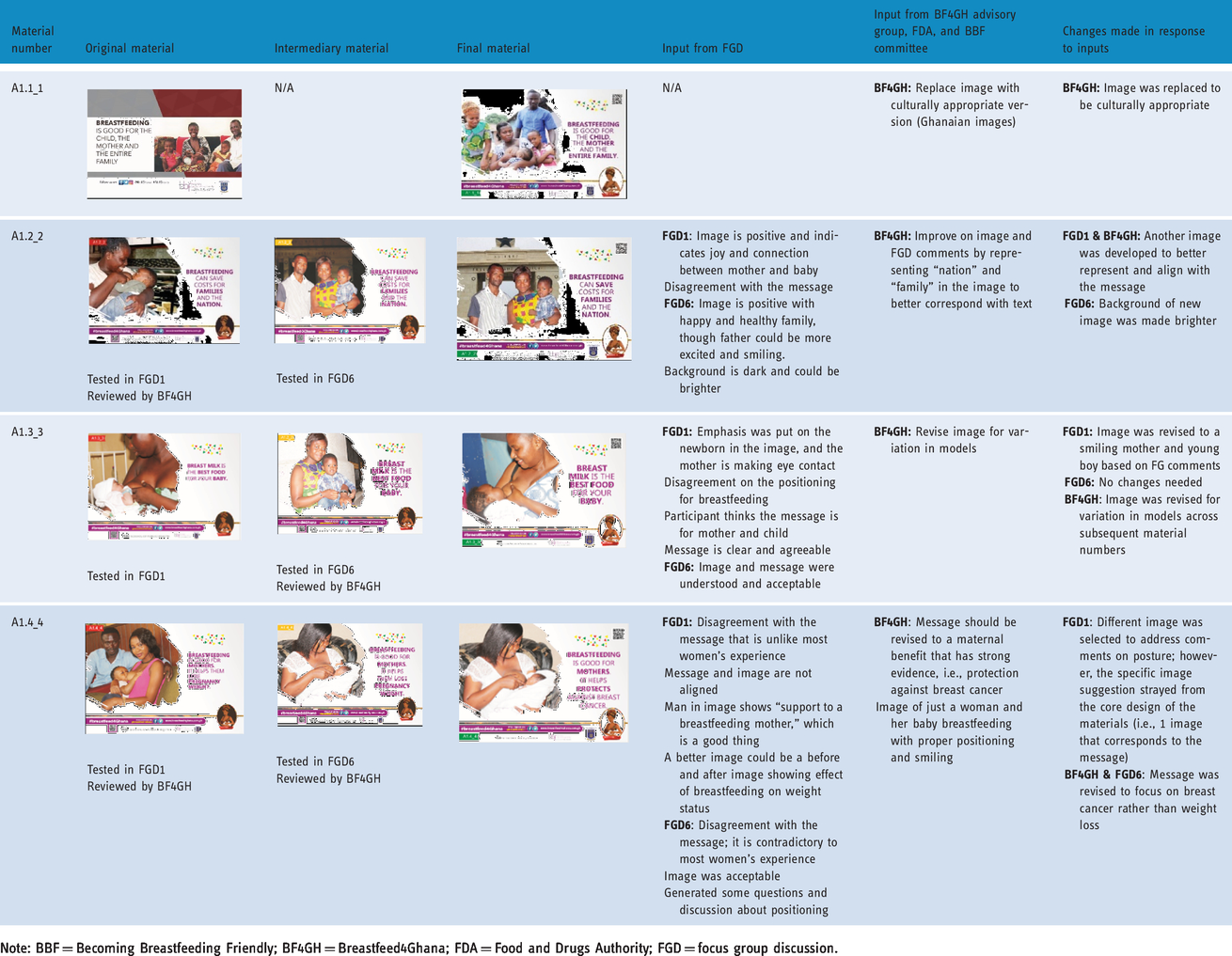
Note: BBF = Becoming Breastfeeding Friendly; BF4GH = Breastfeed4Ghana; FDA = Food and Drugs Authority; FGD = focus group discussion.
Source of inputs
The 60 core campaign materials were tested and finalized based on 132 inputs from four sources: FGDs, Breastfeed4Ghana advisory group, BBF committee, and the FDA (Figure 2). The majority (68%) of these inputs came from FGDs, followed by inputs from the Breastfeed4Ghana advisory group (28%). The median number of different sources of input for a given material was two (Table 3). Although two of the materials that were previously tested and approved by the FDA during formative development were retested in FGDs, a total of nine materials that had been previously tested and approved were not retested in FGDs. All 60 materials were reviewed by the three content and technical expert groups. However, 22 of the materials did not receive any input from these sources; one of these had been previously tested and approved and was therefore not retested in FGDs.

Proportion of sources across the 132 inputs received for the 60 core campaign materials during testing and finalization.
Summary of sources and types of input, and the responses to input on the 60 core campaign materials.

Note: BBF = Becoming Breastfeeding Friendly; BF4GH = Breastfeed4Ghana; FDA = Food and Drugs Authority; FGD = focus group discussion; IQR = interquartile range.
1Percentage is out of 60 materials unless otherwise specified.
2“Other” reasons included alignment/consistency with broader campaign theory, and interest in retesting the materials for additional input.
Types of inputs
The majority of the input from FGDs (78.4%) and content and technical expert groups (76.3%), was to request changes to the images in the material. However, the nature of these inputs differed according to source. In FGDs, image-related inputs were often to support the alignment of the material, ensure variety in images used, and to address the likability and aesthetics of an image, whereas experts’ inputs on the images were primarily regarding cultural appropriateness and breastfeeding technique (e.g., positioning and latch) (Additional File 3).
Inputs were also provided on the messages, although at a lower rate (31.4% of material reviewed by FGDs and 36.8% reviewed by content and technical experts). Most of the message-related inputs consisted of word choice, grammatical changes, or spelling. Three of the four (75%) FDA inputs were regarding the message, and the only BBF committee input was on the content of a message. One of the 60 messages was changed completely during the testing and finalization period (material no. A0104_04), and one message was simplified and given a more positive framing: from “Exclusively breastfed babies have lower risk of chronic disease when they are adults” to “Exclusively breastfed babies will become healthier adults” (material no. A0401_16) (Additional File 3).
Few inputs were received from the Breastfeed4Ghana advisory group, BBF committee, or FDA on material alignment (2.6%); this type of input was received for 15 of the 51 materials reviewed by FGDs. Most of the FGD inputs on alignment were accompanied by suggestions to change the image rather than the message.
Response to inputs
The study investigators made the final decision on inputs from the various sources by working in collaboration with the creative agency to incorporate the required changes into the materials. All inputs from the content and technical expert groups were incorporated directly into the materials, as were 73.3% of inputs from FGDs. Of the 24 FGD inputs that were not incorporated into the materials, seven were inconsistent with the material format for the campaign, and four were not considered feasible due to resource or time constraints. The rest were not considered significant to require revisions, in line with the design theory of the campaign.
Examples of input and responses for selected materials
As shown in Figure 3a, the message of the material was to motivate caregivers to “put your baby to the breast anywhere and anytime that she needs to feed.” Although the FGDs considered the message acceptable, they felt the image (on the left-hand side of the panel) did not convey the concept of “anywhere,” which was considered a critical aspect of the message. Therefore, the image of the breastfeeding baby was encircled by icons of different locations to represent this concept of breastfeeding “anywhere” (Figure 3a).
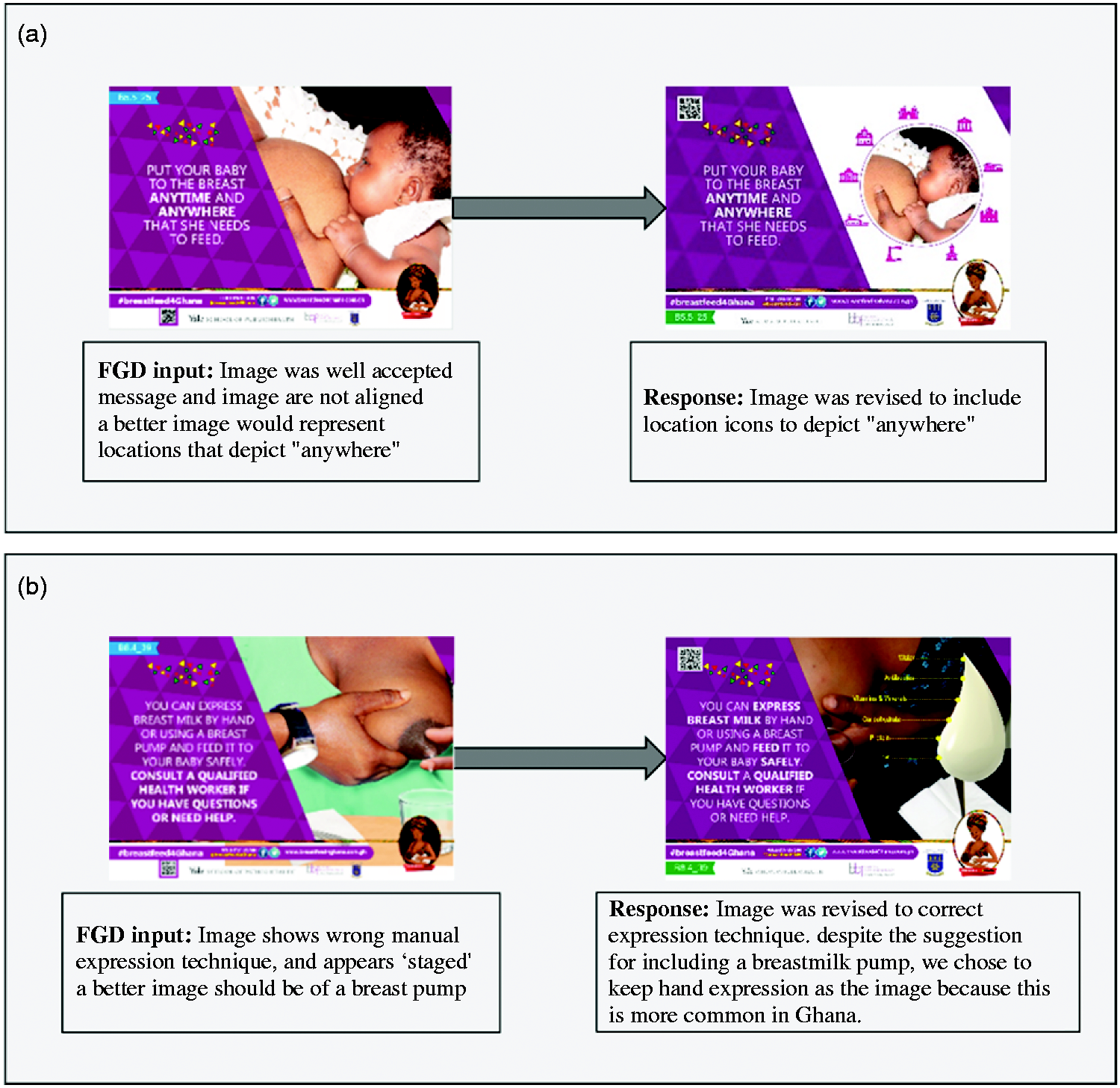
Image demonstrating range of responses to input from a focus group discussion (FGD) toward finalizing the Breastfeed4Ghana campaign materials. Panel A demonstrates an example in which the FGD input was to address poor message–image alignment. Panel B demonstrates an example in which some of the FGD input, specifically to include an image of a breast pump, was not utilized out of respect for local context practice.
Figure 3b demonstrates a case in which FGD inputs were not incorporated due to cultural sensitivities. In this situation, the image was modified in response to FGD input, which indicated it appeared “staged” and also demonstrated the wrong breast milk expression technique. Thus, a revised image (on the right-hand side of the panel) was used. However, although the FGD suggested using an image of a breast pump, this revision was not carried out because in Ghana, hand expression is common practice.
The one message that was changed completely during testing and finalization was that of material no. A0104_04, which originally stated “Breastfeeding is good for mothers. It helps them lose pregnancy weight.” This generated discussion and debate in FGDs about the women’s own experience with pregnancy weight loss and breastfeeding, and among the Breastfeed4Ghana advisory group who agreed that the evidence for this was not strong enough to promote as a benefit of breastfeeding. Therefore, the message was changed to: “Breastfeeding is good for mothers. It helps protect against breast cancer” (see Additional File 3).
Discussion
This paper presents the iterative, user-centered approach taken to develop and test materials for a breastfeeding social media campaign with the aim of insuring that the materials would be culturally appropriate. Campaign materials were informed not only by the end user, but also with evidence and input from various experts and stakeholders. We found that the nature of the inputs from the target population in the FGDs versus the content from technical experts (i.e., Breastfeed4Ghana advisory group, BBF committee, and the FDA) differed, providing justification for consulting both content and context experts alongside the target population. The expert input was valuable for ensuring message validity, while end-user input was focused on message clarity and acceptability.
It has previously been demonstrated that the messages from communication interventions have greater cultural acceptability if appropriate needs assessment have been designed to understand the situation and needs of the target audience. 37 Such acceptability testing is a key element of designing health interventions. 38 A user-centered approach aligns with an emphasis on acceptability, and such an approach is particularly effective for interventions targeting user engagement. 28 Given that, in the context of social media, user engagement is a key performance metric for campaigns, 39 the choice of user-centered design was justified for Breastfeed4Ghana as well as other health promotion campaigns.
The visual elements (i.e., images) of the materials designed in the current study constituted an important area of feedback from the users. Image–message misalignment can create a vague understanding of what is being communicated to end users, thereby leading to misperceptions of the message. 40
Following its design, the campaign was run on Facebook and Twitter for a 6-month period. The results are reported in a forthcoming publication (Maternal and Child Nutrition Journal), and indicate acceptability of the campaign and engagement with the material content among both men and women in Ghana. 31
Lessons learned
In the process of designing the materials, the research team identified a number of practical lessons that can serve as a useful guide to those who will be developing materials for campaigns similar to Breastfeed4Ghana. First, sufficient time must be allocated to material development and testing. Approximately 5 months were allocated for developing the 60 materials for this campaign, which proved sufficient. However, adequate time between each FGD must be allowed to review the proposed changes and revise the materials, especially if FGD participants request new images that will need to be sourced and approved by the research team. The duration required for campaign material development and testing will, however, depend on the number, context, and nature of the materials being developed.
Another important lesson from this study is acknowledging that the images are an essential part of material development. Stock photos were initially used before recognizing they were not culturally acceptable. Thus, only original images were ultimately used to ensure cultural acceptability and campaign branding. Furthermore, it was originally planned to utilize the same images across multiple messages. However, FGD feedback revealed that the recycling of images was poorly received. Across all inputs from all source types, we found the image to be the element that required the greatest attention and time for revisions.
Limitations
Despite the value that this study adds to the literature, there are some important limitations to these findings. The end-user input we sought in this process was limited to mothers in Ghana, despite the campaign’s broad approach to provide messages for family, friends, employers, and co-workers to support and protect breastfeeding. Although input was sought from a diverse group of experts, input from civil society that could have provided additional value was not received. Finally, we have not presented the results on campaign engagement in this paper, but rather focused on the acceptability of the content. However, such results on campaign engagement and content acceptability during the active campaign period have since been published, which confirm that the campaign material was acceptable and the target population (i.e., breastfeeding mothers, family members and associates, and decision-makers who influence the broader breastfeeding environment) did engage with it. 31
Conclusions
This study demonstrated an iterative, user-centered, evidenced-based approach to designing a culturally appropriate and relevant breastfeeding social media campaign in Ghana that was grounded in the social ecological model. Starting with a foundation of the context-specific needs is essential. In the current study, this evidence came from the BBF assessment, and engagement with breastfeeding stakeholders in Ghana. The development stage of such a campaign should emphasize cultural acceptability and relevance, and aim to achieve acceptability among the target population of the campaign. This can be achieved by seeking input from a variety of sources with unique perspectives on the content, culture, dissemination platforms, including end users.
Supplemental Material
DHJ909291 Supplemental Material1 - Supplemental material for Design and testing of communication materials for a breastfeeding social media marketing campaign: Breastfeed4Ghana
Supplemental material, DHJ909291 Supplemental Material1 for Design and testing of communication materials for a breastfeeding social media marketing campaign: Breastfeed4Ghana by R Aryeetey, O Lasisi, A Hromi-Fiedler, G Carroll, R Pérez-Escamilla and K Harding in Digital Health
Supplemental Material
DHJ909291 Supplemental Material2 - Supplemental material for Design and testing of communication materials for a breastfeeding social media marketing campaign: Breastfeed4Ghana
Supplemental material, DHJ909291 Supplemental Material2 for Design and testing of communication materials for a breastfeeding social media marketing campaign: Breastfeed4Ghana by R Aryeetey, O Lasisi, A Hromi-Fiedler, G Carroll, R Pérez-Escamilla and K Harding in Digital Health
Supplemental Material
DHJ909291 Supplemental Material3 - Supplemental material for Design and testing of communication materials for a breastfeeding social media marketing campaign: Breastfeed4Ghana
Supplemental material, DHJ909291 Supplemental Material3 for Design and testing of communication materials for a breastfeeding social media marketing campaign: Breastfeed4Ghana by R Aryeetey, O Lasisi, A Hromi-Fiedler, G Carroll, R Pérez-Escamilla and K Harding in Digital Health
Supplemental Material
DHJ909291 Supplemental Material4 - Supplemental material for Design and testing of communication materials for a breastfeeding social media marketing campaign: Breastfeed4Ghana
Supplemental material, DHJ909291 Supplemental Material4 for Design and testing of communication materials for a breastfeeding social media marketing campaign: Breastfeed4Ghana by R Aryeetey, O Lasisi, A Hromi-Fiedler, G Carroll, R Pérez-Escamilla and K Harding in Digital Health
Footnotes
Acknowledgements
The authors appreciate the contribution of all focus group discussion participants for sharing their opinions on the materials. We are also grateful to the Ghana BBF committee and other experts (including Gabriela Buccini) who provided input for developing and testing the materials. We are also appreciative of Elfortify David Sarfo and John Mawuli Nyadegbe at IZSCOPE Ltd for the digital designing of the materials. The following research and administrative assistants were critical for the design and testing of the Breastfeed4Ghana SM communication materials and are duly acknowledged: Abena Engmann, Faustina Aryeetey, Helena Bentil, Vivian Kapio Abem, Cara Safon, Augustina Boadu, and Katie Doucet.
Contributorship
The study was conceived and designed by RA, KH, RPE, and AHF. Data gathering was led by RA with contributions from KH, RPE, OL, and GC. RA and KH led the data analysis and interpretation, with contributions and final approval from all other authors.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval of this study was granted by the Institutional Review Boards at University of Ghana and Yale University. All FGD participants provided written informed consent to participate. In all cases, appropriate consent was obtained by the creative agency from the persons whose photographs were taken and/or used in preparation of the campaign materials. Permission was obtained from institutions, including hospitals in Accra, where the photographs were taken by the creative agency.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Breastfeed4Ghana study was funded by the International Society for Research in Human Milk and Lactation through Yale University (PI. Kassandra Harding), subaward number GR101839 (CON-80001098).
Guarantor
RA is guarantor.
Peer review
This manuscript was reviewed by reviewers who have chosen to remain anonymous.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.