
Abstract
The assessment of patients likely to undergo lung resection surgery is a multidisciplinary approach involving pulmonologists, surgeons and anaesthesiologists. In thoracic surgery, medical operability is also a calculation of postoperative lung function. A mobile application – PreParAPP MSD – to calculate postoperative lung function has been developed with the endorsement of the Italian Society of Anaesthesia, Analgesia and Intensive Care and with the unconditional support of MSD Italia. Thanks to a simple graphic interface, the calculation becomes fast and intuitive, while the possibility of storing and sharing data in an analytical and computerised way with other clinicians might help with the full assessment of patients without forcing them to undergo several medical examinations. These simple calculated parameters are performed by a minority of clinicians, generally anaesthesiologists. In our facility, there is a team involved in the perioperative evaluation of lung resection surgery (13 pulmonologists, 9 surgeons and 5 anaesthesiologists). In order to evaluate the possible Awareness towards postoperative lung function calculation better, we organised an internal survey with 27 clinicians who are members of such a team before and after the introduction of the PreParAPP MSD. It was found that after the introduction of PreParAPP MSD, the percentage of clinicians involved in postoperative lung function calculation rose from 18% to 70%. The implementation of a digital tool may help to improve guideline adherence, in accordance with other experiences in which such tools represented the start for various quality improvement purposes throughout the medical field.
Keywords
Introduction
The assessment of patients likely to undergo lung resection surgery is a multidisciplinary approach involving pulmonologists, surgeons and anaesthesiologists. 1 Besides the oncological and anatomical evaluation of operability, patients have to undergo a medical operability evaluation. This is calculated by using forced expiratory volume in the first second (FEV1), diffusion lung CO (DLCO) and maximal oxygen consumption (VO2max), as reported in the guidelines of scientific societies for pulmonology, surgery and anaesthesia. Slinger described this preoperative calculation as a three-legged stool, with patients sitting on it. 2 In order to keep their seat safe, all three legs have to be checked and be compatible with the ‘additional load’ that the remaining lung tissue should support.
In thoracic surgery, medical operability is not only a static preoperative assessment, but also a calculation of postoperative lung function. Indeed, the predicted postoperative values (PPOs) derive from each of these parameters: FEV1, DLCO and VO2. The formula for the calculation of PPOs is the same for every respiratory variable:
3

The values thus obtained for operability are then compared with the international guidelines of different scientific societies. A low PPO value correlates with higher postoperative morbidity and mortality. It is an indication that the surgical approach should be avoided and that appropriate second-line therapy should be instituted. 4
The relevance of these simple calculated parameters is sometimes underestimated by the majority of medical staff involved in lung resection surgery. Often, as is the case in our institution, all calculations are performed by a minority of clinicians, generally anaesthesiologists. This creates a bottleneck for patients who are subjected to multiple medical examinations, discomfort and long preoperative times. 5
In our facility, patients are normally checked by pulmonologists for a diagnosis of lung cancer. Then, surgeons evaluate the oncological and anatomical operability. Next, anaesthesiologists calculate PPOs in order to test the effective medical operability. Whenever the value is not compatible with the chosen surgery, anaesthesiologists might require an additional pulmonological evaluation in order to examine the possible benefits of a respiratory physiotherapy cycle or pharmacological optimisation of lung function. In this case, the patients should once more be checked by an anaesthesiologist in order to assess any eventual improvement or by a surgeon to propose less radical lung resection which is compatible with their PPOs.
A mobile application (APP) to calculate PPOs – PreParAPP MSD – has been developed with the endorsement of the Italian Society of Anaesthesia, Analgesia and Intensive Care (SIAARTI) and with the unconditional support of MSD Italia. Thanks to a simple graphic interface, the calculation of PPOs has become fast and intuitive, while the possibility of storing and sharing data with other clinicians in an analytical and computerised way might help with the full assessment of patients without forcing them to undergo several medical examinations.
PreParAPP MSD is only available to physicians regularly enrolled in the Italian medical register. As soon as the application is on, it is possible to enter the patient’s anthropometric parameters, as well as his/her personal data and a personalised ID. From these data, the application automatically calculates the theoretic values of FEV1, DLCO and VO2max, and the user only has to enter manually the actual values measured during the pulmonary function tests. In cases where abnormal haemoglobin levels affect the DLCO, it is possible to insert the altered haemoglobin value in order to obtain the DLCO as it would be if the patient’s haemoglobin were normal. At this point, the clinician will immediately have a summary on their screen (Figure 1) which relates the various data and provides the patient’s FEV1, DLCO and VO2max percentages. These values can already provide an indication of the type of COPD and its severity. In the next step, the graphic representation of lung segments is shown, so that the user may choose those segments to be removed (Figure 2). In cases where there are segments not participating in gas exchange, due to previous pathological conditions, the user may exclude them from the PPO calculation on a specific window. Once this step is completed, the digital tool provides the PPOs as absolute and percentage values, as well as providing a summary screenshot of the patient’s anthropometric data and the type of intervention to be performed (Figure 3). In case of pneumonectomy, the clinician can enter pulmonary scintigraphy values and determine PPOs in these patients in a more precise way (Figure 4).
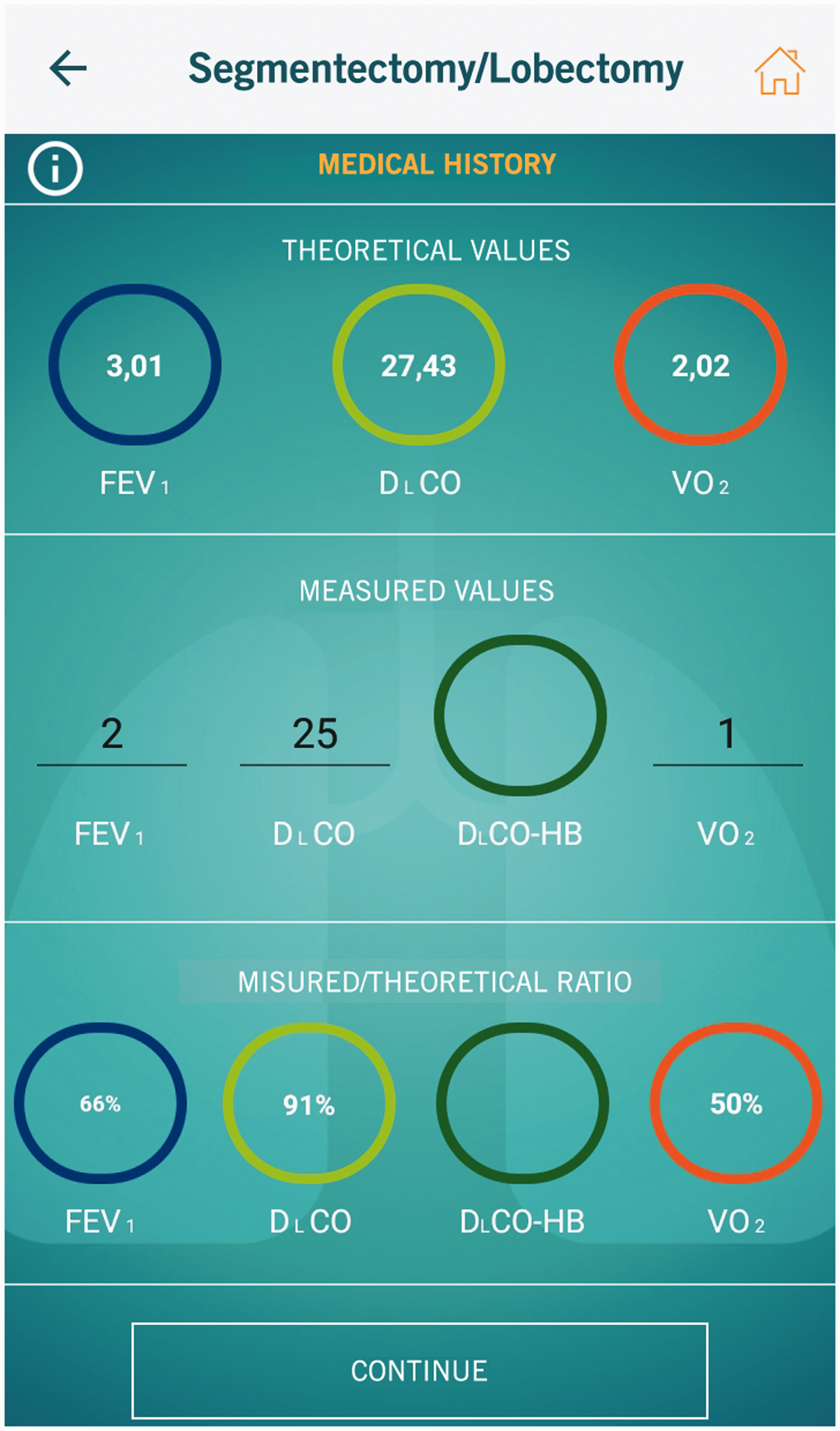
A patient’s summary window relating the various data and providing the percentages of forced expiratory volume during the first second, diffusion lung CO and maximal oxygen consumption.
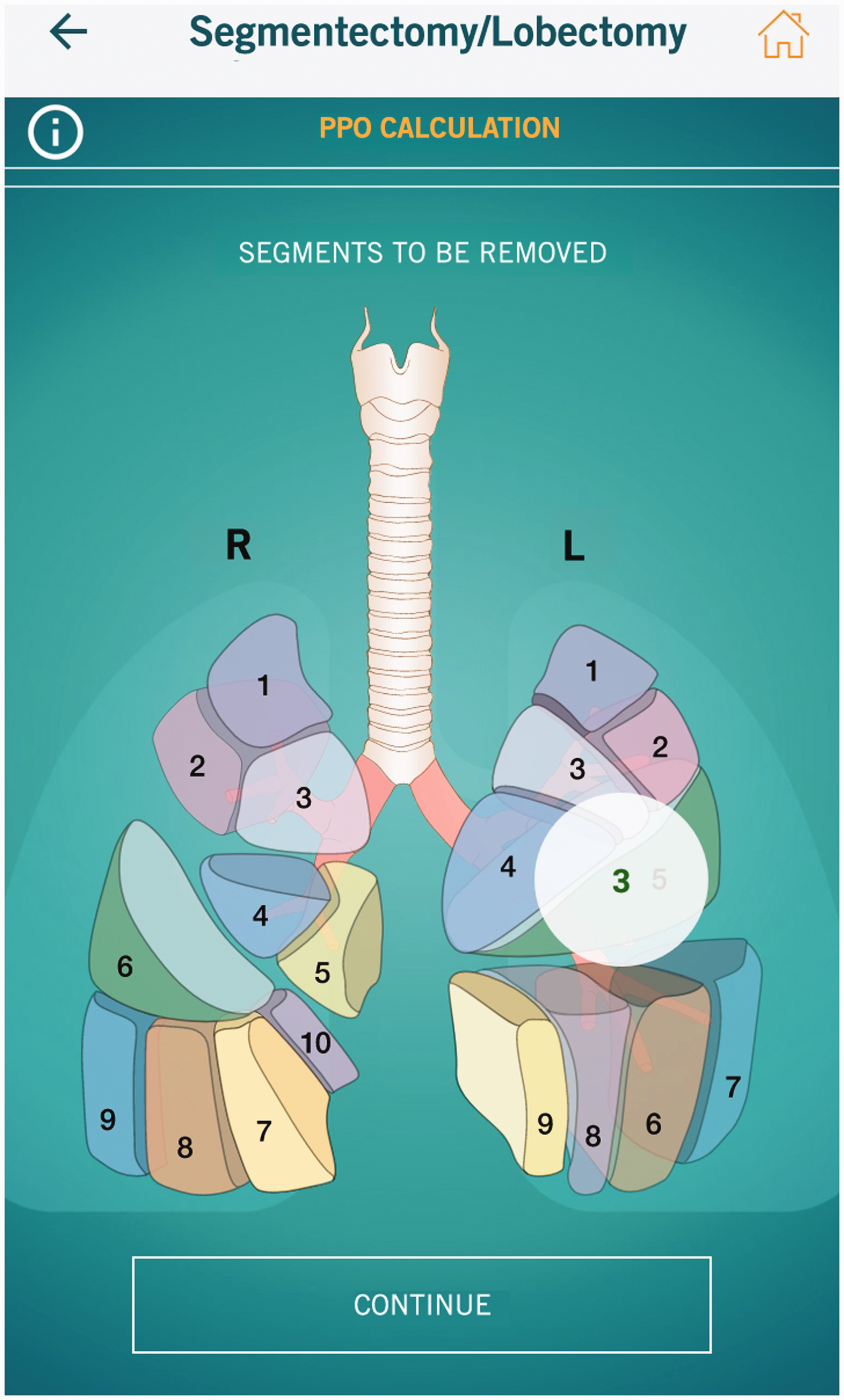
Graphic representation of lung segments so that the user may choose those segments to be removed.

Summary screenshot of a patient’s anthropometric data, predicted postoperative values (PPOs) and the type of intervention to be performed.

In case of pneumonectomy, the clinician can enter pulmonary scintigraphy values and determine PPOs in these patients in a more precise way.
Once the calculation phase is completed, the patient’s record remains in the local memory of the device, characterised by the ID that the user has set. This record can be shared through wireless technology among different devices or saved as a PDF and sent to an external printer. The digital record is designed to be updated in accordance with the patient’s various follow-ups when the clinician can re-enter the measured values of FEV1, DLCO and VO2max to compare them with the preoperative ones and the ones calculated empirically by using the PPO formula.
Methods
In our facility, there is a team involved in the perioperative evaluation of lung resection surgery. In order to evaluate the possible Awareness towards PPO calculation better, we organised an internal survey with 27 clinicians who are members of such a team (13 pulmonologists, 9 surgeons and 5 anaesthesiologists) before and after the introduction of PreParAPP MSD. Before its introduction, participants were asked:
Are you involved in the calculation of PPOs? What is the main reason not to calculate PPOs? Did you know about the existence of PPOs and their role in the guidelines? If you had a digital tool to calculate PPOs, would you use it?
After the introduction of PreParAPP MSD, participants were asked:
Are you involved in the calculation of PPOs? Did you find the digital tool useful? For which function did you find the digital tool most useful?
Results
Only 18% of the whole sample reported being involved in the calculation of PPOs. The primary reasons not to calculate PPOs were not knowing how to do it (59%), believing it was the anaesthesiologists’ responsibility (30%) and believing it was the surgeons’ responsibility (11%). Yet, most participants knew about the existence of PPOs and their role in the guidelines (93%). This lack of familiarity with calculating PPOs might be overcome by providing clinicians with a digital tool in order to calculate and to share this information with other specialists. In fact, 93% of them said that they would use such a tool. After the introduction of PreParAPP MSD, the percentage of clinicians involved in PPOs calculation rose to 70%, and 100% of participants found the digital tool useful, not only for PPOs calculation (74%) but also for data storage (19%) and sharing (7%; Table 1).
Internal survey with 27 clinicians who are members of the lung resection surgery team before and after the introduction of PreParAPP MSD.

Discussion
Although most of the sample (93%) knew about PPOs and the guidelines prescribing their use, only a small percentage of them (18%) calculated them in a preoperative evaluation. Therefore, in this specific scenario, there is not a lack of knowledge, but rather the integration of the guidelines into standard practice is still incomplete.
The implementation of a digital tool may help to improve adherence to the guidelines, in accordance with other experiences in which such tools represented the start of various quality-improvement purposes throughout the medical field. 6 The process of successfully implementing a clinical practice guideline to transform day-to-day practice is rather challenging. An investigation in a Canadian hospital found that non-compliance with published guidelines regarding preoperative assessment varies widely (5–98%). 7 This implies that the introduction of a digital tool to implement a clinical guideline may play a crucial role. 8
Previous experiences have shown that the implementation of new guidelines conveyed through memoranda, lectures and printed material did not lead to any significant adherence to the new guidelines.9,10 Improved strategies are essential in order to translate guidelines into practice, and the implementation of a guideline via a user-friendly digital tool, which can be integrated into a general practitioner’s software or in a specialised hospital, seems most promising according to Flamm et al.’s results. 11
Further evidence comes from the experience of Beinbridge et al. They state that only the theoretical knowledge of guidelines may not be sufficient, reporting that although the sharing of the guidelines of the various scientific societies is global, the rate of improvement in perioperative mortality over time is significantly related to the Human Development Index (a statistic composite index of life expectancy, education and per-capita income indicators), and this might be the result of the capability of wealthier countries to increase health-care investment in the technologies, techniques and training necessary to improve patient health. 12 Therefore, digital and technological support continues to be fundamental in order to put into practice the correct theoretical knowledge.
In this case, according to the survey, there was cultural resistance to reorganisation in the perioperative lung resection surgery department, and therefore we thought that this digital device could facilitate this task by ensuring that the calculation of PPOs becomes a priority in the preoperative assessment of lung resection surgery. In our experience, this digital tool has been useful for improving the application of guidelines in thoracic surgery preoperative assessment. The percentage of clinicians involved in the calculation of PPOs rose from 18% to 70%. Moreover, such a tool offers the possibility of collecting different perspectives on the same subject, depending on the clinic specialist’s point of sight: pulmonologists can tailor more precisely the intensity level of respiratory physiotherapy for the patients (high intensity vs. home based), or they may opt for a more aggressive drug therapy in order to obtain PPOs compatible with the threshold for medical operability without having to wait for surgeons or anaesthesiologists. Likewise, surgeons can easily simulate more or fewer extended surgical options, keeping the resection in line with the calculated PPOs. Once respiratory evaluation has been performed by using PPOs and all the possible therapies – rehabilitation and surgical alternatives – have been tested, then and only then can anaesthesiologists focus on other existing co-morbidities, but the basic prerequisite before starting the preoperative assessment should be the PPOs.
Furthermore, another of the hypothetical uses of such tool could be its use in the extra-hospital network, for instance providing general practitioners with a way to monitor patients’ respiratory status and their compatibility with surgery. Once general practitioners have been properly informed about the lung resection to be performed, they may manage their patients’ respiratory physiotherapy or suggest new drug regimens.
Footnotes
Acknowledgements
We thank Dr Vanni Agnoletti for the seed that made the plant germinate.
Contributorship
M.R. was responsible for the study design, data collection and writing the text. F.P. was responsible for the statistical analysis. S.B. was responsible for data collection. A.C. supervised the study.
Conflict of interest
The author(s) declared following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: M.R. is the scientific manager of the digital tool used in this paper and has been an invited speaker for MSD in 2017.
Ethical approval
I confirm that Ethical Committee approval was sought and is acknowledged within the text of the submitted manuscript.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
M.R. is the guarantor for this paper.
Peer Review
This manuscript was reviewed by Dr. Francesco Petrella and Dr. Vanni Agnoletti.