
Abstract
Case series summary
This case series documents the occurrence of isorhythmic atrioventricular dissociation (IAVD) in three anesthetized cats. There are several proposed mechanisms for the development of this dysrhythmia. The cardinal feature of IAVD is that the atrial and junctional rates are roughly equivalent, which aids in ruling out more severe types of atrioventricular dissociation (such as complete heart block), where atrial and ventricular rates are different. Two cats were treated with anticholinergic medication when hemodynamic variables indicated that the loss of coordinated cardiac conduction had negatively affected cardiovascular function as indicated by arterial hypotension. In one cat, IAVD was not considered to negatively affect the cat’s hemodynamic status and anticholinergic medication was not administered. In this cat, IAVD spontaneously resolved.
Relevance and novel information
Although this rhythm disturbance has been clinically recognized to manifest in domestic felids under general anesthesia, there remains a paucity of literature regarding the development, recognition and treatment of IAVD in this species. From extensive clinical experience, the authors consider this rhythm to occur frequently in clinical practice, and it behooves the feline anesthetist to be familiar and comfortable with the recognition and treatment of this dysrhythmia.
Keywords
Introduction
Atrioventricular (AV) dissociation is a collection of cardiac conduction abnormalities that result in independent electrical and mechanical activity of the atria and ventricles. 1 Resultant cardiac dysrhythmias can range from benign, such as isorhythmic atrioventricular dissociation (IAVD), to pathologic, such as third-degree AV block.1,2 These dysrhythmias can occur secondarily to pathologic changes within the cardiac conduction pathway, deceleration of the dominant pacemaker (sinoatrial [SA] node) or acceleration of a subsidiary pacemaker. 1 The result is a loss of sinus rhythm. Hemodynamic consequences may occur, as atrial contraction will no longer contribute to left ventricular stroke volume. 3
The electrocardiograph (ECG) during IAVD illustrates rhythmic alterations in the P-P interval and a P wave that ‘marches forward’, producing a variable PR interval, while always remaining in close proximity to the neighboring QRS complex.1,4 –6 A unique feature of IAVD is that the QRS morphology remains narrow, indicating that the subsidiary pacemaker is junctional in location. It is postulated that alterations in dominant pacemaker rates, the potential for retrograde conduction resulting in atrial capture, hemodynamic consequences of the dysrhythmia, cardiovascular reflexive responses to altered hemodynamics and the responsiveness of the SA node to accelerating forces may induce the development or resolution of IAVD.4,7,8
IAVD has been documented in the human literature, most often as solitary case reports or case series in geriatric patients with cardiac disease, during enflurane anesthesia and after pancuronium administration.9 –14 Veterinary clinical reports are limited to a case series in Labrador Retrievers and two case reports in cats.5,15,16 Although fundamental experimental research on IAVD mechanisms was performed more than five decades ago, clinical reports are scarce, giving IAVD an impression of elusivity. 7
This case series discusses IAVD in three cats under general anesthesia presented to the veterinary teaching hospital of the Université de Montréal. In the authors’ experience, IAVD is not uncommonly encountered in cats during anesthesia. The multifactorial causative nature of ECG interpretation in the presence of this dysrhythmia may complicate accurate diagnosis, potentially resulting in misdiagnosis, improper treatment or aborted procedures.
Case series description
Anesthetic records of cats that developed IAVD during anesthesia and managed by the authors were retrieved and evaluated for completeness. Information pertaining to signalment, presenting complaint, physical examination findings, relevant clinical pathology test results and procedures performed during anesthesia were collected. Anesthetic records were considered for inclusion if documentation of the timing of IAVD, printed ECG traces to validate the diagnosis, and written description of and response to treatment were available. Three cats met the inclusion criteria (Table 1).
Details regarding the signalment, surgical or diagnostic procedure, anesthetic protocol and complications for three cats that developed isorhythmic atrioventricular dissociation (IAVD) during general anesthesia
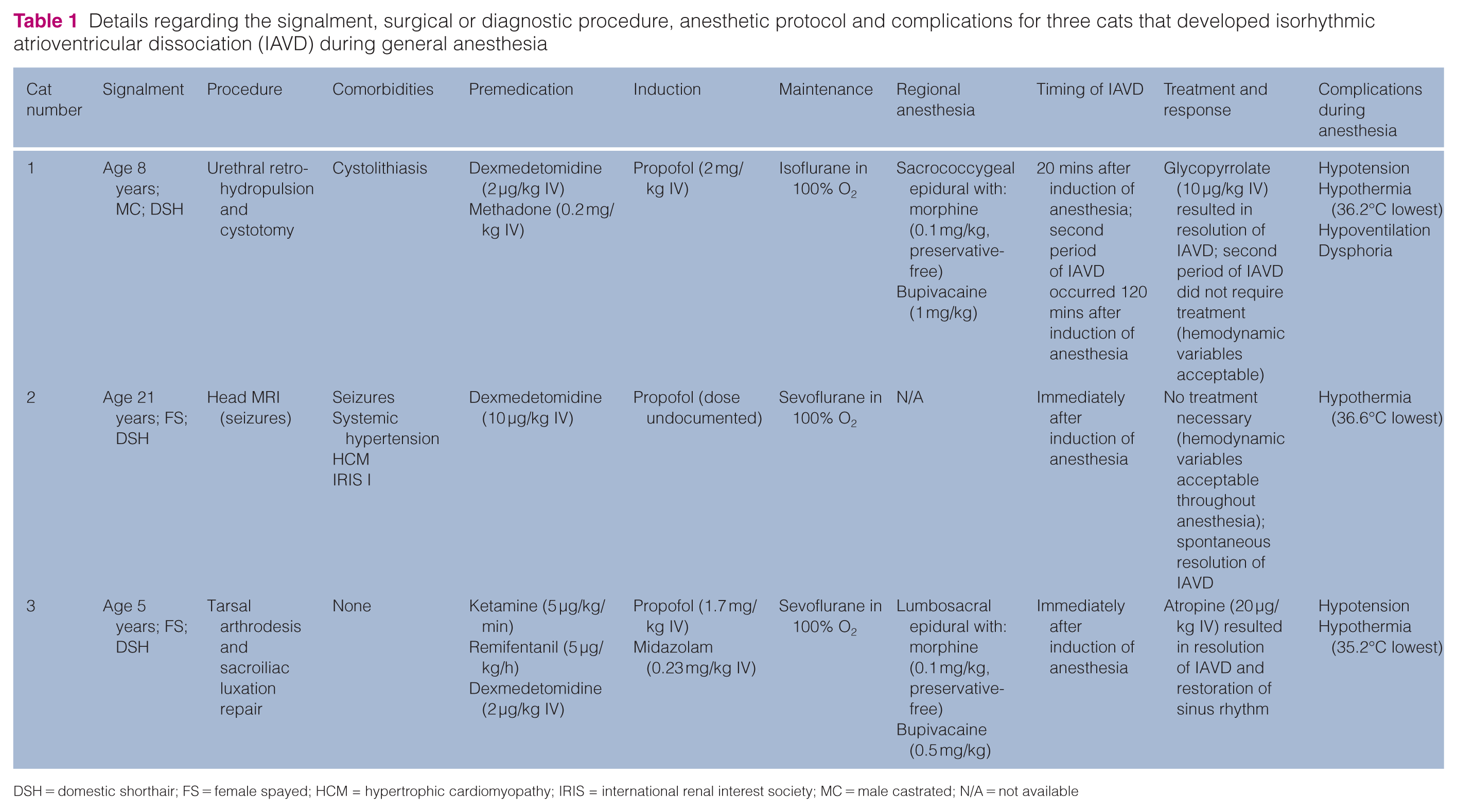
DSH = domestic shorthair; FS = female spayed; HCM = hypertrophic cardiomyopathy; IRIS = international renal interest society; MC = male castrated; N/A = not available
Cat 1 was an 8-year-old, male castrated domestic shorthair (DSH) presented for urethral retrohydropulsion and cystotomy. After urinary catheterization and 3 days of hospitalization with supportive treatment, hematology and serum biochemistry parameters were within laboratory-specific reference intervals (RIs). This cat developed IAVD on two occasions during anesthesia: once 20 mins after induction (see Video 1 in the supplementary material) and again 120 mins after induction (Figure 1a,b). The cat presented bradycardia (100 beats/min) and hypotension (mean arterial pressure [MAP] of 67 mmHg) during the first instance of IAVD (Figure 1a). Glycopyrrolate (10 µg/kg IV) restored sinus rhythm, increased heart rate (120 beats/min) and MAP (85 mmHg). Sinus rhythm was maintained for 100 mins, at which point IAVD recurred (Figure 1b). Although the cat was bradycardic (115 beats/min), MAP remained clinically acceptable (78–83 mmHg); therefore, treatment was not pursued.

Lead II electrocardiograph (ECG) traces acquired from cats 1–3 documenting isorhythmic atrioventricular dissociation (IAVD) during general anesthesia. (a) ECG trace (40 mm/mV, 25 mm/s) from cat 1 showing that the P wave (arrowhead) ‘marches forward’ to sequentially precede, superimpose or succeed the QRS complexes within the same tracing, while atrial and ventricular rates remain the same (107 beats/min). A tracing of the invasive blood pressure (asterisk) indicates relative hemodynamic stability during this period of IAVD. (b) ECG trace (40 mm/mV, 25 mm/s) from cat 1 several minutes after (a), showing synchronization of the atria and ventricles without significant changes in heart rate (108 beats/min) or invasive blood pressure (asterisk). Restoration of sinus rhythm occurred spontaneously, without administration of anticholinergic medication. (c) ECG trace (20 mm/mV, 50 mm/s) from cat 2 showing a ‘marching forward’ P wave (arrowhead) and variable QRS morphology, indicating the presence of a subsidiary pacemaker (arrow) controlling ventricular contraction during IAVD or restoration of sinus rhythm with the sinoatrial node as the dominant pacemaker (open arrow) during brief periods of synchronization. The atrial and ventricular rates are the same (120 beats/min). Treatment was not indicated, as hemodynamic variables (heart rate, invasive blood pressure) were stable and clinically acceptable throughout anesthesia. (d) ECG trace (40 mm/mV, 25 mm/s) from cat 3 showing a ‘marching forward’ P wave (arrowhead) and altered QRS morphology during IAVD due to control of ventricular contraction by a subsidiary pacemaker. Owing to hemodynamic instability (115 beats/min, mean oscillometric blood pressure of 50 mmHg), this cat received 20 µg/kg IV of atropine. A fusion beat is present on this tracing (vertical line). (e) ECG trace (40 mm/mV, 25 mm/s) from cat 3 approximately 7 mins after the administration of atropine showing the restoration of sinus rhythm and an increase in heart rate (160 beats/min). Not shown is the concomitant increase in mean oscillometric blood pressure (100 mmHg)
Cat 2 was a 21-year-old, female spayed DSH presented for investigation of seizures. The cat received amlodipine (0.625 mg PO q12h) for systemic hypertension and had hypertrophic cardiomyopathy (American College of Veterinary Internal Medicine B1) associated with grade II/VI left parasternal systolic heart murmur. 17 Clinicopathologic abnormalities were as follows: azotemia (creatinine 165 µmol/l [RI 35–164]; urea 16.86 mmol/l [RI 4.10–10.80]), hypercholesterolemia (4.85 mmol/l [RI 1.81–3.88]) and hyperproteinemia (86 g/l [RI 59.6–80.8]) with hyperglobulinemia (58.2 g/l [RI 29.0–47.0 g/l]). Azotemia was considered stable by the referring veterinarian after dietary modification. IAVD developed immediately after induction and was observed throughout the anesthetic (Figure 1c). Despite IAVD and persistent bradycardia (105–120 beats/min), MAP remained clinically acceptable (70–80 mmHg) and treatment was not pursued.
Cat 3 was a 5-year-old, female spayed DSH presented with right tarsal subluxation and left sacroiliac luxation resulting from unwitnessed trauma. Hematology and serum biochemistry parameters were within laboratory-specific RIs. The patient received remifentanil (5 µg/kg/h), ketamine (5 µg/kg/min), meloxicam (0.05 mg/kg SC q24h) and gabapentin (10 mg/kg PO q12h) during hospitalization. This cat developed IAVD immediately after induction of anesthesia (Figure 1d). Due to bradycardia (115 beats/min) and hypotension (MAP of 50 mmHg), atropine (20 µg/kg IV) was given, which restored sinus rhythm, increased the heart rate (160 beats/min) and MAP (100 mmHg) within minutes (Figure 1e).
Discussion
IAVD exists in two forms. 5 Type I IAVD is characterized by rhythmic oscillations in the duration of the P-R interval and position of the P wave, such that the P waves precede (positive P-R period), occur simultaneously or succeed the QRS (negative P-R period), without ever occurring in the ST segment.5,7 Type I IAVD is also characterized by the presence of independent atrial and junctional pacemakers, which approximate the same rate. 18 Type II IAVD is a sustained AV junctional rhythm resulting in a consistent location of the P wave, typically within the QRS complex, the S-T segment or early in the T wave.8,12 True AV dissociation may only occur transiently in type II. The ECG traces presented in this case series are illustrative of type I (Figure 1).
IAVD is a physiologic dysrhythmia, with a negative feedback loop involving baroreceptor reflex and its response to changes in blood pressure (BP). 2 Dissociation of the atria from the ventricles may result from a deceleration of the primary pacemaker or an acceleration of a subsidiary pacemaker, which is junctional in location in the case of IAVD. 8 Whatever the initiating event, the SA node and the junctional pacemaker fire at approximately the same rate. 18 Due to the asynchronous contraction of atria and ventricles, the loss of the ‘atrial kick’ may result in reductions in cardiac output and BP. Decreases in BP activate the baroreceptors, which reduce parasympathetic input to the SA node, thus accelerating the SA nodal firing rate. As the SA rate increases, synchronization between atria and ventricles occurs, resulting in restoration of sinus rhythm and increased BP. Baroreceptor activation consequently increases parasympathetic input to the SA node, leading to a decreased SA firing rate and resulting in loss of AV synchronization.2,7,12 In this sense, IAVD can occur in a self-perpetuating cycle due to the SA node acceleration-deceleration activity in response to cyclical changes in baroreceptor activity.
In humans, IAVD has been associated with several drugs, including nitrous oxide, halogenated volatile anesthetics, opioids, epinephrine, atropine, pancuronium, anticholinesterase inhibitors and digitalis.9 –12,14 In one report, IAVD occurred in up to 15% of enflurane-anesthetized patients. 10 Treatment is achieved with drugs that restore sinus rhythm via increased SA node activity or decreased junctional pacemaker activity, such as anticholinergics or beta-adrenergic receptor antagonists, respectively.9,19,20 Treatment for IAVD during anesthesia should be pursued in patients who experience hemodynamic consequences, as in cats 1 and 3, when there is evidence of hypotension likely due to the loss of atrial stroke volume.
It is possible that IAVD developed secondarily to slowing of the dominant pacemaker in this case series. All cats received some combination of dexmedetomidine, volatile anesthetic and propofol. Two cats received a mu-opioid agonist. Alpha-2 adrenoceptor agonists, such as dexmedetomidine, cause vasoconstriction, resulting in baroreceptor-mediated bradycardia, which is maintained via centrally mediated sympatholysis, thus preserving cardiac vagal efferent activity. 21 Methadone possesses calcium channel-blocking activity, which reduces the SA rate and slows AV conduction velocity. 22 Remifentanil suppresses SA and AV nodal functionality, although its effect on parasympathetic tone has yet to be elucidated.23,24 Propofol has a direct inhibitory effect on SA node automaticity, resulting in bradycardia in the clinical setting. 25 Halogenated agents are notoriously arrhythmogenic due to multifactorial and complicated mechanisms, including alterations in cardiac sodium, calcium and potassium homeostasis, catecholamine reuptake and neuronal ion channel functionality. 26 Therefore, it is conceivable that any of these drug combinations could reduce the SA nodal rate into junctional pacemaker range, thus resulting in IAVD. Cats as a species have high escape rates in the range of 80–140 bpm, which helps them to maintain relative hemodynamic stability even in the presence of pathologic AV dissociation.5,27,28 Perhaps the high escape rate in this species predisposes them to IAVD development in the anesthetic period, where use of negative chronotropic drugs is inevitable.
In a previous report, IAVD was diagnosed in a cat suffering hypothermia. 5 Hypothermia can affect the cardiovascular system in a variety of ways, potentially resulting in bradycardia and the development of dysrhythmias. 29 Hypothermia notably affects cardiac conduction via alterations in potassium, sodium and calcium homeostasis, resulting in decreased pacemaker rate, prolonged action potential duration and slowed conduction velocity.5,29,30 Although mild hypothermia (35.2–37.5°C) could have contributed to the development of IAVD in these cats, bradycardia typically occurs at lower body temperatures (<32°C in humans) and it can be resistant to anticholinergic therapy. 30 Cats 1 and 3 showed acceptable response to anticholinergic therapy, suggesting that hypothermia was not the dominant or sole causative factor. 30
Increased vagal tone due to existing comorbidities or surgical manipulation cannot be ruled out as contributing factors in the development of IAVD in these cats. Although cat 2 had documented myocardial disease and pre-existing comorbidities, the presence of a conduction impairment was not documented. Cats 1 and 3 did not present with cardiac murmurs; however, echocardiographic examination was not undertaken, so it is not possible to rule out occult cardiac disease. Cat 3 had a history of unwitnessed trauma, which itself can be associated with dysrhythmia due to traumatic myocarditis, as documented in dogs. 31 Anesthesia in cat 3 occurred more than 5 days after the traumatic incident, and no dysrhythmia was noted during telemetric monitoring. In dogs, dysrhythmias from traumatic myocarditis tend to appear within 24–48 h of injury. 31 Furthermore, IAVD is a physiologic dysrhythmia, and traumatic myocarditis is classically associated with pathologic dysrhythmias, such as ventricular premature contractions, ventricular tachycardia and ventricular fibrillation. 31
Conclusions
Continuous ECG monitoring will aid in the recognition, diagnosis and treatment of IAVD. It is imperative to differentiate IAVD from other types of AV dissociation, which can be pathologic and require specific treatment. Improved education on ECG interpretation may increase patient safety while avoiding unnecessarily aborted anesthetic procedures in clinical practice, particularly in the perianesthetic period where the use of negative chronotropic drugs is essentially inevitable.
Footnotes
Supplementary material
The following file is available as supplementary material: A video of a continuous lead II electrocardiograph (ECG) from cat 1 during isorhythmic atrioventricular dissociation, before the administration of glycopyrrolate via the intravenous route.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognized high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed and/or this work involved the use of cadavers. Ethical approval from a committee was therefore not specifically required for publication in JFMS Open Reports. Although not required, where ethical approval was still obtained, it is stated in the manuscript.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (experimental or non-experimental animals, including cadavers, tissues and samples) for all procedure(s) undertaken (prospective or retrospective studies). No animals or people are identifiable within this publication, and therefore additional informed consent for publication was not required.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.