
Abstract
Background:
The airway of an anesthetized patient should be secured with an artificial airway for oxygenation or ventilation. Pediatrics are not small adults which means they are different from adults both anatomically and physiologically. This study aims to determine the prevalence of difficult airway and its associated factors in pediatric patients who underwent surgery under general anesthesia in referral hospitals of Addis Ababa.
Methods:
A multi-centered cross-sectional study design was employed. The bivariable and multivariable logistic regression was used to measure the association between the dependent variable (pediatrics difficult airway) and independent variables. p-value < 0.05 was used to declare statistical significance.
Results:
A total of 290 pediatrics patients were included in this study. The prevalence of difficult airway in pediatrics patients who underwent surgery was 19.7%. In multivariate logistic regression, pediatrics patients less than 2 years of age (adjusted odds ratio = 6.768, 95% confidence interval = 2.024, 22.636), underweight pediatrics patients (adjusted odds ratio = 4.661, 95% confidence interval = 1.196, 18.154), pediatrics patients having anticipated difficult airway (adjusted odds ratio = 18.563, 95% confidence interval = 4.837, 71.248), history of the difficult airway (adjusted odds ratio = 8.351, 95% confidence interval = 2.033, 34.302), the experience of anesthetists less than 4 years of age (adjusted odds ratio = 9.652, 95% confidence interval = 2.910, 32.050) had a significant association with pediatrics difficult airway.
Conclusion:
Being pediatric patients less than 2 years of age, underweight pediatrics patients, having anticipated difficult airway, those anesthetists who do not perform enough pediatric cases were identified as the main factors associated with the greater occurrence of difficult airway in pediatric patients.
Introduction
One of the tasks of an anesthetist is securing the airway of patients with an artificial means that involves mask ventilation (MV) and endotracheal intubation.1–3 The difficult airway is one of the most common complications of the airway. Hypoxia, esophageal intubation, and difficult endotracheal intubation (DETI) are the reasons for problems with the airway. Around 17% of the respiratory-related problems resulted from difficult intubation, and about 28% of all anesthesia-related mortality is due to difficult intubation or ventilation. 1
Pediatrics have a large tongue, large head, anterior larynx, smallmouth, narrow airway, and low functional residual capacity, and they are hard to intubate.3–8 MV, direct laryngoscopy, and endotracheal intubation could be relatively difficult in pediatric patients.
A patent and secure airway is needed to manage anesthetized or critically ill patients. 9 Different kinds of literature show that pediatrics cannot tolerate a period of hypoxia when compared to adults. When they are hypoxic, they will be bradycardic and might develop cardiac arrest. Difficulty in securing the airway of pediatric patients is not uncommon in anesthesia practice and results in morbidity and mortality of patients.10–14
Assessing the airway parameters like the oropharyngeal view, thyromental distance, hyomental distance, or other predictors of difficult airway in pediatrics patients is difficult in managing difficult airway case scenarios.13,15–17 Studies regarding difficult airways in pediatric patients were not established well in developing countries like Ethiopia. Therefore, this study aims to determine the prevalence of difficult airway and its associated factors in pediatric patients who underwent surgery under general anesthesia in referral hospitals of Addis Ababa.
Methods
Study design, setting, and participants
This is a multi-centered cross-sectional study was conducted in referral hospitals of Addis Ababa. There are 13 governmental hospitals, from which pediatric surgical procedures are done in 12 hospitals. This study was conducted in five government hospitals (Tikur Anbessa Comprehensive Specialized Hospital, Zewditu Memorial Hospital, Yekatit 12 Hospital Medical College, Minilik II Hospital, and St. Peter Hospital). The study participants were pediatric patients who underwent elective surgical procedures under general anesthesia from 30 December 2019 to 30 March 2020. This study is reported in line with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) checklist 18 and registered at www.researchregistry.com with Research Registry UIN: researchregistry6269.
Inclusion/exclusion criteria
The pediatric patients falling in the classification of American Society of Anesthesiologists (ASA) class I and II; elective surgical procedures; pediatrics patients who require endotracheal intubation; age 0–5 years were included in this study while pediatric patients undergoing surgical procedures under endotracheal intubation under indirect laryngoscopy technique; and pediatric patients whose airway were secured with anesthesia students were excluded.
Sample size and sampling procedure
The sample size was determined using finite population correction formula by assuming the prevalence as 0.5 (since no previous study of similar setup); 5% margin of error; 95% confidence interval (CI); and 10% non-response rate, and therefore, a total sample size of 290 elective surgical patients have participated in this study. A stratified random sampling technique was used to get the required sample size during the study period. The daily operation schedule list was used as a sampling frame. A situational analysis and logbook review showed that during a 3-month period, 300 elective pediatric surgeries are done in Tikur Anbessa Comprehensive Specialized Hospital, 144 in Zewditu Memorial Hospital, 144 in Yekatit 12 Hospital Medical College, 180 in Minilik Hospital, and 72 in St. Peter Hospital. So during the study period, a total of 840 pediatric patients underwent elective surgery. Since the calculated sample size is 290 (n), to find k, we divide 840 (N) by 290 (n) is 2.9. When we divide the total pediatric elective surgery in 3 months by 2.9, we will have (300/2.9) = 103 elective pediatric patients undergoing surgery at Tikur Anbessa Comprehensive Specialized Hospital, 144/2.9 = 50 in Zewditu Memorial Hospital, similarly 50 in Yekatit 12 Hospital Medical College, 180/2.9 = 62 in Minilik Hospital, and 72/2.9 = 25 in St. Peter Hospital. The first patient was chosen by lottery method, and then every third patient was chosen for the study.
Data collection technique
Data were collected, and a structured questionnaire was prepared and pretested on 5% (15 patients) of the sample size. Elective pediatric patients scheduled for surgery under general anesthesia requiring endotracheal intubation were assessed at the waiting room by the trained data collectors immediately before they entered the operation room. Then, each patient who underwent endotracheal intubation was observed for difficult intubation, difficult laryngoscopy (DL), and difficult MV in the operation room. The Cormack and Lehane’s laryngoscopy grade of the patient was determined by the anesthetist who performed the laryngoscopy as well as training was given for the data collectors about the Intubation Difficulty Scale Score (IDSS). An observational data collection technique was used in this study. Han’s scale 19 for MV was used for assessing difficult MV.
Operational definitions
Difficult airway: an experienced anesthetist encounters difficulty with any or all of face MV, laryngoscopy, and tracheal intubation during securing the airway with an endotracheal tube for surgical procedures. 20
Difficult face MV: the Han MV Grade III or Grade IV (Grade III—difficult ventilation (inadequate, unstable, or requiring two providers) with or without muscle relaxant and Grade IV—unable to mask ventilate with or without muscle relaxant). 19
DL: the presence of the Cormack and Lehane Grade III or IV (Grade III—visualization of the only epiglottis and Grade IV—visualization of just the soft palate). 21
Difficult tracheal intubation: IDSS of greater than 5 (IDSS score of greater than 5 has a moderate to major difficulty). 22
Data analysis
Data were entered into Epi-info version 7, and then exported to SPSS version 22 for analysis. All independent variables were analyzed using binary logistic regression with the dependent variable, difficult airway, and those with a p-value of <0.2 from the bivariable analysis were fitted to a multivariate logistic regression to check their association with a difficult airway. The odds ratio, 95% CI, and p-value were computed to identify associated factors and to determine the strength of the association. The p-values of <0.05 were considered to be statistically significant. The Hosmer–Lemeshow test of goodness of fit was performed to check the appropriateness of the analysis model.
Data quality control
To assure the quality of data, training on the objectives and relevance of the study, and brief orientations on the assessment tools were provided for data collectors. A pretest was done before data collection for its accuracy, clarity, and consistency. During data collection, each questionnaire was revised by the investigator for being complete and appropriate.
Ethics approval and informed consent
Ethical clearance and a letter of permission to conduct were obtained from Addis Ababa University Ethical review board. Informed written consent was secured from every study participant’s guardians who have legally authorized representatives of pediatrics patients. Confidentiality and anonymity were ensured.
Results
Demographic characteristics of study participants
A total of 290 pediatric patients who underwent surgical procedures under general anesthesia and endotracheal intubation were included in this study. The mean weight was 8.8 kg with a standard deviation of 4.5 kg. From the total sample, 64.8% were male, and 61.4% of patients were underweight (Table 1).
Demographic characteristics of pediatric patients who underwent surgery under general anesthesia in referral hospitals of Addis Ababa.
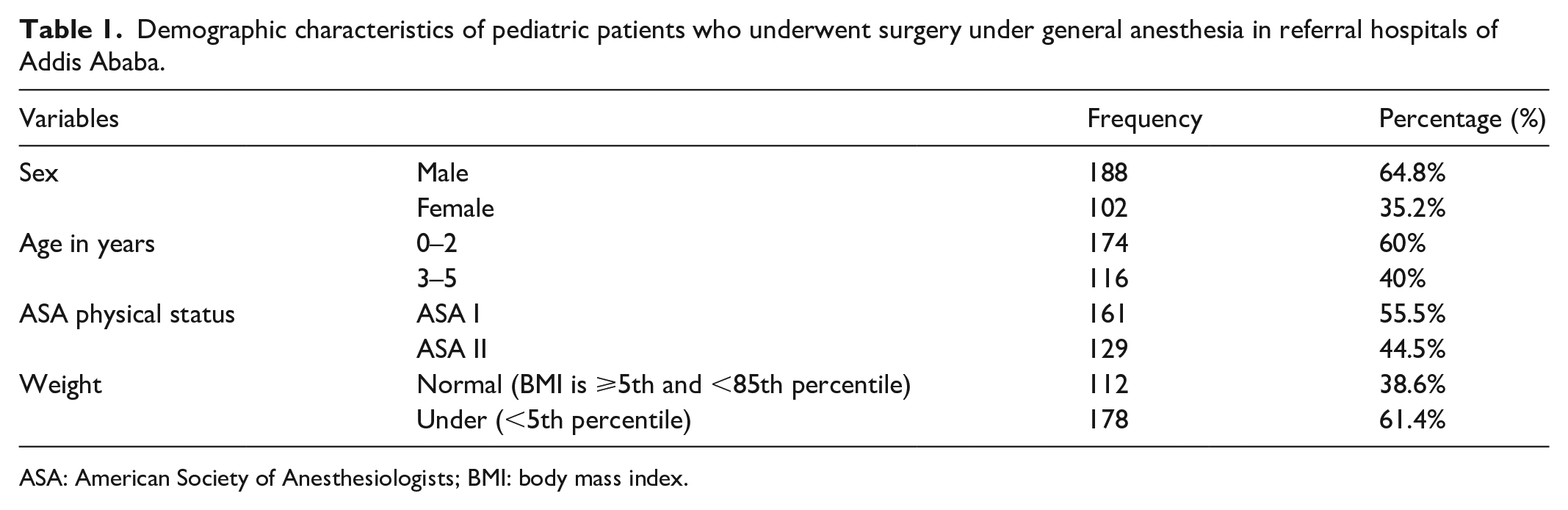
ASA: American Society of Anesthesiologists; BMI: body mass index.
Prevalence of difficult intubation, DL, difficult MV, and difficult airway
In this study, we found the prevalence of difficult intubation as 32/290 (11%), DL as 21/290 (7.2%), difficult MV as 16/290 (5.5%), and difficult airway as 57/290 (19.7%).
We found that IDSS was easy on 119/290 (41%), slight difficulty on 139/290 (47.9%), and moderate to major difficulty on 32/290 (11%) of pediatric patients who underwent surgery under general anesthesia in referral hospitals of Addis Ababa. The majority (69.7%) of pediatrics patients had the Cormack and Lehane Grade of Laryngoscopy (CLGL) I, 23.1% of pediatrics patients had the CLGL II, and 7.2 of pediatrics patients had the CLGL III. This study showed that the HAN MV Grade I, II, and III were 92.4% versus 82.4%, 2.1% versus 11.4%, and 5.5% versus 6.2% before and after muscle relaxant was administered, respectively.
Anesthesia and surgery-related variables
An excessive gas leak was observed in 6.2% of patients, and 17.9% of patients required more than two persons to ventilate (Table 2).
Factors related to mask ventilation of pediatric patients who underwent surgery under general anesthesia in referral hospitals of Addis Ababa.

For this study, the number of laryngoscopies was done in 67.93% of the patients, and the Miller-type laryngoscope blade was used in 15.17% of the study participants (Table 3).
Laryngoscope-related factors of pediatric patients who underwent surgery under general anesthesia in referral hospitals of Addis Ababa.

For this study, the original endotracheal tube was changed in 29.3% of patients. The cuffed endotracheal tube was used in 23.8%, and intubation attempt was single in about 81% of the patients (Table 4).
Endotracheal intubation-related factors of pediatric patients who underwent surgery under general anesthesia in referral hospitals of Addis Ababa.

In this study, 100 (34.48%) patients were undergone general surgery, 103 (35.52%) patients were undergone maxillofacial surgery, and 87 (30%) patients were undergone neurosurgery.
Factors associated with difficult airway
In multivariable logistic regression, pediatrics patients age of 0–2 years (adjusted odds ratio (AOR) = 6.768, 95% CI = 2.024, 22.636); underweight pediatrics patients (AOR = 4.661, 95% CI = 1.196, 18.154); pediatrics patients having anticipated difficult airway (AOR = 18.563, 95% CI = 4.837, 71.248); pediatrics patients having a history of the difficult airway (AOR = 8.351, 95% CI = 2.033, 34.302); anesthetist who are working less than 4 years (AOR = 9.652, 95% CI = 2.910, 32.015) were found to be associated with pediatrics patients difficult airway (Table 5).
Factors associated with the difficult airway of pediatric patients who underwent surgery under general anesthesia in referral hospitals of Addis Ababa.

OR: odds ratio; CI: confidence interval; AOR: adjusted odds ratio.
Discussion
Pediatrics patients have relatively more difficult MV, direct laryngoscopy, and endotracheal intubation as compared to adults.7,23,24 The intubation difficult scale is a blend of subjective and objective criteria that permit a qualitative and quantitative approach to the progressive nature of the difficulty of intubation. 25
On day-to-day practice, we have used endotracheal tubes of an appropriate size determined by calculation for pediatric patients who underwent surgery.26,27 However, most Ethiopian children are underweight, and we usually use tubes smaller than the actual calculated endotracheal tubes.
In this study, we found that the prevalence of difficult airway was 19.7% and DL was 7.2%, in pediatric patients who underwent surgical procedures at Addis Ababa Referral Hospitals, which is higher than in other studies that the incidences of DL were 4.77%, 28 1.3%, 29 1.37%, 30 2.95%, 31 4%, 32 and 3%. 33
This study reveals that the incidence of difficult MV was 5.5%. Similarly, El-Orbany and Woehlck 34 reported that the incidence of difficult MV varies widely from 0.5% to 15%. In another study which is conducted on patients between 0 and 8 years, the incidence of difficult bag-MV was 6.6%. 35 In a study done in India on pediatric patients age 1–5 years, the incidence of difficult MV was 3%, and similarly to our finding, the grade of difficult MV had improved after relaxant was given. 36
We found that the incidence of difficult intubation was 11%, which is higher compared to other studies conducted in infants at Osaka City General Hospital 2.4%, 9 and in Canada at the Hospital for Sick showed that 0.5% of pediatrics patients had difficult intubation. 37
This study showed that small age (0–2 years), underweight children, anticipated difficult airway from history and physical examination, children who had difficult airway history, and anesthesiologists who do not perform enough pediatric cases also will have difficulties in managing difficult airway (less than 4 years of experience) had a significant association with a difficult airway. In line with our finding, a study done in the pediatric intensive care unit showed that a history of difficult airways and less experienced providers were associated with difficult airways. 38 Studies showed that there was a significant association between small age and difficult airway.30,31,36 The main limitation of this study is it only focuses on the prevalence of difficult airway in pediatrics age groups other than other surgical patients that could have difficulties in securing the airway.
Conclusion
The prevalence of difficult airway in pediatric patients who underwent surgery was high. Pediatric patients less than or equal to 2 years, who are underweight, those who had a history of difficult airway and anticipated difficult airway, and those anesthetists who do not perform enough pediatric cases were identified as the main factors associated with the greater occurrence of difficult airway in pediatrics patients.
Supplemental Material
sj-docx-1-smo-10.1177_20503121211052436 – Supplemental material for The prevalence of difficult airway and its associated factors in pediatric patients who underwent surgery under general anesthesia: An observational study
Supplemental material, sj-docx-1-smo-10.1177_20503121211052436 for The prevalence of difficult airway and its associated factors in pediatric patients who underwent surgery under general anesthesia: An observational study by Eleni Amaha, Lydia Haddis, Senait Aweke and Efrem Fenta in SAGE Open Medicine
Supplemental Material
sj-docx-2-smo-10.1177_20503121211052436 – Supplemental material for The prevalence of difficult airway and its associated factors in pediatric patients who underwent surgery under general anesthesia: An observational study
Supplemental material, sj-docx-2-smo-10.1177_20503121211052436 for The prevalence of difficult airway and its associated factors in pediatric patients who underwent surgery under general anesthesia: An observational study by Eleni Amaha, Lydia Haddis, Senait Aweke and Efrem Fenta in SAGE Open Medicine
Footnotes
Acknowledgements
The authors acknowledge the Addis Ababa University.
Author contributions
EA, LH, SA, and EF were involved in the data collection, data analysis, and manuscript preparation. All authors agree, read, and verify the manuscript for publication.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from the Addis Ababa University Ethical Review board with the Ethical Approval no. 10/19/Anes.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Addis Ababa University.
Informed consent
Informed written consent was secured from every study participant guardians who were legally authorized representative of pediatrics patients.
Data sharing statement
Data will be shared upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.