
Abstract
Case summary
A 14-year-old, female spayed domestic shorthair cat presented with a 2-day history of lethargy and intermittent vomiting. Abdominal ultrasonography identified biliary obstruction with several choleliths, dilation and thickening of the intrahepatic biliary ducts and a mass-like lesion was identified in the right medial liver lobe, attached to the gallbladder. Cholecystectomy and partial liver lobectomy were performed to treat biliary obstruction and remove the mass lesion, respectively. Histopathological examination of the hepatic mass confirmed the diagnosis of biloma.
Relevance and novel information
Bilomas and biliary pseudocysts are considered uncommon findings in cats. This is the first reported case of spontaneous biloma in a cat associated with biliary obstruction secondary to cholelithiasis and presumptive previous history of biliary peritonitis. Non-iatrogenic causes, such as gallbladder rupture, should be considered in the differential diagnosis of feline biloma.
Plain language summary
A 14-year-old cat was brought to the clinic after 2 days of being very tired and occasionally vomiting. An ultrasound scan showed that the tubes carrying bile from the liver were blocked by gallstones, and there was also a mass in the liver near the gallbladder. The cat underwent surgery to remove the gallbladder and part of the affected liver. Laboratory examination of the removed tissue confirmed that the mass was a biloma, which is a pocket of leaked bile surrounded by scar tissue. Bilomas are rare in cats. This is the first reported case of a biloma that developed on its own (not caused by a medical procedure) and was linked to gallstones and a suspected past episode of bile leakage into the abdomen. The case highlights that gallbladder rupture and other non-procedural causes should be considered when diagnosing bile-filled cysts in cats.
Introduction
A biloma is a bile collection outside the biliary tree but within the abdominal cavity. 1 Bile may accumulate extrahepatically or intrahepatically. 1 Leakage into hepatic interstitial tissue triggers an inflammatory response, forming a fibrous pseudocapsule, termed a biliary pseudocyst. 2 In humans, this rare condition occurs in 0.3–2.0% of cases, 1 while incidence in small animals remains unknown.
In human medicine, bilomas are typically linked to iatrogenic injury or trauma to the hepatic biliary tract. Causes include hepatobiliary procedures such as cholecystectomy, percutaneous biopsy, bile duct catheter placement and transhepatic cholangiography, as well as choledocholithiasis and surgeries like common-duct exploration, choledochoenteric anastomosis and partial hepatectomy.3 –5 In the veterinary literature, only five cases are reported: four in dogs and one in a cat. Two canine cases were iatrogenic: one after cholecystectomy following traumatic gallbladder rupture 6 ; and the other after attenuation of an intrahepatic portosystemic shunt. 7 A third, non-iatrogenic case involved an extruded gallbladder mucocele, 8 and a fourth case involved a dog bite injury. 9 The feline case occurred after a hepatic biopsy. 5
To the authors’ knowledge, this is the first reported feline case of a biloma secondary to suspected gallbladder rupture and bile peritonitis. This report describes the diagnostic approach and treatment of biloma with concurrent neutrophilic cholecystitis and obstructive cholelithiasis.
Case description
The 14-year-old, female spayed domestic shorthair cat in this report had a history of septic biliary peritonitis due to gallbladder perforation from bacterial cholangiohepatitis 4 years prior, which was managed conservatively at another centre (Table 1). Two days before referral, the cat developed progressive lethargy and intermittent vomiting and was referred for further investigations.
Summary of diagnostic tests and findings from the previous episode of hepatobiliary disease and peritonitis

At presentation, the cat was quiet, alert and responsive. Her body weight was 4.09 kg, and body condition score was 3/9, with moderate muscle wasting. Moderate jaundice was noted. Cardiac auscultation revealed tachycardia (208 bpm) and a low-grade (II/VI) left-sided systolic heart murmur. Systolic blood pressure was 160 mmHg via oscillometric device with a 2.5 cm cuff. The rest of the examination was unremarkable.
Complete blood count, coagulation, serum biochemistry, and vitamin B12 (cobalamin) and B9 (folate) levels showed several abnormalities. Haematology revealed a mild non-regenerative anaemia (Table 2). Pre-anaesthetic echocardiography showed mild discrete upper septal thickening without significant left ventricular outflow tract obstruction. Mild dynamic right ventricular outflow tract obstruction was also noted, with no treatment required.
Complete blood count, serum biochemistry, vitamin B12 and folate results before admission

Abnormal value
ALP = alkaline phosphatase; ALT = alanine transaminase; GGT = gamma-glutamyl transferase; HCT = haematocrit; HGB = haemoglobin; MCH = mean cell haemoglobin; MCHC = mean cell haemoglobin concentration; MCV = mean cell volume; RBC = red blood cell; RI = reference interval; WBC = white blood cell
The cat was premedicated with intravenous dexmedetomidine (2 μg/kg, Dexdomitor; Vetoquinol UK) and methadone (0.3 mg/kg, Comfortan; Dechra UK). Anaesthesia was induced with midazolam (0.3 mg/kg, Hypnovel; Neon Healthcare UK) at 0.3 mg/kg and alfaxalone (Alfaxan; Zoetis UK) to effect. Abdominal ultrasonography was performed using two linear transducers (RS85 Prestige; Samsung). A single, rounded, hypoechoic to anechoic mass with heterogeneous echogenicity was identified caudal to the gallbladder. The lesion lacked Doppler signal and appeared confined within the serous capsule of the right middle liver lobe (Figure 1). Differentials included haematoma, biliary pseudocyst/biloma, extruded mucocele, granuloma, abscess or neoplasia. Three choleliths were present in the common bile duct, one at the duodenal papilla, causing marked dilation of the common and intrahepatic bile ducts (8 mm). The gallbladder wall (3 mm) and bile ducts (2 mm) were thickened, with non-dependent biliary sludge in the gallbladder lumen (Figure 2). Findings indicated cholelithiasis with extrahepatic biliary obstruction and severe cholangitis. Given the ultrasound evidence of significant or complete biliary obstruction, emergency hepatobiliary surgery was elected.

Ultrasound image of the hepatic mass-like lesion (between white arrowheads) near the gallbladder with a thick capsule and heterogeneous anechoic to hypoechoic material in the centre
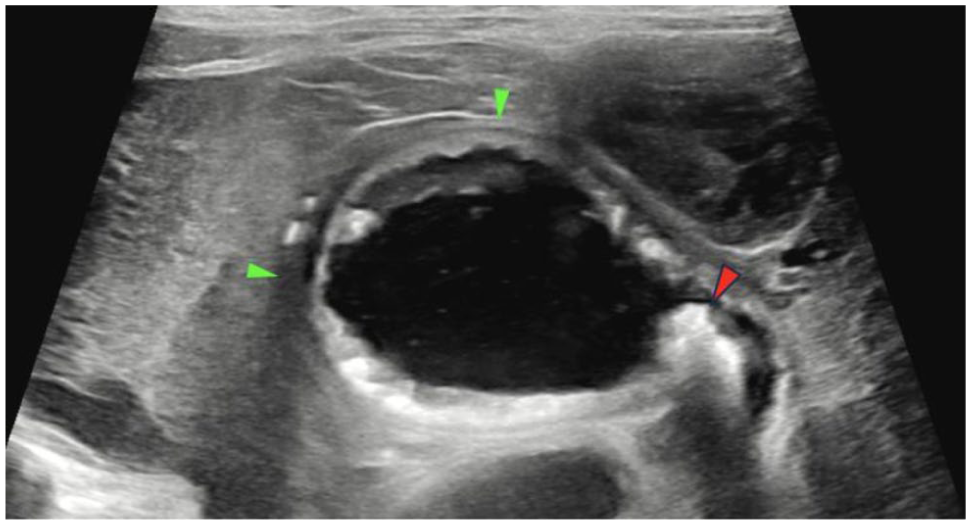
Longitudinal ultrasound image of the gallbladder with thickened wall and irregular mucosa (green arrowheads). One of the choleliths can be seen in the right of the image at the entrance of the cystic duct (red arrowhead)
A ventral midline celiotomy was performed. 10 Intraoperative exploration revealed a markedly enlarged gallbladder firmly adhered to adjacent liver lobes, particularly the right medial lobe, and a solitary, firm, well-demarcated mass originating from the medial aspect of the right medial liver lobe. The bile duct was distended and tortuous (Figure 3), with two choleliths palpated at the duodenal papilla; normograde flushing restored ductal patency. The initial plan to dissect the gallbladder from the liver and mass followed by separate excision of the mass was initiated; however, it was modified because of acute intraoperative hypotension, prompting en bloc excision of the gallbladder and mass via partial right medial liver lobectomy using a 0-metric Endoloop (Ethicon) (Figure 4). The abdominal wall was closed routinely 10 and an oesophagostomy feeding tube was placed for postoperative nutrition.
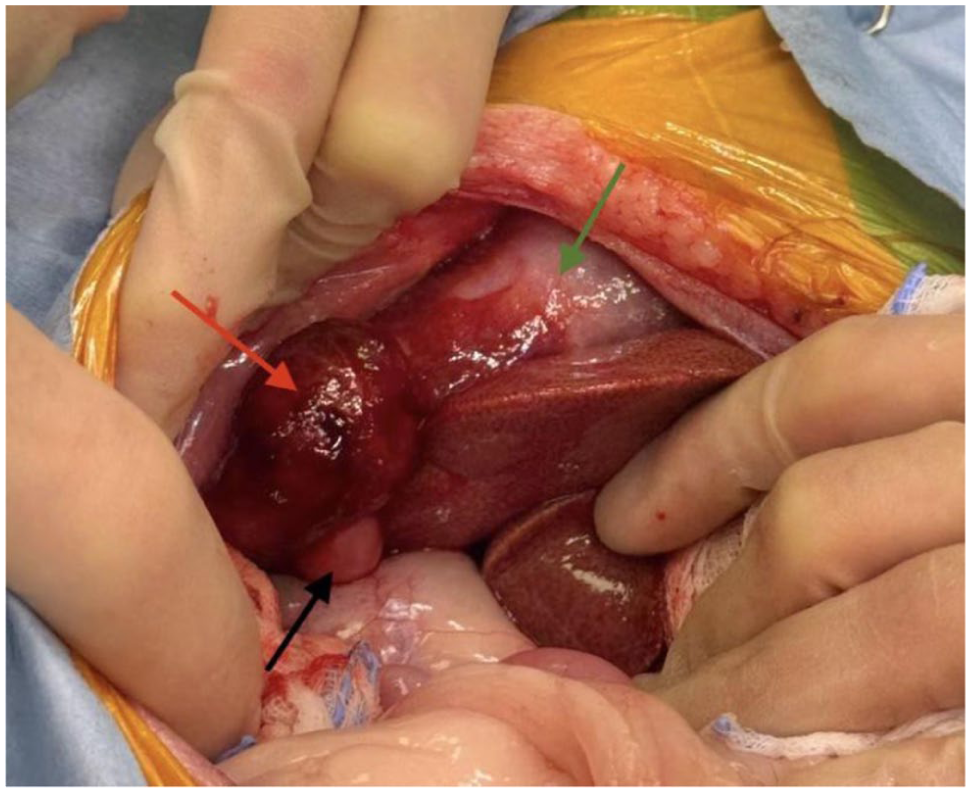
An enlarged gallbladder was observed, tightly attached to the right middle lobe (green arrow). A separate, mass-like lesion appeared as a single, firm and clearly defined structure, arising from the inner side of the right medial liver lobe (red arrow). The bile duct was significantly tortuous and distended (black arrow)

En bloc resection of the markedly enlarged gallbladder, which was firmly adhered to the right middle lobe and the biloma
Postoperatively, the cat remained severely hypotensive, unresponsive to vasopressors and intravenous oncotic support (canine plasma transfusion), but showed improvement with a continuous rate infusion of hydrocortisone 200 mg/day (Hydrocortisone sodium succinate; Panpharma). A marked postoperative haematocrit drop was initially managed with a canine xenogenic transfusion, and a complete haematology sample revealed severe anaemia with moderate left-shift neutrophilia (Table 3). As a result of subsequent haemolysis, an allogenic transfusion was administered, resulting in clinical improvement. The cat remained hospitalised with multimodal analgesia: methadone (0.2 mg/kg q4h, Comfortan; Dechra Veterinary Products), gabapentin (10 mg/kg q8h, Gabapentin; Milpharm), anti-nausea treatment (maropitant 1 mg/kg per day, Vetemex; Virbac UK) and intravenous antibiotics (amoxicillin-clavulanic acid 20 mg/kg q8h, Synulox; Zoetis). Discharge occurred 6 days postoperatively and follow-up biochemical tests showed that liver parameters had nearly returned to normal levels (Table 4).
Complete blood count profile 5 days postoperatively

Platelet clumping was observed on the blood smear; therefore, the automated platelet count should be interpreted as a minimum value. The platelet estimate on smear suggested a mild decrease, approximately 100–200 × 109/l
Abnormal value
HCT = haematocrit; HGB = haemoglobin; MCH = mean cell haemoglobin; MCHC = mean cell haemoglobin concentration; MCV = mean cell volume; RBC = red blood cell; RI = reference interval; WBC = white blood cell
Serum biochemistry on follow-up examination 6 days postoperatively

Abnormal value
ALP = alkaline phosphatase; ALT = alanine transaminase; GGT = gamma-glutamyl transferase; NH3 = ammonia; RI = reference interval
The excised gallbladder, liver mass and an incisional biopsy of grossly normal liver were fixed in 10% neutral buffered formalin for histopathology and aerobic, anaerobic and fungal culture. Fresh bile was submitted for analysis, cytology and culture. Grossly, a well-defined, mildly expansile lesion (approximately 18 mm) was present in the liver adjacent to the adhered gallbladder (Figure 5). Histologically, the lesion was encapsulated by fibrous tissue extending into the gallbladder capsule (Figure 6), lacked epithelial lining and contained minimal inflammation with lymphoid aggregates. Its contents included necrotic debris, haemorrhage, foamy macrophages, cholesterol clefts and golden-brown pigment; Perl’s Prussian blue and Fouchet stains confirmed haemosiderin and bile, supporting a diagnosis of biloma or biliary pseudocyst. Gallbladder histology showed chronic-active cholecystitis with fibrosis, while the normal liver sample revealed moderate cholangiohepatitis, biliary proliferation and periportal fibrosis. Bile analysis and cytology indicated bacterial cholangitis, and cultures from bile, gallbladder, liver and choleliths identified Staphylococcus felis and Enterococcus faecalis, both sensitive to amoxicillin-clavulanate.

Macroscopic appearance of an expansile lesion located within the liver parenchyma and immediately adjacent to the broadly adhered gallbladder

Histological section of the mass lesion, encapsulated by a fibrous tissue rim, which partially extended into the fibrous capsule surrounding the gallbladder
Follow-up 14 days postoperatively showed no abnormal clinical findings. The surgical wound had healed without incident, the external sutures were removed and the complete blood count indicated full resolution of anaemia. The final follow-up at 10 months postoperatively reported the cat had returned to normal quality of life with no recurrence of clinical signs or pain. At the time of writing this report, 11 months postoperatively, the cat remains alive and asymptomatic, demonstrating an uncomplicated recovery.
Discussion
Reports of bilomas or biliary pseudocysts in the veterinary literature are rare, with only one feline case 5 and four canine cases6 –9 documented. To our knowledge, no cases describe gallbladder perforation leading to biloma formation in small animals. This is the first reported case of a biloma or biliary pseudocyst possibly linked to gallbladder disease and suspected prior biliary perforation. In human medicine, biloma is also an uncommon complication of gallbladder perforation. However, the gallbladder is the most common perforation site within the biliary tree. 11 Intrahepatic bilomas in humans typically occur in the right upper quadrant or mid-abdomen near the porta hepatis or gallbladder, 12 similar to this case. Because of their rarity, preferred locations in veterinary species remain unknown.
This cat had a prior history of septic peritonitis of unknown origin, treated medically at another referral centre, with successful resolution after antibiotic therapy and without the need for surgery. Extension of bacterial cholangiohepatitis/bile peritonitis was suspected at that time. According to the referral records, culture, fine-needle aspiration, imaging and fluid analysis were performed (Table 1). It is hypothesised that the biliary peritonitis resulted from gallbladder perforation, with bile leakage into the adjacent medial right liver lobe, subsequently leading to the formation of the biloma, which was later confirmed on imaging and histopathology.
Differential diagnoses for intrahepatic biloma based on imaging included ectopic or duplicated gallbladder, hepatic cysts, cystic duct remnants, choledochal cysts, neoplasia, focal fluid accumulations such as haemorrhage, abscesses 5 or extruded gallbladder mucocele. 13 Although mucoceles are rare in cats, a few cases exist;14,15 however, no reports describe extruded mucoceles in cats. Bilomas are typically anechoic with posterior acoustic enhancement, sometimes containing sludge material,5,6 or appear as echoic focal hepatic subcapsular accumulations. 8 Our case differed, showing a hypoechoic to anechoic mass with heterogeneous echogenicity caudal to the gallbladder (Figure 1). In contrast, extruded mucoceles are heteroechoic, and the gallbladder has a thickened, irregular wall with no mucocele material in the lumen, and the rupture wall may not always be visible. 13 As a result of overlapping characteristics of biloma and extruded mucocele, an initial diagnosis of extruded mucocele was considered. The authors hypothesised that the lesion’s appearance and deviation from typical findings in the limited literature were likely related to its chronicity and nature. Therefore, biloma or biliary pseudocyst should be included as differential diagnoses for hypoechoic to anechoic solitary liver masses with heterogeneous echogenicity and no Doppler signal near the gallbladder, particularly if previous biliary disease is suspected. According to the literature, bilomas typically appear on CT and MRI as well-defined or mildly irregular cystic masses, generally without septations or calcifications, often surrounded by a pseudocapsule that may be difficult to distinguish; 2 however, neither modality was used in this case.
Although diagnostic imaging is important for the diagnosis of bilomas and biliary pseudocysts, histopathological examination is required for definitive diagnosis. In this case, histopathology classified the lesion as a biloma, a bile-filled pseudocyst lacking epithelial lining and enclosed by fibrous tissue within the liver parenchyma adjacent to the gallbladder. The cavity contained necrotic debris, haemorrhage and foamy macrophages; Fouchet stain confirmed bile components. The lesion showed no epithelial lining, including necrotic remnants, submucosa or glandular structures, which contrasts with gallbladder mucoceles. 16 In the veterinary literature, mucoceles are characterised by hyperplastic or cystic epithelium supported by submucosal or glandular structures. 17 Although extended inflammation or ischaemia could theoretically obliterate the epithelium, there were no histological signs suggesting this had occurred, such as basement membrane fragments, residual epithelial cells, inflammation or fibrosis. Consequently, an extruded mucocele was deemed to be unlikely; instead, features aligned with a biloma, where localised bile leakage is encapsulated by fibrous tissue without epithelial involvement.
In humans, biloma treatment typically involves percutaneous drainage, although surgery may be required for major biliary injury, unsuccessful drainage or septic bilomas. 3 In this case, surgery was chosen because of obstructive choleliths requiring biliary access and the need for liver histopathology. The obstruction was primarily caused by choleliths at the duodenal papilla, as normograde flushing restored ductal patency. The biloma adherent to the gallbladder and liver may have contributed to local compression, but its role as the primary cause is uncertain and it may represent an incidental or secondary finding. Clinical improvement likely resulted from both relief of obstruction and resolution of cholangitis. The biloma was removed with the gallbladder to prevent potential future complications and to obtain a histological diagnosis of such lesions.
Conclusions
This represents the first documented case of a non-iatrogenic cause of biloma in a cat. To our knowledge, this is the first instance of biloma attributed with suspected gallbladder perforation. Non-iatrogenic causes, such as gallbladder perforation, should be considered as a differential diagnosis in cats presenting with suspected biloma. Diagnostic imaging and histopathological evaluation are essential for establishing a definitive diagnosis. Further studies on bilomas in veterinary patients are warranted to develop standardised diagnostic tools for this rare finding.
Footnotes
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognised high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed and/or this work involved the use of cadavers. Ethical approval from a committee was therefore not specifically required for publication in JFMS Open Reports. Although not required, where ethical approval was still obtained, it is stated in the manuscript.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (experimental or non-experimental animals, including cadavers, tissues and samples) for all procedure(s) undertaken (prospective or retrospective studies). No animals or people are identifiable within this publication, and therefore additional informed consent for publication was not required.