
Abstract
Practical relevance:
Diseases of the hepatobiliary system are not uncommon in first-opinion practice. The anatomy of the feline hepatobiliary tract differs from that of dogs and may predispose cats to inflammatory hepatobiliary disease. Case management can be challenging, and the prognosis is variable and dependent on the underlying disease process.
Clinical challenges:
Biliary tract disease in the cat has non-specific clinical signs that overlap with those of diseases of other body systems. Diagnostic tests of the hepatobiliary system are widely available, but interpretation of results can be challenging. Deciding on medical or surgical management can also be challenging; for example, various degrees of cholestasis may be seen with different diseases and disease severities, and will influence the decision to manage the patient medically or surgically. Surgery is indicated in cases of bile peritonitis, severe cholestasis, focal neoplasia or disease that is refractory to medical management. Intensive perioperative and postoperative management, with 24 h hospitalisation facilities, is essential.
Audience:
This review article is written for the small animal general/primary care practitioner, with an emphasis on decision-making in the surgical management of feline hepatobiliary disease.
Evidence base:
Evidence available in the published literature is reviewed and presented, and the inherent limitations are discussed.
Keywords
Introduction
Biliary tract disease in the cat is not uncommon in first-opinion practice. Clinical signs are non-specific, differentiation of surgical cases from medical cases is not always straightforward and surgery itself is technically challenging. This review covers aspects that a practitioner needs to have a thorough understanding of when considering surgery of the feline hepatobiliary system: anatomy, function, pathophysiology, surgical techniques and perioperative management.
Anatomy and function of the feline biliary tract
The liver is responsible for a variety of homeostatic, synthetic and excretory functions, 1 including the production of bile, which is essential for normal digestion and absorption of nutrients. At the microscopic level, bile is produced in the hepatocytes and secreted into the bile canaliculi. 2 The canaliculi continue as the interlobular bile ducts before becoming the grossly visible hepatic ducts. These extrahepatic ducts are associated with the gallbladder and the duodenum via the cystic duct and the common bile duct, respectively (Figure 1). The common bile duct is visible ultrasonographically, and is typically a maximum of 4 mm in diameter. 4 The gallbladder is located within the hepatic fossa bordered by the right medial and quadrate lobes, 5 and acts as a bile store. The common bile duct enters the duodenum and courses intra-murally before emptying at the major duodenal papilla, about 3 cm aborad to the pylorus. In cats, the common bile duct and pancreatic duct fuse before emptying into the duodenum, unlike in the dog where the ducts remain distinct. 6 In 20% of cats, an accessory pancreatic duct empties into the minor duodenal papilla, approximately 2 cm aborad to the major duodenal papilla. 7 Anatomical variants of the normal unilobed gallbladder may be seen in cats; bilobed or duplex gallbladders have been reported.8,9
The gallbladder modifies and then secretes the stored bile via the cystic and common bile ducts - a process that is under neurohormonal control. 5 Bile acids aid in digestion and absorption before being mostly reabsorbed via the enterohepatic circulation. 4 Bile is also used to excrete organic solutes and other waste products. 2
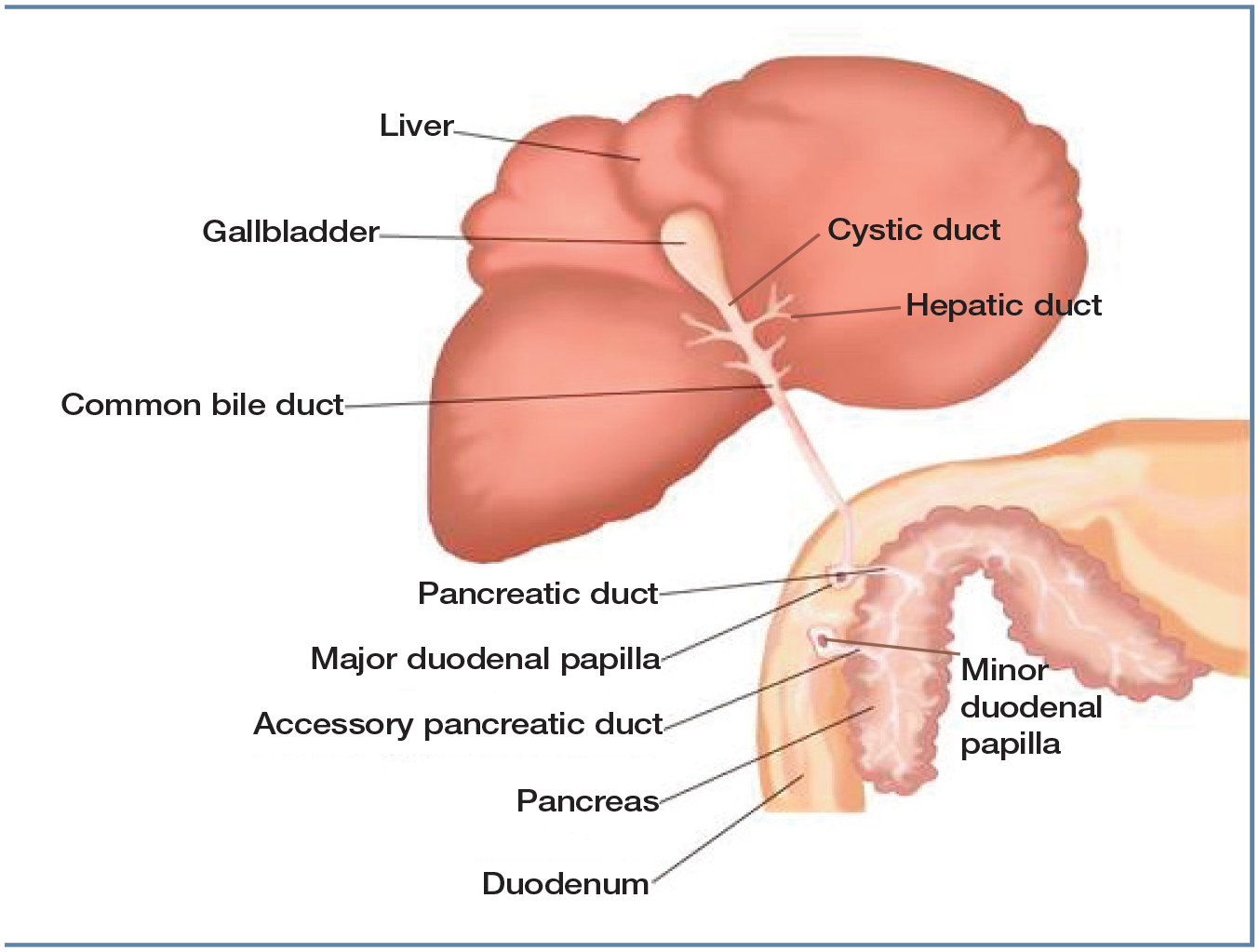
Illustration of gross hepatobiliary anatomy showing the gallbladder, hepatic ducts, common bile duct, pancreatic duct, and major and minor duodenal papillae.
Feline biliary tract disease
The biliary tract in the cat may be affected by various disease processes, and concurrent disease in other organs such as the pancreas, liver and gastrointestinal tract is not uncom-mon. 3 Cats are unlike dogs in that feline gallbladder mucoceles are rare. 2
Cholestasis - which is a reduction in or cessation of bile flow 10 - is an important feature of biliary tract disease in the cat. It is not a disease in itself but instead a consequence of abnormal biliary tract structure or function. 2 Cholestasis may arise within or outside the liver. Intrahepatic cholestasis occurs mainly at the level of the hepatocytes, bile canaliculi or bile ducts of the periportal zone, and may be associated with inflammation, fibrosis, endo-toxins or use of certain drugs. 10 Extrahepatic cholestasis occurs within the common bile duct (Figure 2), secondarily to gross obstruction (most commonly from choleliths), neo-plasia or inflammation of surrounding tissues. 11

Intraoperative view of a dilated common bile duct in a cat with extrahepatic biliary obstruction. The duct, indicated by the Metzenbaum scissors, is located between the right medial lobe (arrowhead) and left medial lobe (arrow) of the liver
Depending on their anatomical location, both cholelithiasis and neoplasia may result in varying degrees of cholestasis. Cholelithiasis is uncommon in the cat, 12 with most choleliths (Figure 3) made up of bili-rubin or its derivatives. 2 The aetiology of cholelithiasis is variable, and includes altered metabolism, dysmotility and bacterial infec-tion.13,14 Neoplasia of the hepatobiliary system may be cholangiocellular, hepatocellular, neuroendocrine or mesenchymal in origin, with cholangiocellular tumours being the most common.15,16 Hepatobiliary neoplasia is a diverse set of diseases, and tumours may be benign or malignant and primary or metastat-ic in nature. 17

(a) The cat pictured in Figure 2 was found to have a cholelith (arrow) within the common bile duct (arrowheads). (b) Cholelith (4 mm diameter) removed from the common bile duct
Inflammatory hepatobiliary tract disease is common in cats and can be classified into neutrophilic, lymphocytic and chronic forms. 18 Cholangitis is the preferred term (vs cholangiohepatitis) and better reflects the histopathological findings of significant biliary tract inflammation with minor to no hepatic inflammation. 19 Because the cat has a fused common bile duct and pancreatic duct, this may predispose to bacterial reflux and ascending infection. 3 Neutrophilic cholangitis, the most common entity among the inflammatory hepatopathies, 19 is thought to develop secondarily to bacterial infection. 20 Neutro-philic cholangitis may present concurrently with pancreatitis and inflammatory bowel disease, a syndrome known as triaditis. 3 Cholecystitis is recognised in association with neutrophilic cholangitis 21 and is thought to represent a different manifestation of a single disease entity. 2
In contrast to neutrophilic cholangitis, lymphocytic cholangitis has not conclusively been shown to have a bacterial aetiology 22 and is postulated instead to be a result of autoimmune inflammation. 19 In endemic regions, chronic cholangitis secondary to trematode infection is recognised as a separate entity, 23 with free-roaming cats that hunt being at greater risk of disease. 24
Leakage of bile from the gallbladder or extrahepatic biliary tract can be a sequela to blunt or penetrating trauma, or a consequence of extrahepatic biliary obstruction (EHBO). 25 In rare traumatic cases, rupture of the biliary tract can involve the gallbladder, cystic duct or common bile duct, and concurrent cholecystitis may be seen. 26 When this occurs, a sterile (chemical) peritonitis ensues. 25 Nontraumatic bile peritonitis, in contrast, may be associated with a concurrent focus of infection and a septic peritonitis. 27 , 28
Clinical presentation and diagnostic tests
Clinical signs of hepatobiliary disease are non-specific and may overlap with those of pancreatic, bowel or other organ system disease. 29 Vomiting, weight loss, lethargy and anorexia are common presenting signs; jaundice, cranial abdominal pain and pyrexia may be found on physical examination. 21 The clinical course of hepatobiliary tract disease is extremely variable and is dependent on the underlying condition; cats may be presented with chronic insidious disease or acute fulminant disease. 19

Routine haematology and serum biochemistry are useful for evaluating the severity of hepatobiliary disease and to rule out disease in other organ systems. Anaemia and leukocytosis may be seen in certain biliary tract diseases, although neither is specific for a particular diagnosis. 12 Analytes such as alanine aminotransferase, alkaline phosphatase, gamma-glutamyl transferase and bilirubin may be elevated on routine biochemistry in conjunction with elevations in serum bile acids. However, no combination of findings is highly sensitive or specific for biliary tract disease. 2 Further laboratory tests, such as feline pancreatic lipase immunoreactivity, urinalysis or faecal analysis, may be performed in conjunction with blood tests. The reader is referred to other sources for a more comprehensive discussion of laboratory evaluation of the hepatobiliary system. 30
Diagnostic imaging is essential in the cat with hepatobiliary disease to further localise the site of disease and to assess if EHBO is present. The choice of imaging modality will depend on the patient's clinical condition, stability for general anaesthesia, facilities available and operator experience. Plain I radiography may reveal choleliths (Figure 4), most of which are radiopaque, or large mass lesions; sensitivity for other conditions is poor. 33 Abdominal ultrasound provides detailed information regarding the structure of the hepatobiliary tract and can be particularly useful when visualising choleliths (Figure 5). As well as providing a live image of patient anatomy, ultrasonography may allow limited assessment of function. 34
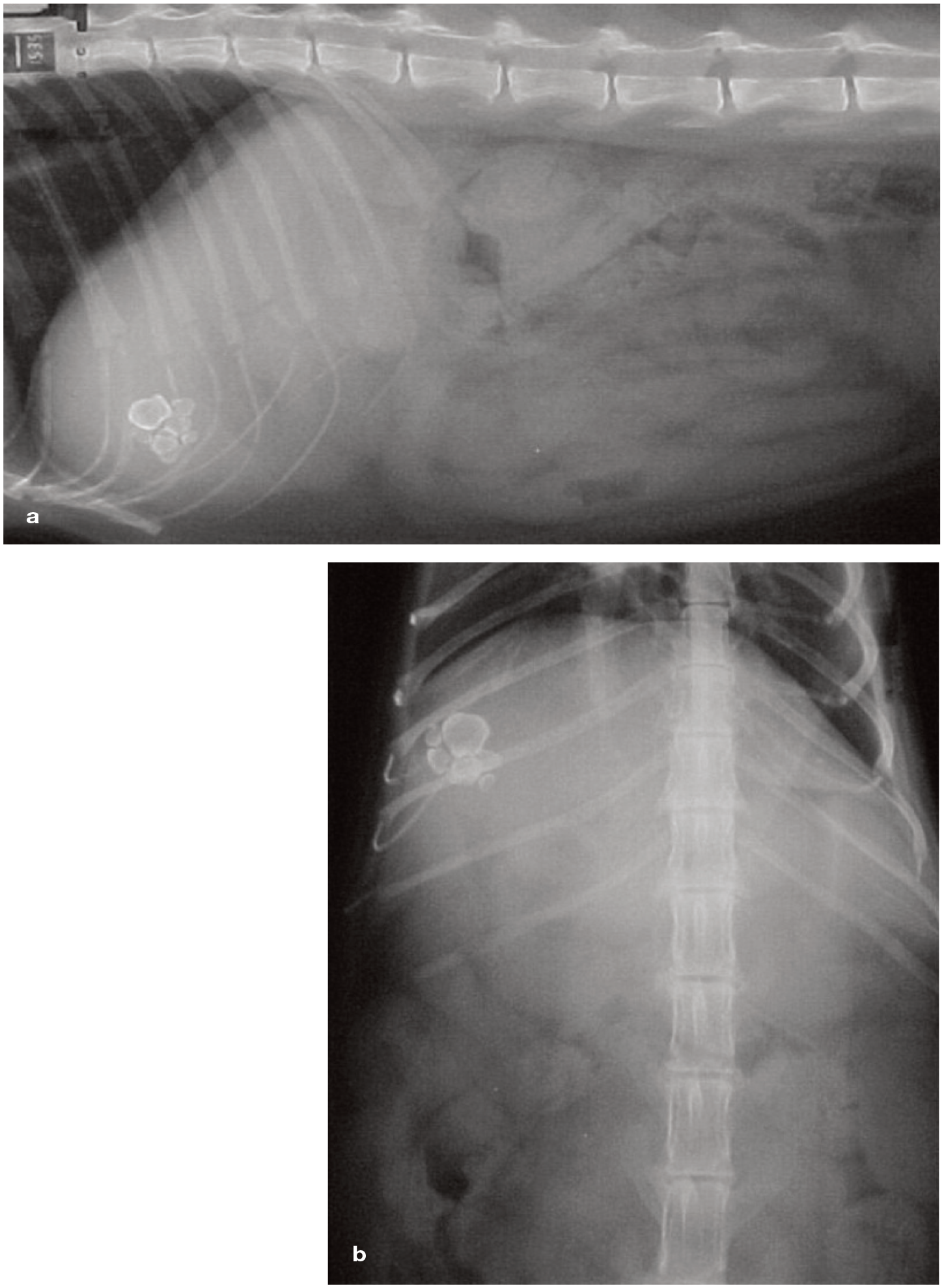
Lateral (a) and ventrodorsal (b) radiographs showing mineral-density choleliths in the right cranial abdomen. Reproduced from Elwoodetal (2001), 14 with permission from SAGE Publications
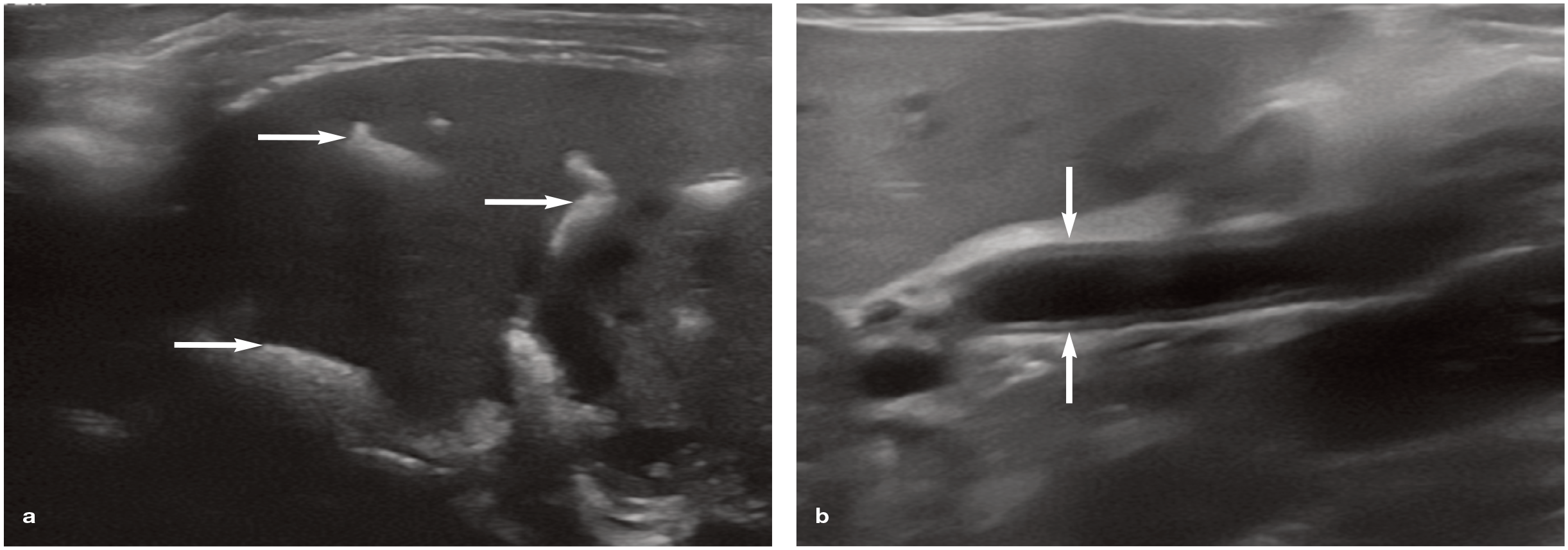
Ultrasonographic findings in two cats with hepatobiliary disease, (a) Multiple tortuous hyperechoic tracts (arrows), with associated distal acoustic shadowing, observed throughout the liver of a 16-year-old male neutered domestic shorthair cat with advanced renal failure; these findings are representative of extensive choledocholithiasis, (b) Dilation of the common bile duct (arrows) in a 14-year-old female neutered domestic shorthair cat with neutrophilic cholangitis.
Ultrasonography is highly sensitive in the work-up of biliary tract disease, but lacks specificity.35,36 As such, where lesions are revealed, further confirmatory tests such as cytology, histology or exploratory surgery will be required. 37 For example, abdomino-centesis and effusion analysis are necessary for the confirmation of bile peritonitis; an abdominal fluid bilirubin concentration twice that of the serum is diagnostic. 37 CT, with the use of intravenous contrast when appropriate, yields information complementary to that provided by an ultrasound examination. 33 Compared with ultrasonography, CT also has the advantages of being less operator-dependent and is less limited by the size or conformation of the patient. Other advanced techniques such as MRI, contrast-enhanced ultrasound, endoscopic retrograde cholangio-pancreatography and ultrasound elastogra-phy are useful, but not widely available.33,35
Decision-making in biliary tract disease
Once biliary tract disease has been diagnosed with laboratory tests and imaging, the practitioner should attempt to refine the diagnosis, establish if EHBO is present and, if so, its severity, and determine whether medical or surgical management is most appropriate.
EHBO may be partial or complete and is not an immediate indication for surgery. For example, the cholestasis observed in inflammatory hepatobiliary disease (ie, functional intrahepatic cholestatsis) is multifactorial, but cholestasis may also be associated with EHBO within the extrahepatic biliary system. 38 For inflammatory diseases of the biliary tract, medical management is the treatment of choice, unless there is severe and complete EHBO and/or the patient is refractory to medical management. Medical management is centred on use of analgesics, antiemetics, antibiotics, nutritional support and fluid therapy. 3
Choleliths may be associated with cholangi-tis or cholecystitis,
39
but may also be incidental findings.40,41 The clinical course of disease has been shown to be more acute in symptomatic feline cholelithiasis compared with inflammatory hepatobiliary disease or neo-plasia resulting in EHBO.
11
Hepatobiliary neoplasia may be focal, multifocal or diffuse, and may be suspected on the basis of patient signalment, clinical signs and imaging findings. 33 Histopathology is required for definitive diagnosis of the tumour type. The accuracy of fine-needle aspiration and needle core biopsies for this purpose is limited compared with wedge biopsies obtained either laparoscopically or via open surgery.43-45 Open surgery for diagnostic purposes within the hepatobiliary tract may be performed in conjunction with therapeutic surgical procedures, including those to relieve EHBO. 12 Further treatment will be dictated by tumour type, grade and stage. 46
Bile peritonitis is a consequence of rupture within the biliary tract and subsequent bile leakage into the abdominal cavity. 47 This is a surgical condition that requires open laparo-tomy, identification of the underlying cause and source of contamination, treatment of the source of biliary leakage and abdominal lavage. 48 Differentiation of a sterile from a septic bile peritonitis is important as the latter may require closed suction peritoneal drainage. 49
See box 'Surgical intervention: indications and timing' for further discussion, including decision-making around referral of patients for further surgical or medical care.
Perioperative management
Key components of perioperative management are the provision of appropriate analgesia, fluid therapy and perioperative antibiosis, as well as monitoring of the coagulation system.
Analgesia
Cats with biliary tract disease are likely to experience pain secondarily to the underlying condition. 21 An appropriate analgesic plan should be tailored to the patient, accounting for both existing pain and anticipated pain associated with the surgical procedure. 52 Opioids are recommended for perioperative pain management in the acute setting. 53 They may be combined with incisional or intraperitoneal local anaesthesia to provide multimodal analgesia. 54 Non-steroidal anti-inflammatory drugs are contraindicated when dehydration, hypotension, gastrointestinal disease or coagulopathies are present, and should be used with caution in the cat with hepatobiliary disease. 55 The reader is referred to other sources for more detailed discussion of perioperative analgesia. 52 Techniques that may be useful include epidural anaesthesia, peripheral nerve blocks (transverse abdominal plane block or quadratus lumborum block 56 ) and ketamine infusions. 52
Fluid therapy
Interstitial and intravascular volume deficits are likely to be present in the sick cat with hepatobiliary disease. 36 Fluid and electrolyte deficits should be corrected prior to anaesthesia and surgery; this may be performed alongside the initial diagnostic work-up. Intra -o perative hypotension without haemorrhage and postoperative acute kidney injury are common complications in cats undergoing biliary tract surgery. 57 The reader is referred to other sources for more detailed discussion of monitoring of blood pressure and peri-operative fluid therapy. 58
Antibiotics
Antibiotics are administered perioperatively depending on the planned surgical procedure and the presence of pre-existing contamination or infection.

Monitoring for coagulation disturbances
Coagulation disturbances in cats with hepato-biliary disease are variable and complex. 36 Hypercoagulable, normocoagulable and hypo-coagulable states may be seen on thrombo-elastography.63,64 In vitro haemostatic testing may show elevations in prothrombin time; 65 however, these tests may not reflect conditions in vivo. 64 Further treatment with paren-teral vitamin K or antifibrinolytic agents may be used at the practitioner's discretion.12,63
Surgical procedures
Surgical procedures of the biliary tract include choledochal catheterisation and stenting, chole-cystostomy tube placement, cholecystectomy, cholecystoenterostomy, choledochotomy, chole-cystotomy and treatment of bile peritonitis.
The biliary tract is generally approached via a midline coeliotomy with the patient positioned in dorsal recumbency. Full exploration of the abdomen should always be performed, regardless of the specific biliary tract procedure; whether this is conducted before or after the primary procedure depends on the preference of the surgeon. Other surgical procedures such as hepatic or pancreatic biopsy may be performed in conjunction with biliary tract surgery.
Choledochal catheterisation and stenting
Choledochal catheterisation (Figure 6) is a technique performed, usually in conjunction with and prior to other procedures, to confirm the patency of the common bile duct. 66 Normograde placement of a catheter via a cholecystotomy incision increases the risk of bile spillage and is not recommended. Retrograde placement via an antimesenteric duodenotomy and passage of a 3.5-5 French red rubber catheter is preferable. 66 Patency can then be confirmed with retrograde flushing, and any choleliths may be flushed into the gallbladder prior to cholecystectomy. Alternatively, a cholecystotomy may be performed prior to retrograde flushing, and choleliths directly visualised as they are flushed into the gallbladder.

Choledochal catheterisation in a cat performed via a duodenotomy
Choledochal stenting may be performed to restore normal flow of bile in cases of reversible EHBO. 67 Following choledochal catheterisa-tion, a 5-10 cm segment of catheter is left in situ with approximately half residing within the duodenal lumen in an aborad direction. The catheter is sutured into the duodenal submu-cosa with 1 or 1.5 metric absorbable monofila-ment suture material. 12 The stent restores biliary flow temporarily and subsequently is passed through the gastrointestinal tract. 68
Cholecystostomy tube placement
Cholecystostomy tube placement is an alternative to choledochal stenting to temporarily restore normal flow of bile. 36 The technique should only be performed in cats with a healthy gallbladder. 12
A stab incision is created in the gallbladder apex and a locking pigtail catheter is placed following drainage of bile from the gall-bladder. 66 Having secured the catheter to the gallbladder wall using a 1.5 or 2 metric purse-string suture, the catheter is passed through the body wall and secured externally. A closed collection system is attached to the catheter and maintained in place for 3-4 weeks. 69 If bile is being removed over a long period, consideration should be given to replacing this into the gastrointestinal tract, otherwise maldigestion and malabsorption may result.
Cholecystectomy
Cholecystectomy may be performed in cases of cholecystitis, cholelithiasis, gallbladder rupture or gallbladder neoplasia. 12 The gallbladder is identified and bluntly dissected away from the hepatic fossa before double ligation of the cystic duct and artery with nonabsorbable suture material or ligating clips. 66 The stump should be inspected for retrograde leakage of bile, and testing may be performed with retrograde flushing via a choledochal catheter. Performing a cholecystectomy precludes performing a cholecystoenterostomy in the future, should recurrent biliary obstruction occur, and this should be factored into decision-making and client counselling.
Cholecystoenterostomy
Cholecystoenterostomy is used to create a permanent biliary diversion in cases of irreversible EHBO. 70 A cholecystoduodenostomy is favoured over a cholecystojejunostomy, to preserve the normal physiological emptying of bile into the duodenum. 66
The gallbladder is dissected free from the hepatic fossa, as for cholecystectomy, and apposed against the intended site of anastomosis along the duodenum. Excessive tension on or twisting of the cystic duct and artery should be avoided. Matching incisions about 2.5-3 cm in length are created along the long axis of the gallbladder, and in the antimesen-teric wall of the duodenum. 12 If duodenotomy and choledochal catheterisation have been performed, the same duodenal incision may be used. Finally, the cut edges of the gallbladder and duodenum are apposed with 1.5 or 2 metric absorbable monofilament suture material in a simple continuous pattern.
The prognosis after cholecystoenterostomy depends on the underlying condition, and median survival times have been reported to be 14 days and 255 days with neoplasia and inflammatory disease, respectively. 70 Choledo-choduodenostomy has been reported in the cat as a salvage procedure, 71 but is not routinely recommended.
Choledochotomy
Choledochotomy may be used to remove choleliths causing intraluminal obstruction which cannot be removed with choledochal flushing. A longitudinal incision is made into the bile duct over the area of interest, and the obstruction removed before repair with either 1 or 1.5 metric absorbable monofilament suture material. Choledochotomy may be combined with choledochal stenting to buttress the repair. 12 Choledochotomy is only recommended as a last resort due to the risks of dehiscence, stenosis and iatrogenic biliary tract damage. 66
Cholecystotomy
Cholecystotomy may be performed to remove cholecystoliths and spare the gallbladder. 39 However, a cholecystectomy is favoured over this procedure as most choleliths form within the gallbladder; therefore, cholecystectomy is curative. 66 The gallbladder is isolated from the abdomen with laparotomy swabs and an incision is made in its apex. Bile and choleliths within the gallbladder are removed and the gallbladder lavaged. Cholecystotomy may be combined with choledochal catheterisation to verify the patency of the common bile duct. The cholecystotomy incision is repaired with 1 or 1.5 metric absorbable monofilament suture. 66
Treatment of bile peritonitis
Bile peritonitis (sterile or septic) is approached in a similar fashion to the treatment of other forms of peritonitis. Surgery is directed at identifying the source of bile leakage and removal of abdominal contamination, combined with other procedures of the biliary tract to repair the source of leakage.



Oesophagostomy feeding tube in a cat
Prognosis
The patient's prognosis depends on the underlying disease process. Cats with hepato-biliary disease requiring biliary tract surgery generally have a poor to guarded progno-sis.12,36 EHBO associated with neoplasia carries a worse prognosis than that associated with inflammatory hepatobiliary disease, 78 with one study reporting a median survival time of 14 days after surgery. 70 The anaesthetic and postoperative complication rate in cats undergoing cholecystoenterostomy is high, and thus the prognosis is guarded, regardless of the underlying cause. 36 Choledochal stent-ing may offer cats a better prognosis than cholecystoenterostomy, although the strength of evidence is low.36,68 Cholecystectomy is well tolerated and, provided neoplasia is not involved, cats undergoing this surgery have a good long-term prognosis.8,79
Conclusions
Feline biliary tract disease can represent a diagnostic and treatment challenge. Clinical signs and clinical pathology overlap with diseases of other body systems. Diagnostic imaging is useful to localise disease to the biliary tract and guide further tests or treatment. Strong evidence to support the optimal timing of surgery and surgical procedure of choice is lacking. Referral of these patients for further medical or surgical care is appropriate, where possible.
Key Points
✜ The anatomy of the feline and canine hepatobiliary tracts differs. Cats may be predisposed to inflammatory hepatobiliary disease.
✜ Clinical signs and diagnostic test results are nonspecific and should be interpreted in the context of the individual patient and alongside other findings.
✜ Cholestasis is a syndrome and not a specific disease.
✜ Treatment of hepatobiliary disease is directed at the underlying cause.
✜ Surgery is indicated in cases of bile peritonitis, severe cholestasis, focal neoplasia or when the disease is refractory to medical management. Specialist referral should be considered.
✜ The prognosis is variable, dependent on the underlying disease process.
Footnotes
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This work did not involve the use of animals and therefore ethical approval was not specifically required for publication in JFMS.
Informed consent
This work did not involve the use of animals (including cadavers) and therefore informed consent was not required. No animals or people are identifiable within this publication, and therefore additional informed consent for publication was not required.