
Abstract
Case summary
A 7-year-old spayed female domestic shorthair cat was presented for evaluation of a 4-month history of slowly progressive back pain. Neurological and orthopaedic examinations revealed a low posture of the hindlimbs, reluctance to walk, a wide stance, hind limb ataxia and significant pain at the caudal spine, including the base of the tail. MRI of the brain and spinal cord demonstrated marked segmental dilation of the central canal with diffuse ependymal and parenchymal contrast enhancement, affecting almost the entire spinal cord. Widening of the intracranial ventricular system with a secondary mass effect on the surrounding cerebral parenchyma resulted in a reduction of cerebral cortex thickness as well as of the subarachnoid space, flattening of the cerebellum and a decreased size of the interthalamic adhesion. Histopathological examination of the brain and spinal cord revealed perivascular and parenchymal aggregates of mononuclear cells containing occasional atypical large lymphocytes, often infiltrating into blood vessels and the central canal, and affecting both white and grey matter. The most severe changes were found at the lumbosacral segment, with markedly distorted parenchyma and central canal, and the presence of neuronal and axonal degeneration and loss. Immunohistochemistry showed atypical large mononuclear cells positive to Pax5 (neoplastic B cells) and abundant small round cells positive to CD3 (reactive T cells), confirming the diagnosis of central nervous system T-cell-rich B-cell lymphoma with an angiocentric and angioinvasive distribution pattern.
Relevance and novel information
This article describes imaging characteristics of a rare case of histopathologically confirmed central nervous system T-cell-rich B-cell lymphoma.
Introduction
Lymphoma is the most common spinal neoplasm and the second most common intracranial tumour in cats.1 –3 MRI features of feline spinal cord lymphoma include focal or multifocal lumbar/lumbosacral epidural lesions characterised by ill-defined margins, hyperintensity on T2-weighted (T2W) images, isointensity on T1-weighted (T1W) images and variable post-contrast enhancement. Lesions commonly extend into adjacent bone and paraspinal musculature; however, none of these MRI characteristics are pathognomonic.4,5
Primary nervous system lymphoma is uncommon in cats, predominantly affecting the spinal cord and epidural space, typically with multi-organ involvement. 6 T-cell-rich B-cell lymphoma (TCRBCL) is a rare subtype of large B-cell lymphoma, most commonly affecting cervical lymph nodes, 7 where atypical large B cells are surrounded by extensive populations of reactive T cells. In this report, we present MRI and histopathology findings of an uncommon case of feline primary central nervous system (CNS) TCRBCL with an angiocentric and angioinvasive pattern affecting the cerebrum, cerebellum, brainstem and spinal cord.
Case description
A 7-year-old spayed female domestic shorthair cat was presented with slowly progressive back pain of 4 months’ duration, reluctance to jump, a wide-based stance of the hindlimbs and vocalisation in the litter box. There was no known history of trauma. Radiographs of the spine and pelvis were unremarkable. Before referral, the primary veterinarian initiated multimodal analgesic therapy consisting of meloxicam (0.05 mg/kg PO q24h, Novacam; Dechra) and gabapentin (10 mg/kg PO q8h), given both intermittently and in combination. After approximately 2 months without clinical improvement, frunevetmab (1.7 mg/kg SC q28 days, Solensia; Zoetis) was added to the regimen. Despite these trials, the patient’s condition continued to progress.
On physical examination, the cat was bright, alert, responsive and in good body condition (body condition score 4/9). The cat exhibited a low body posture, particularly in the hindlimbs and tail base, reluctance to walk, a wide-based stance and hindlimb ataxia. Neurological examination revealed normal mentation and cranial nerve function. Conscious proprioception was absent in the hindlimbs, and significant pain was elicited upon lifting the tail and palpating the lumbar and sacral spine. The remainder of the neurological and orthopaedic examination was unremarkable, and neurolocalisation was suspected to involve the T3–L3 spinal segment. Although the underlying cause was initially unclear, vertebral canal stenosis and chronic intervertebral disc disease were considered the most likely differential diagnoses at that time. MRI was selected as the diagnostic modality of choice and recommended to be performed on the same day.
Head, thoracic and lumbosacral spine MRI was performed under general anaesthesia following the standard institutional protocol for feline patients (dexmedetomidine 6 µg/kg and butorphanol 0.2 mg/kg as premedication, propofol 2.4 mg/kg for induction). The patient was in dorsal recumbency in a 1.5 T MRI (Ingenia; Philips Healthcare) using head and body coils. The following sequences were obtained: sagittal T1W, T2W, three-dimensional T2W single shot echo (3D myelogram), transverse T1W and T2W, dorsal short tau inversion recovery (STIR) and intravenous contrast administration (gadoterate meglumine 0.2 ml/kg), transverse T1W, sagittal T1W and spectral presaturation with inversion recovery T1W.
MRI scans (Figures 1 and 2) revealed multifocal marked segmental cystic widening of the spinal central canal with T1W hypointensity and T2W/STIR hyperintensity with mild to moderate contrast enhancement of the lining of the central canal and cord surrounding the central canal. The changes were most severe at the caudal lumbar spine and the sacrum; secondary moderate to marked spinal cord parenchymal deformation and compression were present, most pronounced at the cyst-like widenings of the central canal. Heterogeneous, ill-defined T2W hyperintensity of the entire visible spinal cord surrounding the central canal could be noted, and the surrounding epidural fat and cerebrospinal fluid (CSF) signal of the subarachnoid space were lost. The paraspinal bones, soft tissues and included abdominal lymph nodes were unremarkable.

(a,c) Transverse mid-L5 body (dotted white line) and (b,d) mid-sagittal T1-weighted (T1W) and T2-weighted (T2W) MRI scans of the lumbosacral spinal cord. T1W hypointense and T2W hyperintense multifocal and segmental widening of the central canal, extending throughout the spinal cord. Variable degree of spinal cord compression by the cyst-like widening of the central canal

(a) Mid-sagittal T1-weighted (T1W) and (b) T1W spectral presaturation with inversion recovery post-gadolinium MRI scans of the lumbosacral spinal cord. Intramedullary contrast enhancement around (peripheral to) the mentioned segmental cystic widening of the central canal
MRI of the brain (Figure 3) revealed marked asymmetric widening of the ventricular system with secondary leftward midline shift, dorsal flattening of the cerebellum, decrease in interthalamic adhesion size and marked cerebral cortex thinning. There was no evident contrast enhancement of the cerebrum and cerebellum, as well as the pons, meninges or ependymal lining of the ventricular system.

(a) Transverse T2-weighted (T2W), (b) T1-weighted (T1W) and (c) T1W post-gadolinium imaging of the brain at the level of the third ventricle (the right side is the left side of the images). Marked asymmetric dilation of the lateral (right > left), third and mesencephalic aqueduct and significant thinning of the cerebral cortex
It was concluded that there was marked generalised dilation of the ventricular system (hydrocephalus and hydromyelia) with multifocal contrast enhancement of the spinal cord and central canal ependyma. Meningoencephalomyelitis with ependymitis of infectious origin, such as feline infectious peritonitis (FIP), was considered most likely, while parasitic (eg, toxoplasmosis) or bacterial causes were less likely. Round cell neoplasia (eg, lymphoma) was deemed unlikely at that time.
Given the high probability of FIP, together with an uncertain but likely poor prognosis, the lack of legally available disease-modifying treatment options and ongoing chronic pain despite analgesia, the cat was subsequently euthanased. The owner consented to a post-mortem examination.
Pathological and histopathological findings
Post-mortem examination
Macroscopically, the L4–L7 spinal cord was mildly thickened, and adjacent nerves appeared pale yellow, wet and shiny. No other gross CNS lesions were seen. Elsewhere, only scattered 0.2 cm white pancreatic nodules (presumed chronic pancreatitis/nodular hyperplasia) and diffusely light brown, slightly irregular tibial-plateau cartilage in both stifles (osteoarthritis) were noted.
Histopathological findings
Histological examination with haematoxylin and eosin stain was performed on the brain, spinal cord, peripheral nerves, heart, lung, liver, spleen, kidney, pancreas, thyroid and adrenal glands, thymus and muscle, plus L6 and L7 vertebrae and intervertebral disc after previous decalcification with formic acid. Throughout several cuts from the cervical, thoracic, lumbar and, more prominently, sacral spinal cord, frequent intraparenchymal and perivascular aggregates of mononuclear cells were noted. The mononuclear cell population was observed distending the Virchow–Robin space of many parenchymal blood vessels within the grey and white matter, multifocally infiltrating into the vessel walls and lumina, and often within the central canal lumen. The canal was markedly dilated and distorted, mainly at thoracolumbar and sacral levels, with multifocal areas with slightly swollen ependymal lining (reactive) and infiltrating mononuclear cell aggregates (Figures 4 and 5).

Transverse cuts of (a) cervical (× 20), (b) thoracic (× 10) and (c) lumbar spinal cord (× 20) showing multifocal aggregates of mononuclear cell populations surrounding parenchymal vessels, affecting both grey and white matter and often infiltrating into the dilated central canal. Variable numbers of small round lymphocytes are present, randomly distributed throughout the neuropil. Haematoxylin and eosin stain
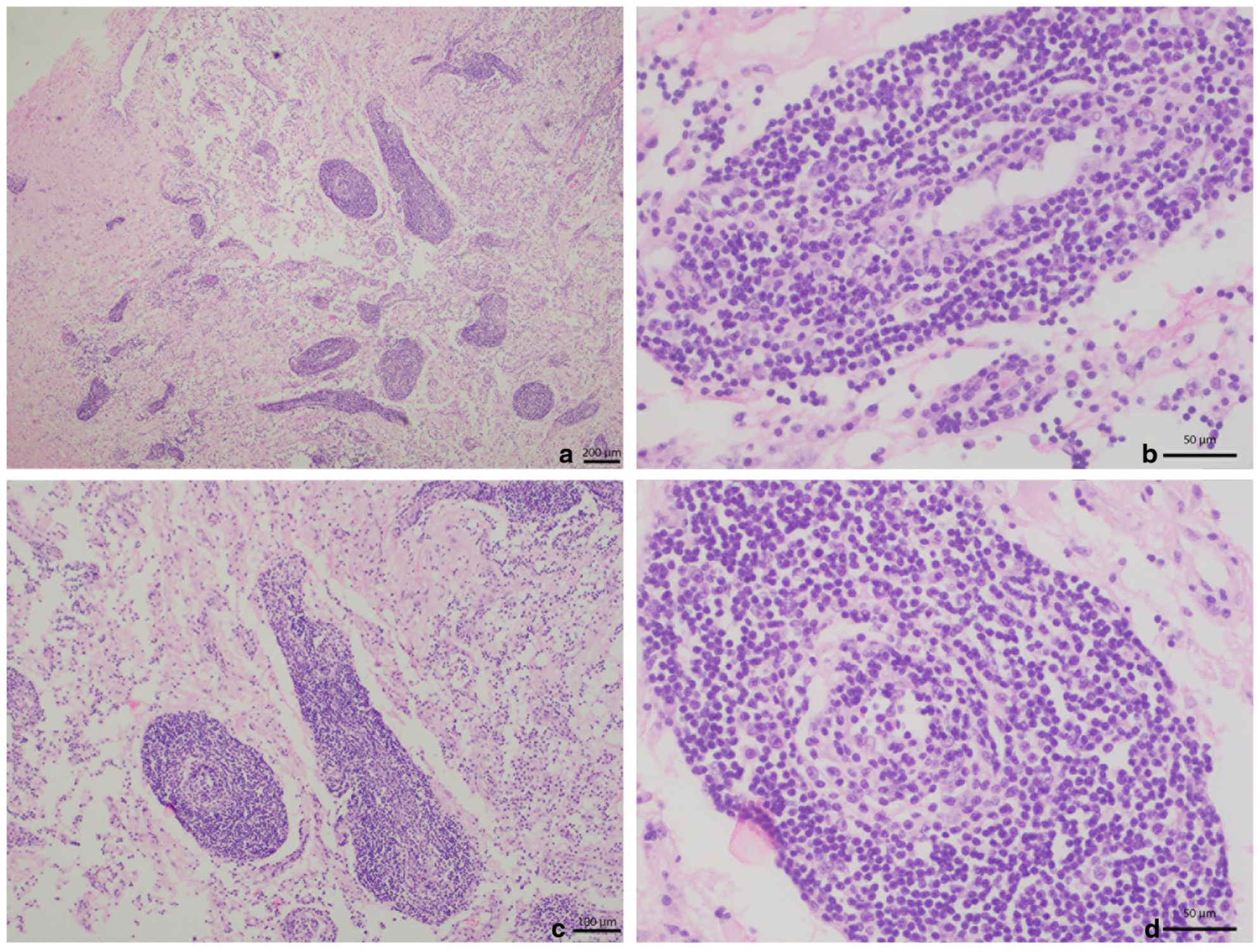
Transverse cut of the sacral spinal cord with many perivascular aggregates of the mononuclear cell population that distort and fragment the spinal parenchyma and central canal, affecting both (a) grey (× 4) and (c) white matter (× 10). (b,d) At × 40 magnification, scattered atypical large and irregular lymphocytes are seen surrounded by a majority of small T lymphocytes and variable numbers of typical B lymphocytes, infiltrating into the vessel walls and lumina. Endothelial cells appear plump, with swollen and clear nuclei protruding into the lumen (reactive). Haematoxylin and eosin stain
The cell population consisted of many small, well-differentiated T lymphocytes, variable numbers of small, well-differentiated B lymphocytes, and scattered atypically large and bizarre B cells up to 35 µm in diameter, with a round to polygonal shape and poorly distinct borders, scant to moderate amount of pale eosinophilic to amphophilic and finely vacuolated cytoplasm (the cytoplasm:nucleus ratio was 1:2), and a paracentric or eccentric round to oval nucleus, often vacuolated and with finely stippled chromatin, with up to two round nucleoli. Anisocytosis and anisokaryosis among the atypical B-cell population were moderate, and the mitotic count was very low (<1 mitosis per 2.37 mm²).
The sacral spinal cord also showed marked compression and distortion of the adjacent parenchyma in both white and grey matter, as well as several distended axonal sheaths, occasionally containing swollen and hypereosinophilic axons (spheroids), suggestive of axonal degeneration. Some neurons exhibited dispersion of Nissl substance towards the periphery of the cytoplasm and had clear, slightly vacuolated nuclei (chromatolysis, neuronal degeneration).
Similar cell populations were also found surrounding parenchymal blood vessels through the submeningeal areas of the cerebrum, cerebellum and brainstem, and multifocally markedly expanding the choroid plexus (Figure 6).
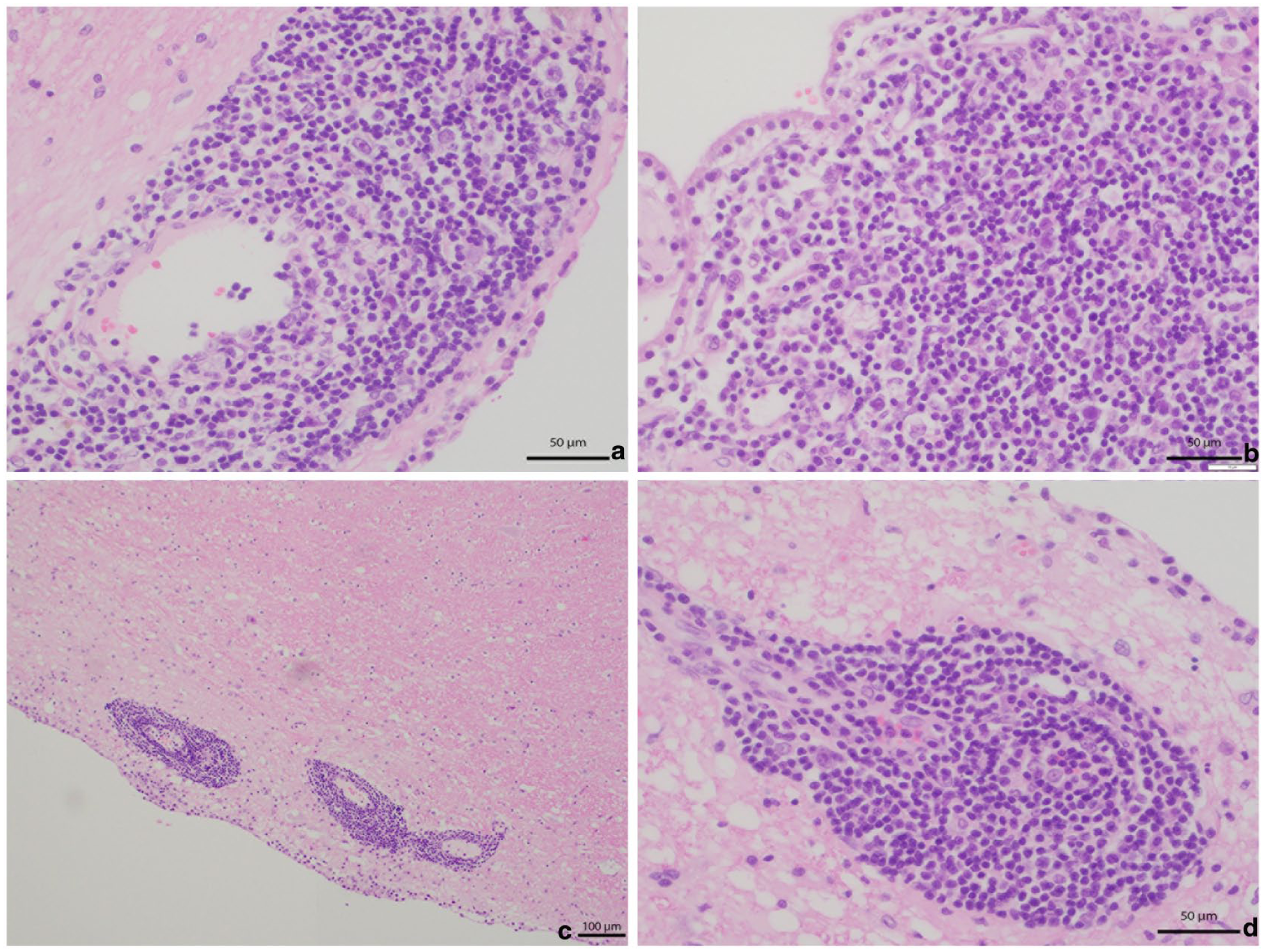
Transverse cuts showing the submeningeal regions of (a) the cerebrum (× 40), (b) choroid plexus (× 40), submeningeal areas of (c) the cerebellum (× 10) and (d) brainstem (× 40), showing similar perivascular and infiltrative mononuclear cell populations with scattered atypical large cells. Haematoxylin and eosin stain
No similar histological changes were found in the tissue analysed from the rest of the organs, including peripheral nerves, although signs of intervertebral disc degeneration were found in the L6–L7 intervertebral disc, as well as an incidental finding of nodular hyperplasia in the pancreas.
Antiserum against the T-lymphocyte marker CD3 and the B-lymphocyte marker Pax5 was used for the immunocharacterisation of the cell population in the sacral spinal cord. Up to 60% of the small mononuclear cell population was labelled by anti-CD3 antibody (consistent with reactive T lymphocytes), while the rest of the population, including the atypical large cells, were labelled by anti-Pax5 antibody (consistent with both neoplastic and reactive B lymphocytes) (Figure 7).

Transverse cut of sacral spinal cord immunolabelled with (a,b) anti-CD3 antibody at ×4 and ×40, respectively, and (c,d) anti-Pax5 antibody at ×4 and ×40, respectively. Up to 60% of the mononuclear population consists of small round T lymphocytes with uniform cytoplasmic labelling against CD3, also observed diffusely in small numbers throughout the entire spinal cord parenchyma. The remaining cells within and around the previously mentioned foci, including the atypical large cells, present uniform nuclear labelling against the Pax5 marker. Haematoxylin and eosin stain
Discussion
TCRBCL has previously been reported in cats,6 –10 with only three cases described affecting the brain or spinal cord, specifically affecting the frontal and parietal lobes and cervical and L6–L7 spinal regions. 6 To our knowledge, this is the first case report that describes the MRI findings in a cat with histopathologically confirmed TCRBCL, with simultaneous spinal cord and brain involvement and secondary alteration of CSF flow.
Spinal cord lymphoma is the most common neoplasm affecting the feline spinal cord and the second most common intracranial tumour in cats,2 –4 typically affecting younger individuals with a short clinical course.2,11,12 The tumour commonly presents in an extradural or combined extradural-intradural location, while exclusive intradural or intramedullary presentations are rare.2,4,12 Both T-cell and B-cell phenotypes have been associated with spinal infiltration, and survival times range from 1 week to 13 months, with a mean survival of 4.5 months.5,6
In previous studies, MRI findings of feline spinal lymphoma have shown lesions primarily in the thoracolumbar and lumbosacral regions, involving both extradural and intradural (including intramedullary) compartments and frequently (>50%) affecting the associated spinal nerves. These lesions are generally ill-defined, hypointense to isointense on T1W images, hyperintense on T2W images and exhibit heterogeneous hyperintensity on STIR sequences, often with homogeneous and strong contrast enhancement. Vertebral and paraspinal muscle lesions are common,4,5,13,14 as well as brachial plexus involvement, with mass-like formations extending into the subarachnoid space and spinal cord parenchyma proximally.12,15
Differential diagnosis can be challenging, as the MRI characteristics of spinal lymphoma may overlap with those of other neoplastic conditions (eg, histiocytic sarcoma, oligodendroglioma), as well as inflammatory and infectious conditions, such as meningomyelitis caused by FIP or toxoplasmosis.
This report describes a rare case of TCRBCL lymphoma with MRI evidence of marked hydrocephalus, ependymal and intramedullary contrast enhancement, and segmental cystic dilation of the central canal in the thoracolumbar and lumbosacral spine. These MRI abnormalities are not unique to this tumour type but reflect extensive infiltrative and obstructive CNS disease. Few studies have documented primary CNS lymphoma in cats, with TCRBCL previously described either in the brain or the spinal cord; therefore, to our knowledge, this is the first primary nervous TCRBCL reported to affect both regions simultaneously. The unusual hydrocephalus and central canal dilation may result from increased CSF production due to choroid plexus infiltration and/or disrupted CSF flow and drainage.14,16 –18
TCRBCL is a subtype of large B-cell lymphoma characterised by the presence of large atypical B cells surrounded by a majority of small reactive T cells, and it is one of the less common large B-cell lymphomas in dogs and cats, according to recent studies.6,19,20 Furthermore, in cats, it is often associated with a multicentric presentation with involvement of cervical or submandibular lymph nodes. 8
This case emphasises the diagnostic challenges encountered when relying solely on imaging to diagnose spinal cord lymphoma in cats. The prolonged 4-month clinical course, together with non-specific signs and ambiguous MRI findings, highlights the importance of integrating additional diagnostic modalities, such as CSF analysis, cytology, histopathology and immunohistochemistry, to achieve a definitive diagnosis. A further limitation was the absence of pre-imaging laboratory or serological testing, as the cat was referred after several months of orthopaedic management, and the chronic localised presentation did not initially raise suspicion for infectious or systemic disease. Consequently, advanced imaging was pursued directly, reflecting the clinical referral pathway rather than a deviation from best-practice principles.
Conclusions
This case report describes the MRI findings of histopathologically confirmed primary CNS TCRBCL in a 7-year-old domestic shorthair cat. The imaging changes are not specific for TCRBCL; however, they are noteworthy for the combination of segmental cystic dilation of the central canal within the thoracolumbar and lumbosacral spine, marked ependymal and intramedullary contrast enhancement, and concurrent hydrocephalus with atypical central canal dilation, most likely secondary to altered CSF flow. Histopathologically, the lesion showed typical features of TCRBCL, consisting of atypical large B cells intermixed with abundant small reactive T cells. Although primary CNS involvement with TCRBCL is rarely reported in cats, this case, to the authors’ knowledge, represents the first documented example with simultaneous spinal cord and brain involvement, highlighting an unusual pattern of diffuse CNS infiltration rather than defining MRI features that are unique to TCRBCL.
Footnotes
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognised high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed, and/or this work involved the use of cadavers. Ethical approval from a committee was therefore not specifically required for publication in JFMS Open Reports. Although not required, where ethical approval was still obtained, it is stated in the manuscript.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (experimental or non-experimental animals, including cadavers, tissues and samples) for all procedure(s) undertaken (prospective or retrospective studies). No animals or people are identifiable within this publication, and therefore, additional informed consent for publication was not required.