
Abstract
Case summary
Lymphoma is a prevalent malignancy in cats, commonly involving lymphatic or gastrointestinal tissues; however, primary muscular lymphoma is an exceedingly rare condition in veterinary medicine. This report describes a 7-year-old spayed female domestic shorthair cat that was presented for a 3-day history of progressive change in iris colour in the right eye. After rapid deterioration, the affected eye was enucleated and the cat was diagnosed with large T-cell lymphoma based on ocular histopathology and immunohistochemistry. The initial clinical signs were ocular; however, subsequent diagnostic evaluation revealed muscular involvement. Lymphoma was suspected to have originated in the quadriceps femoris muscle and subsequently metastasised to the eye.
Relevance and novel information
This case underscores the diagnostic complexity of lymphoma and highlights the importance of considering systemic disease in cases of unexplained uveitis. It was not possible to determine whether the muscle or the eye was the primary site; clinical signs were first ocular, but this does not confirm the eye as the origin. The association between primary muscular lymphoma and ocular presentation has not been previously reported. Early detection of lymphoma can improve clinical management, but diagnostic challenges often arise because of atypical presentations and the absence of detectable masses.
Introduction
Lymphoma is a common neoplasm of the feline haematopoietic system.1 –4 Ocular lymphoma, particularly uveal involvement, represents the most prevalent form of intraocular neoplasia in cats and often indicates systemic disease,5 –7 although frequently ocular signs appear before the identification of systemic involvement.8 –10 Occasionally, intraocular lymphoma can present as a presumed solitary ocular lymphoma (PSOL), without evidence of systemic involvement at the time of diagnosis. 11
Primary muscular lymphoma is extremely uncommon, with fewer than 10 cases reported in companion animals. 12 It poses significant diagnostic challenges because of its atypical location and potential overlap with other musculoskeletal or systemic conditions.
This case report describes a presumed primary muscular lymphoma where ocular signs were the exclusive clinical manifestation. This rare case highlights the importance of a comprehensive diagnostic approach in uveitis cases, particularly when routine work-up fails to identify a primary cause. The report also highlights the challenges of diagnosing lymphoma in its early stages, before progression to the lymph nodes or spleen.12 –14
Case description
A 7-year-old spayed female, indoor/outdoor domestic shorthair cat (weight 4.5 kg) presented to the ophthalmology service of the Hebrew University of Jerusalem’s Veterinary Teaching Hospital with a 3-day history of progressive iris colour change in the right eye (oculus dexter [OD]) and anorexia. The cat had a history of anaemia caused by Mycoplasma haemofelis 3 years prior, and fever of unknown origin 2 years before presentation, both of which were treated successfully with doxycycline. Upon presentation, the cat was otherwise healthy and up to date on vaccinations and flea control.
On examination, the cat exhibited moderate blepharospasm in OD with mild buphthalmos, seromucoid discharge, moderate diffuse corneal oedema, Florida spot keratopathy, 15 moderate conjunctival and episcleral hyperemia, 3+ aqueous flare with fibrin, hypopyon and a blood clot in the anterior chamber, congested and swollen iris, and a miotic pupil that prevented visualisation of the posterior segment (Figure 1). Examination of the left eye (oculus sinister [OS]) was overall unremarkable except for two small Florida spots. 15 The right pupil was smaller than the left; the direct pupillary light reflex (PLR) in the OS and consensual PLR from the OD to OS were intact, whereas the direct PLR in the OD and consensual PLR from the OS to OD were difficult to assess because of significant changes in the anterior segment of the right eye. Menace response was intact in the OS but sluggish and inconsistent in the OD, while dazzle and palpebral reflexes were intact in both eyes. Physical examination was unremarkable and vital signs were within normal limits.

Clinical image at initial presentation of the right eye of a 7-year-old domestic shorthair cat diagnosed with large-cell lymphoma. The main ophthalmic findings included moderate diffuse corneal oedema, Florida spot keratopathy (black arrowheads), moderate conjunctival and episcleral hyperaemia, 3+ aqueous flare with fibrin, hypopyon and a blood clot in the anterior chamber, congested and swollen iris, and miotic pupil
Both corneas were fluorescein negative. Intraocular pressure (IOP) was 20 mmHg in the OS and 90 mmHg in the OD. Ocular ultrasound of the OD showed a large echogenic ‘mass’ (Figure 2) posterior to the iris and cil-iary body, with no noticeable changes in the vitreous chamber nor evidence of retinal detachment. Aqueous paracentesis was performed to reduce the elevated IOP and collect an aqueous sample for cytology, followed by intracameral injection of tissue plasminogen activator (25 µg) and dexamethasone (1 mg). Cytological analysis of the aqueous humour revealed a neutrophil-dominant inflammatory response, but no neoplastic cells were identified.

Ultrasound images of (a) the right eye, showing an enlarged, echogenic mass (white asterisk) extending from the iris to the posterior lens capsule, (b) the right quadriceps muscle, which is thickened and hyperechoic with surrounding oedema and poorly defined muscle fascia, and (c) the right popliteal lymph node, which appears normal in size and shape but is surrounded by a small amount of free fluid (white arrowhead). Note the extension of oedema into the caudal thigh muscles (white asterisk)
Haematological and biochemical parameters were within reference intervals (RIs), while feline immunodeficiency virus (FIV)/feline leukaemia virus SNAP test was positive for FIV and feline serum amyloid A test was elevated (32 mg/dl, RI 0–6). The cat was discharged with topical prednisolone acetate 1%, brinzolamide 1% and atropine 1% (all twice daily OD), systemic antibiotics (amoxicillin-clavulanic acid, 12.5 mg/kg PO q12h) and an analgesic drug (dypirone, 25 mg/kg q24h).
Five days later, the cat returned for re-examination. The OD blepharospasm had improved but conjunctival hyperaemia and corneal oedema persisted, a superficial ulcer had developed in the central cornea, several keratic precipitates were noted on the ventral corneal endothelium and the pupil was mydriatic from atropine. OD aqueous flare decreased to 2+ and the IOP decreased to 15 mmHg. Topical therapy was changed to tropicamide 0.5%, oxytetracycline ointment 0.5%, penciclovir 1% cream16,17 because of presumed herpetic corneal ulceration (all q12h) and systemic oral prednisolone (1 mg/kg q24h).
On day 15, the cat presented again with an acute episode of right hindlimb lameness. Examination of the leg was overall unremarkable, while ophthalmic examination of the OD revealed worsening blepharospasm, blindness (absent menace, dazzle, PLRs), dyscoria and further thickening of the iris (Figure 3). Enucleation of the right eye, recommended for therapeutic and diagnostic purposes, was scheduled for the following week (day 21). On pre-anaesthetic evaluation, IOP was elevated in the OD (34 mmHg), uveitis with rubeosis iridis were observed in the OS (Figure 4) and the right hindlimb was moderately swollen, mainly cranial to the femur (eg, quadriceps femoris).

Clinical image of the right eye on day 15, showing a dyscoric dilated pupil, thickened and hyperaemic iris, and resorbing fibrin/blood clot in the anterior chamber

External photography of the feline patient on day 21 before enucleation of the right eye. Note the rubeosis iridis in the left eye (white arrowhead)
After standard subconjunctival enucleation of the OD, an extended diagnostic work-up was performed by an internal medicine specialist. A complete blood count and biochemistry panel revealed mild anaemia, with a haematocrit of 20.7% (RI 27–32.8), and lymphopenia (RI 2–7.2 ×10³/µl). Muscle enzymes, including creatine phosphokinase at 8759 IU/l (RI 73–260) and aspartate transaminase at 286 IU/l (RI 17–58) were significantly elevated. Additional abnormal findings included hypertriglyceridemia (373 mg/dl, RI 8–80), hypocholesterolaemia (81 mg/dl, RI 89–258), hypoproteinaemia (5.85 g/dl, RI 6.6–8.4) and low creatinine levels (0.72 mg/dl, RI 1.1–1.6). All other parameters, including lipase levels, were within normal limits. Urinalysis revealed elevated levels of protein, white and red blood cells, and urobilinogen.
As feline uveitis can be regarded as an intraocular lymphadenopathy, 18 fine-needle aspirate (FNA) samples were obtained from the right mandibular and right popliteal lymph nodes (ie, the same side as the ocular involvement). Cytological analysis of the mandibular lymph node revealed mild lymphoid reactivity, while the popliteal lymph node aspirate was consistent with adipose tissue and therefore a non-diagnostic sample. Three-view thoracic radiographs were unremarkable. Ultrasound of the swollen right hindlimb demonstrated a thickened and hyperechoic quadriceps femoris muscle surrounded by moderate oedema (Figure 2). FNA samples from the muscle were obtained, and cytological evaluation was consistent with large cell, high-grade lymphoma. Abdominal ultrasound revealed enlargement of the spleen and pancreas, although cytological evaluation of the spleen showed no evidence of malignancy.
The cat remained hospitalised for 4 days, during which intravenous fluids (lactated Ringer’s solution 2.6 ml/kg/h), systemic corticosteroids (prednisolone 2 mg/kg), antibiotics (amoxicillin-clavulanic acid 15 mg/kg), antiemetics (maropitant 1 mg/kg, metoclopramide 1 mg/kg/day) and L-asparaginase (400 U/kg) were administered. Despite initial improvements in the ocular signs of the OS, the cat developed a fever before discharge on day 24. The cat was discharged on day 25 with topical prednisolone acetate 1% and tropicamide 0.5% three times daily in the OS, systemic antibiotics (amoxicillin-clavulanic acid suspension 15 mg/kg), corticosteroids (prednisolone 2 mg/kg), maropitant (1 mg/kg) and mirtazapine (1.88 mg/cat). The owner reported worsening clinical signs 2 days later, and the cat died at home on day 28. Necropsy was not performed per the owner’s request.
Histopathological evaluation of the enucleated right eye revealed findings consistent with the cytological findings from the hindlimb; that is, large cell lymphoma (Figure 5). The iris and ciliary body were markedly expanded by a densely cellular sheet of atypical large lymphocytes (Figure 5). Neoplastic cells were also present within the vitreous chamber. A high mitotic rate was observed (8–19 per high power field), and there was hypertrophy of the retinal pigmented epithelium. The retina was detached, with multifocal loss of ganglion cells and the outer plexiform layer (Figure 5), and there was marked thinning of the sclera, particularly in the posterior globe. Immunohistochemical labelling for CD3 (ie, T-cell marker) and CD20 (ie, B-cell marker) was performed by the Michigan State Veterinary Diagnostic Laboratory. The results showed large, round cells with perimembranous CD3 immunoreactivity within the iris stroma, anterior chamber and lining the inner retinal surface. A few sloughed cells within the anterior chamber and along the inner retinal surface exhibited perimembranous CD20 immunoreactivity. These findings confirmed the diagnosis of peripheral T-cell lymphoma.
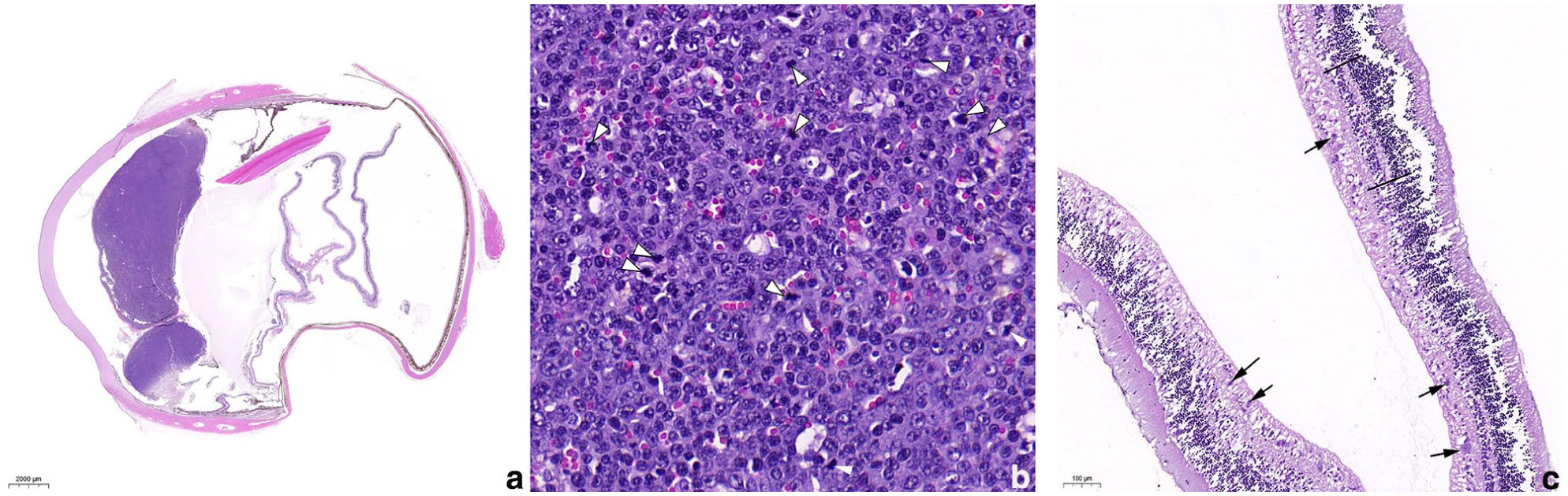
Microscopic findings in the enucleated eye (oculus dexter): (a) subgross magnification. There is diffuse infiltration of basophilic neoplastic cells into the iris and ciliary body. The retina is completely detached. There is marked thinning of the sclera in most of the caudal part of the globe. (b) The neoplastic cells have a small to moderate amount of cytoplasm and large round to slightly irregular nuclei, with one or more prominent nucleoli. They are arranged in densely cellular sheets. Mitotic figures are common (white arrowheads). (c) In the detached retina, the black arrows identify ganglion cells and the black lines mark the outer plexiform layer. Notice the multifocal loss of ganglion cells and thinning of the outer plexiform layer
Discussion
This case highlights the diagnostic complexity of primary muscular lymphoma in cats, a condition that is exceedingly rare. Although ocular signs were the initial clinical manifestations, the authors suspect that mus-cular involvement preceded ocular metastasis. Charac-terising the immunophenotype of lymphoma is vital for prognosis and treatment planning in both feline and canine patients. In cats infected with FIV, the risk of developing a lymphoid malignancy is estimated to be five- to six-fold higher than in uninfected cats. 19 In addition, FIV infection is most commonly associated with high-grade, B-cell lymphomas arising at extranodal sites. Although rare, T-cell lymphomas have also been reported in FIV-infected cats, as in the present feline patient.19,20 In dogs, T-cell lymphomas are associated with significantly shorter survival and earlier relapse compared to B-cell lymphomas (150 vs 330 days and 52 vs 160 days, respectively). 21 Although such prognostic differences are less consistently documented in cats, Wolfesberger et al 22 demonstrated that certain feline T-cell subtypes, such as intestinal T-cell lymphoma, may confer longer median survival times (1.7 years) than aggressive B-cell forms like diffuse large B-cell lymphoma, with a median survival of only 4.5 months. These findings support the clinical value of immunophenotyping in providing prognosis regarding disease progression and guiding therapeutic decision-making. Lymphoma involving the ocular tissues is typically considered part of systemic disease, as supported by previous reports.6 –9,18 However, in rare cases, intraocular lymphoma may present as a primary site of origin without detectable systemic involvement at the time of diagnosis.7,11 Musciano et al 11 highlighted this classification and the importance of differentiating PSOL from systemic lymphoma with ocular involvement, given the implications for prognosis and treatment outcomes.
Human patients are sometimes diagnosed with cancer of unknown primary site (CUP),23 –26 a diverse group of metastatic cancers where the original tumour location cannot be identified. This occurs even after a comprehensive review of medical history, a thorough physical examination and extensive diagnostic testing. The primary tumour may grow slowly or even disappear, and it rarely becomes apparent during the clinical course of the disease. Even with advancements in molecular diagnostic tools, immunohistochemistry analysis and imaging, diagnosing which metastatic site is primary sometimes remains unclear.23 –26 In this cat, the rapid clinical deteri-oration suggests that the primary neoplastic process may have originated in the quadriceps femoris muscle; however, high-grade lymphoma metastases could also progress rapidly in some cases, thus definitive confirmation is not possible without a necropsy. It remains conceivable that a post-mortem examination would have revealed involvement limited to the ocular and muscular systems, in which the patient could potentially be classified as a case of CUP.
Primary muscular lymphoma presents unique diagnostic challenges because of its atypical location and non-specific clinical signs. In addition, the protective nature of muscle tissue, including contractile activity and local biochemical factors (eg, pH, anti-tumour factors), likely contribute to the rarity of muscle neoplasms.13,14,27,28 Mori et al 13 described a case of primary muscular T-cell lymphoma in a cat, with the neoplasm exhibiting tropism for striated muscles and peripheral nerves. In addition, metastatic lymphoma to skeletal muscles has been reported in a domestic shorthair cat with primary mediastinal lymphoma and in an Abyssinian cat with epitheliotropic T-cell gastrointestinal lymphosarcoma.29,30 Although there are differences in the presentation of these cases, one notable similarity is that the affected patients were shorthaired females, with the cat in the report by Mori et al 13 being only 4 years older than the one described in this case. Lymphoma in cats typically presents in older cats with a median age of 10 years at the time of diagnosis, although cases have been described in cats aged from 2 months to 28 years.1 –5,12 –14,20 In dogs, primary lymphoma presenting with muscle involvement has been documented,11,31 –35 and several case reports describe metastatic lesions to skeletal muscles.27,35
In this case, the ocular manifestation of the disease was initially perplexing. The acute onset of signs in a cat previously considered healthy by the owner, combined with unremarkable initial bloodwork and non-diagnostic ocular cytology, suggested a solitary ocular condition. Although Linn-Pearl et al 36 demonstrated the diagnostic value of cytopathological evaluation of aqueocentesis samples, particularly for intraocular neoplasms including lymphoma, the cytology in this case, as in several other studies,36 –39 provided limited diagnostic benefits. The primary limitation of this case report is the absence of a post-mortem examination, which was not allowed by the owner; such an examination could have provided deeper insights into the full extent of organ involvement in this specific case. An additional challenge was the absence of detectable masses in any organ, which delayed the diagnosis of lymphoma until the disease had advanced to a more severe stage with ocular involvement and hindlimb lameness.
Conclusions
This case highlights the diagnostic complexity of feline lymphoma, particularly when presenting with isolated ocular signs. It was not possible to determine whether the muscle or the eye was the primary site; clinical signs were first ocular, but this does not confirm the eye as the origin. Therefore, the true primary site of disease remains uncertain. Although primary muscular lymphoma can be considered as a differential diagnosis in cats with unexplained uveitis and concurrent lameness, this case underscores that early tissue sampling and advanced imaging are essential for the timely diagnosis of atypical lymphoma presentations.
Footnotes
Acknowledgements
The authors thank Dr Dana Peery of the radiology department for performing the ultrasound evaluation, acquiring imaging and collecting the fine-needle aspirates. They also extend their sincere appreciation to the clinicians, registered veterinary nurses and support staff for their invaluable contributions to the management of this case.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognised high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed and/or this work involved the use of cadavers. Ethical approval from a committee was therefore not specifically required for publication in JFMS Open Reports. Although not required, where ethical approval was still obtained, it is stated in the manuscript.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (experimental or non-experimental animals, including cadavers, tissues and samples) for all procedure(s) undertaken (prospective or retrospective studies). For any animals or people individually identifiable within this publication, informed consent (verbal or written) for their use in the publication was obtained from the people involved.