
Abstract
Case summary
A 6-year-old female spayed Ragdoll presented with a 4-day history of acute onset non-productive retching, coughing and anorexia. A complete blood count, serum biochemistry, thoracic radiography and abdominal ultrasound were performed. Initially, aspiration pneumonia was suspected owing to an alveolar lung pattern in the right cranial ventral lung lobes seen on radiographs. The cat did not improve with empirical antibiotic therapy. Bronchoscopy and bronchoalveolar lavage were performed. An intraluminal tracheal mass was identified and removed via endoscopic guidance and gentle traction. Histopathology results were consistent with a fibrinous tracheal pseudomembrane. The cat was concurrently diagnosed with Pseudomonas aeruginosa pneumonia, which was confirmed on bronchoalveolar lavage. Pseudomonas aeruginosa was also cultured within the pseudomembrane. The cat was received antimicrobial therapy for his Pseudomonas pneumonia. In humans, fibrinous tracheal pseudomembranes occur uncommonly as a complication following endotracheal intubation and rarely due to infectious organisms. As there was no prior history of endotracheal intubation, the development of fibrinous tracheal pseudomembrane in this cat was suspected to be secondary to Pseudonomas aeruginosa aspiration pneumonia.
Relevance and novel information
The present case report is the first to describe a tracheal pseudomembrane in a cat. Bronchoscopy-guided gentle traction and subsequent removal of the tracheal pseudomembrane resulted in a complete resolution of the clinical signs.
Introduction
Fibrinous tracheal pseudomembrane is a rare condition characterised by the formation of a pseudomembrane across the trachea, resulting in respiratory obstruction. It is typically considered a complication following endotracheal intubation or secondary to tracheal trauma and, in rare cases, infection. The exact mechanisms of pseudomembrane formation are unclear but are suspected to be the end stage of tracheal ischaemic damage or extensive inflammation of the tracheobronchial tree.1,2 In the veterinary literature, there has been a previous case report of a recurrent tracheal pseudomembrane in a British Bulldog secondary to endotracheal intubation. 3 It has also been reported in foals secondary to equine herpesvirus. 4 The present case report is the first to describe a tracheal pseudomembrane in a cat, which was suspected to be secondary to aspiration pneumonia.
Case description
A 6-year-old spayed female Ragdoll presented to the referral hospital for evaluation of a 4-day history of acute onset retching and anorexia. The cat had been previously diagnosed with idiopathic hypercalcaemia which was being medically managed with weekly oral administration of 10 mg/kg alendronate (Bova Compounding Pharmacy). The cat had been previously reported to intermittently vomit after administration of alendronate. The development of retching and anorexia were noted to occur the day after the administration of alendronate.
On presentation, the cat was bright, alert and responsive. The cat was witnessed to cough with a terminal retch. As the cat was aggressive in nature, a detailed physical examination could not be performed. The cat was sedated with an intramuscular injection of 10 mg/kg tiletamine and zolazepam (Zoletil; Virbac) to facilitate handling. Physical examination under sedation was unremarkable. A complete blood count, serum biochemistry, electrolytes and venous blood gas analysis were performed. This showed a neutropenia (2.27 ×109/l; reference interval [RI] 2.3–10.29 ×109/l) and a hypophosphotaemia (0.69 mmol/l; RI 1–2.42 mmol/l). The rest of the analysis was within normal limits. Serum ionised calcium was normal.
Abdominal ultrasound identified a focal segment of the small intestine that was dilated with fluid. This was suspected to be secondary to gastrointestinal ileus. Orthogonal two-view thoracic radiographs identified an alveolar lung pattern in the right cranial ventral lung lobes (Figure 1). An echocardiogram was performed to assess for underlying cardiomyopathy causing cardiogenic pulmonary oedema as a possible explanation for the alveolar lung pattern. The echocardiogram was unremarkable.

Right lateral radiograph of the thorax was performed under sedation. There is an alveolar lung pattern in the right cranial lung lobes. Tracheal narrowing is observed at the level of the thoracic inlet.
Further diagnostics such as bronchoscopy and bronchoalveolar lavage (BAL) were recommended to the owner but declined. In light of the history of vomiting, coughing and the right cranial ventral alveolar lung pattern, aspiration pneumonia was suspected. The cat was hospitalised and empirical treatment of aspiration pneumonia was commenced. The cat was treated with 22 mg/kg amoxicillin intravenously (IV) q8h. During this time, the coughing resolved. However, exaggerated swallowing was observed and 0.02 mg/kg buprenorphine (Temvet; Troy) IV q8h was also commenced owing to concerns for oesophageal injury secondary to alendronate administration. The cat was hospitalised for 3 days and, during this time, remained hyporexic. The cat was discharged at the owner’s request on the fourth day. A single subcutaneous injection of 8 mg/kg cefovecin (Convenia; Zoetis) was administered prior to discharge.
The cat re-presented 4 days after discharge owing to progressive coughing, persistent anorexia and intermittent neck extension with open-mouth breathing. Repeat physical examination was unremarkable. Bronchoscopy and BAL were performed under general anaesthesia. Bronchoscopy identified a flesh-coloured mass that was occluding approximately 75% of tracheal lumen (Figure 2). This was removed via bronchoscopy-guided traction using paediatric biopsy forceps. Grossly, the mass was smooth, tubular and uniform, and measured approximately 10cm in length. The mass had occluded 75% of the tracheal lumen for the entire 10 cm. A blind BAL was also performed by advancing a 1.7 mm washing catheter through the lumen of the endotracheal tube until resistance was felt. Five millilitres of 0.9% sterile saline were instilled into catheter and then gently aspirated back out of the airways. The catheter was subsequently removed from the endotracheal tube after the saline was retrieved.

Flesh-coloured intraluminal tracheal mass (histologically diagnosed as tracheal pseudomembrane) seen during bronchoscopy.
Histopathology of the intraluminal mass revealed a mesh of fibrin containing pockets of haemorrhage with occasional small aggregates of neutrophils, rare hair fragments and keratin (Figure 3). Both tissue culture of the intraluminal mass and fluid culture from the BAL yielded a growth of Pseudomonas aeruginosa that was resistant to tetracyclines, penicillins and cephalosporins but sensitive to fluroquinolones. The cat was started on 5 mg/kg pradofloxacin (Veraflox; Bayer) once daily for 4 weeks.
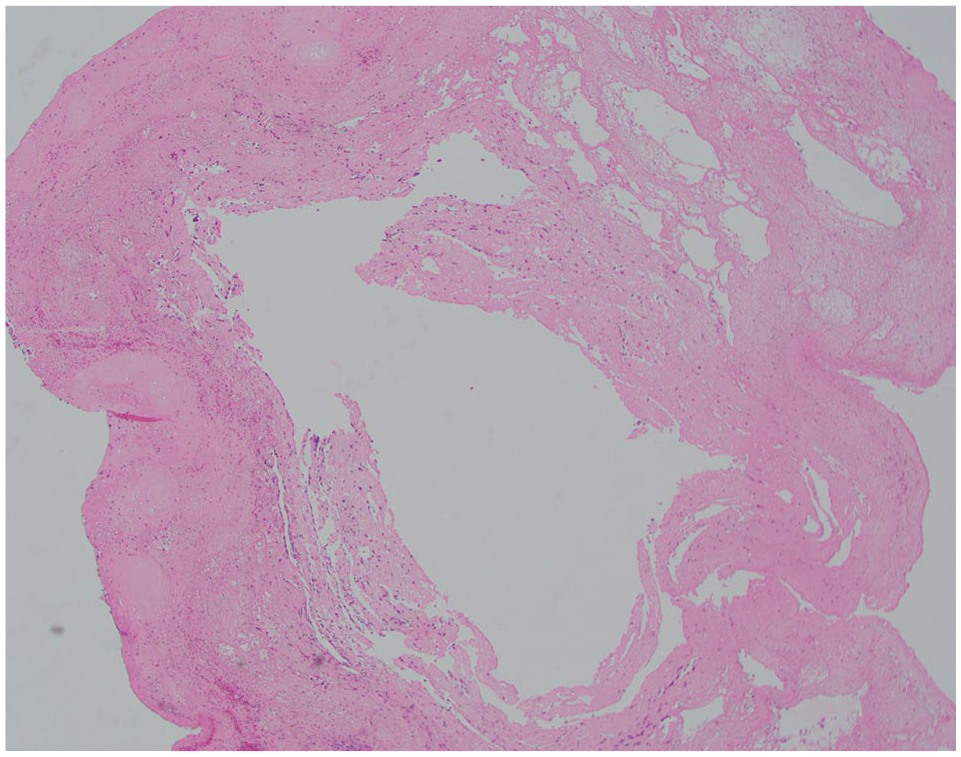
Histopathology of the intraluminal mass revealed a mesh of fibrin containing pockets of haemorrhage with occasional small aggregates of neutrophils, rare hair fragments and keratin. Haematoxylin and eosin, magnification ×4. (Courtesy of Dr Helen Owen)
The cat’s respiratory signs immediately improved following the removal of the tracheal pseudomembrane, with complete resolution of clinical signs following extubation. The cat made an excellent recovery with resolution of the coughing, retching, open-mouth breathing and anorexia. The cat was discharged the following day. Follow-up was performed at the referral hospital 4 weeks after discharge, where thoracic radiographs were offered to assess the resolution of the pneumonia, but this was declined by the owner. At the time of writing (3 months after diagnosis), the cat had no persistent or recurrence of any clinical signs.
Discussion
This is the first reported case of a fibrinous tracheal pseudomembrane in a cat. In humans, tracheal pseudomembranes that have been documented to be infectious in origin are most often reported in immunocompromised patients. In immunocompromised patients, pseudomembrane formation has been reported in association with fungal infections such as Aspergillus species, Candida species and Rhizopus species.2,5–7 Other pathogens that have been rarely associated with tracheal pseudomembrane formation include Pseudomonas species, Corynebacterium species, Bacillus species, Staphylococcus species, Diptheria species, Moraxella species and Chlamydia species.2,8 There have been sporadic case reports in human literature of pseudomembrane formation secondary to bacterial agents in immunocompetent patients. 2
There has also been a single case report documenting the formation of pseudomembrane overlying the upper larynx, vocal cord, tracheal and right main stem bronchus following aspiration of alendronate in an 84-year-old woman. 9 Given the temporal association of the administration of alendronate and the development of the cat’s clinical signs of vomiting and coughing, aspiration of alendronate should also be considered as a possible contributing cause.
The exact mechanisms of formation remain unclear, with several hypothesised mechanisms. Tracheal pseudomembranes have been described as the first step of a process that can ultimately lead to tracheal stenosis. In cases of tracheal pseudomembrane, the initial superficial tracheal necrosis leads to profuse fibrinous exudate and infiltration by polymorphonuclear cells. 1 Infectious tracheal pseudomembrane is characterised by extensive inflammation of the tracheo-bronchial tree with formation of a pseudomembrane that is composed of fibrin, leukocytes and sometimes organisms overlying a damaged airway mucosa.2,8 For those cases that develop secondary to intubation, it has been postulated that hyper-pressure at the site of endotracheal cuff leads to necrosis of the tracheal mucosa and submucosa with subsequent exposure of the cartilage, chondritis and perichondritis.1,10–13
Histopathology of the tracheal cast in this case report was consistent with a tracheal pseudomembrane due to the presence of neutrophils and fibrin. As the hair fragment and keratin were visualised within the lesion, the tracheal pseudomembrane is postulated to have developed secondary to aspiration pneumonia. The antimicrobial sensitivity profile of the P aeruginosa cultured from both the tissue and BAL were identical, which further supports this hypothesis. The aspiration is suspected to have been due to vomiting after the administration of alendronate. The cat had no known previous history or comorbidities that may have resulted in immunosuppression and therefore this is considered a rare case of tracheal pseudomembrane formation in an immunocompetent patient.
Tracheal pseudomembrane is a rare condition, even in human medicine, and therefore a strong clinical suspicion is required to diagnose this condition. Bronchoscopy is paramount to the diagnosis and treatment of tracheal pseudomembrane as direct visualisation is required to make a diagnosis and to facilitate subsequent removal. The diagnostic utility of bronchoscopy was highlighted in the case described as performing thoracic radiography and blind BAL alone would have unlikely achieved a diagnosis. However, in retrospect, there was the presence of a possible soft-tissue opacity in the cervical tracheal causing reduction of tracheal luminal diameter on the thoracic radiographs obtained at initial presentation. Cervical and thoracic CT would have been of benefit to determine the extent of the intraluminal tracheal mass and evaluate for the presence of pulmonary parenchymal disease, although it would have been unlikely to alter the diagnosis. In the current case, histopathology was useful in ruling out malignancy.
The cat was commenced on IV amoxicillin in hospital as an empirical treatment of aspiration pneumonia. Owing to difficulties in medicating the cat at home, it was elected to administer cefovecin upon discharge. In retrospect, changing antibiotic families is not ideal and commencing IV cephalosporin during the cat’s hospitalisation rather than IV amoxicillin would have been a more appropriate stewardship of antimicrobials.
Recurrence of tracheal pseudomembrane is rare in human medicine. Repeat bronchoscopy or CT is sporadically used to assess for resolution and recurrence. In the current case, repeat bronchoscopy would have been useful to document the complete resolution of the tracheal pseudomembrane.
Tracheal pseudomembrane is a differential diagnosis to consider in patients presenting with coughing or an obstructive breathing pattern with a history of general anaesthesia, tracheal trauma or infection.
Conclusions
This report describes the first case of a fibrinous tracheal pseudomembrane in a cat. Bronchoscopy and BAL were useful diagnostics in this case to determine the cause of the cat’s clinical signs. Intraluminal tracheal disease such as fibrinous tracheal pseudomembrane merits consideration in the differential diagnosis of persistent coughing and retching.
Footnotes
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This work involved the use of non-experimental animals only (including owned or unowned animals and data from prospective or retrospective studies). Established internationally recognised high standards (‘best practice’) of individual veterinary clinical patient care were followed. Ethical approval from a committee was therefore not necessarily required
Informed consent
Informed consent (either verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (either experimental or non-experimental animals) for the procedure(s) undertaken (either prospective or retrospective studies). For any animals or humans individually identifiable within this publication, informed consent (either verbal or written) for their use in the publication was obtained from the people involved.