
Abstract
Case summary
A 7-year old male neutered domestic shorthair cat was presented with a 2 month history of a slow-growing mass on the right zygomatic area. A CT scan revealed a soft tissue mass in the right zygomatic region with no alterations of the underlying bone and features of local invasiveness. Cytology was suggestive of a mesenchymal tumour and histopathology from an incisional biopsy was consistent with a soft tissue sarcoma (STS). The cat was treated with neoadjuvant intravenous doxorubicin chemotherapy at a dose of 25 mg/m2, every two weeks. The patient experienced a partial response and underwent surgical excision of the tumour. Doxorubicin was continued as an adjuvant treatment for three further chemotherapy sessions, at a dose of 25 mg/m2 every 21 days. Local tumour recurrence was detected on clinical examination and cytologically confirmed 259 days following surgery.
Relevance and novel information
Treatment with neoadjuvant doxorubicin can be considered in cases of inoperable STSs in order to cytoreduce the tumour and improve the chances of achieving complete surgical margins. The role of adjuvant chemotherapy in this setting remains unclear.
Introduction
Soft tissue sarcomas (STSs) are a group of heterogeneous mesenchymal tumours frequently arising in cutaneous and subcutaneous tissues. Feline STSs are usually feline injection-site sarcomas (FISSs), for which a histological grading has been validated and several therapeutic options have been described.1,2
Information regarding feline STSs other than FISS is sparse; however, a few case reports have described the link between STS and miscellaneous events such as foreign bodies, surgical implants, non-absorbable suture material, microchips, fluid ports and trauma.3–11 Based on histopathology, FISSs are generally classified as fibrosarcomas; however, other tumour types have been reported for both injection-site and non-injection site sarcomas in cats; these histotypes include nerve sheath tumour, malignant fibrous histiocytoma, leiomyosarcoma, liposarcoma, myxosarcoma, undifferentiated sarcoma, osteosarcoma, chondrosarcoma and rhabdomyosarcoma.12,13
Surgery is considered the main treatment in cases of STSs in both dogs and cats. Wide surgical excision is recommended for the treatment of STSs in dogs to avoid local tumour recurrence (usually 3 cm for lateral margins and one fascial plane in depth), although low-grade tumours are reported to recur less frequently, even in the case of incomplete excision.14,15 Regarding FISS, the Vaccine Associated Feline Sarcoma Task Force has recommended a minimum of 2 cm margins for both lateral and deep margins. 16 A recent study on 131 cats reported a recurrence rate of 38.1% when wide-margin surgery was performed (3 cm for lateral margins and full-thickness body wall resection or a minimum of two fascial planes depending on tumour location). 17 A more radical approach with 3–5 cm margins has also been recently described; cats experienced a longer disease-free interval (DFI) than previously reported, suggesting wider margins may affect recurrence rates. 18
The role of radiation therapy (RT) in the treatment of FISS has also been investigated. Studies reporting the use of neoadjuvant and adjuvant RT and RT alone in a palliative setting are numerous. However, recurrence rates range from 28–45% and there is still no convincing evidence that radiotherapy may be effective at prolonging the DFI in cases of FISS.19–21 In a study with 10 cats treated with liposomal doxorubicin as a radiation sensitiser, palliative RT was used resulting in seven partial responses (PRs) and two complete responses, with a median progression-free interval of 117 days. 22
Chemotherapy as a neoadjuvant treatment is still not widely used in veterinary oncology although it has been described for FISS.23,24
The first study evaluating neoadjuvant and adjuvant doxorubicin administration in comparison with surgery alone in the treatment of FISSs found no statistically significant difference in outcome when comparing the two groups. 23 Recently, the efficacy of epirubicin, a stereoisomer of doxorubicin, in the treatment of FISSs has been reported. In those cats where neoadjuvant chemotherapy was used, the DFI and tumour-free survival were longer than in historical controls. 24
However, data regarding the use of neoadjuvant chemotherapy in the treatment of feline non-FISS STSs prior to surgical excision are lacking.
The authors here describe an STS in a cat treated with neoadjuvant doxorubicin prior to surgical excision and followed by adjuvant chemotherapy.
Case description
A 7-year-old male neutered domestic shorthair cat was referred to our institution for the evaluation of a slow-growing subcutaneous mass in the right zygomatic region, first noted 2 months earlier. On physical examination, the patient was bright and alert; its body weight was 5.5 kg. A firm, non-painful subcutaneous nodule measuring 25 × 20 mm (caliper measurements) was detected in the subcutis of the right ventral eyelid (Figure 1). There was no peripheral lymphadenopathy and no other abnormalities could be identified on clinical examination.

The patient at the time of presentation. The mass extends from the upper portion of the right lip towards the right ventral eyelid
Diagnostic work-up included haematology, biochemistry and urinalysis, which were within normal limits, together with fine-needle aspirates of the mass.
Cytological findings were consistent with a mesenchymal neoplasia; therefore, a contrast-enhanced CT scan of the head, thorax and abdomen was performed for surgical planning and to rule out metastatic disease. An incisional biopsy of the tumour was performed at the same time.
CT findings showed a 16 mm mass arising from the soft tissues in the right zygomatic region, with mild-to-moderate local invasiveness of the surrounding tissues and a moderate and heterogeneous enhancement following contrast administration. There were no lytic or proliferative changes of the bones. No changes suggestive of local or distant metastases were detected (Figure 2). Histopathology confirmed a diagnosis of fibrosarcoma, which was consistent with a low-grade STS according to FISS classification. 1

CT scan of the head. Transverse view of the mass. Soft tissue (a) and bone (b) windows. The mass appears to involve the subcutaneous tissue (a); no bone involvement is observed (b)
The extension of the tumour and its location were not amenable to conservative surgery with complete surgical margins; orbitectomy was offered but declined by the owner. Therefore, neoadjuvant doxorubicin was administered with the purpose of reducing the tumour’s dimensions prior to surgery.
A complete blood count and baseline serum biochemistry were checked before each chemotherapy administration, with particular attention to the renal parameters, owing to the potential nephrotoxicity of doxorubicin in cats.25,26 Doxorubicin was administered at a dose of 25 mg/m2 as a slow intravenous (IV) infusion, following premedication with IV maropitant at 1 mg/kg. Treatments were administered every 2 weeks up to a total of three treatments. Serial caliper measurements were performed at the time of each follow-up revisit. Overall, chemotherapy was well tolerated; a sporadic, self-limiting gastrointestinal (GI) toxicity (nausea) was reported by the owner and no clinical signs of renal toxicosis or any haematological toxicity were detected. This was classified as grade I according to the Veterinary Co-operative Oncology Group (VCOG) Common Terminology Criteria for Adverse Events. 27
Since the first chemotherapy administration, the tumour mass became softer and appeared to have lesser extension towards the surrounding tissues (caliper measurement 23 × 19 mm); following the second treatment, a reduction in tumour volume became evident (20 × 19 mm), although it was not sufficient to be classified as a PR, according to the VCOG Response Evaluation Criteria In Solid Tumours. 28 Following the third treatment, a 39% reduction in tumour volume was detected (final caliper measurement 16 × 19 mm), and deemed compatible with a PR. The degree of cytoreduction was considered sufficient for the patient to undergo surgical removal of the mass and it was admitted for surgery 48 days after following chemotherapy initiation (Figure 3). A second CT scan was not considered necessary to assess clinical response and to make a surgical plan. In fact, together with the reduction in size, the tumour appeared more mobile; moreover, CT findings at presentation showed only soft tissue involvement.

The patient after three treatments with doxorubicin. The mass has reduced by 39% of its original volume and there is a lesser extension towards the right eye and surrounding structures
Following a cutaneous incision, the mass was carefully isolated from the surrounding tissues with Metzenbaum scissors and electrocautery, by keeping a 1 mm distance from the lower eyelid. The dorsal branch of the ipsilateral buccal nerve and the rostral portion of the ipsilateral maxillary nerve were resected and the mass removed. The surgical wound was closed using a single advancement flap and a closed suction Redon drain was placed before suturing the surgical wound (Figure 4).
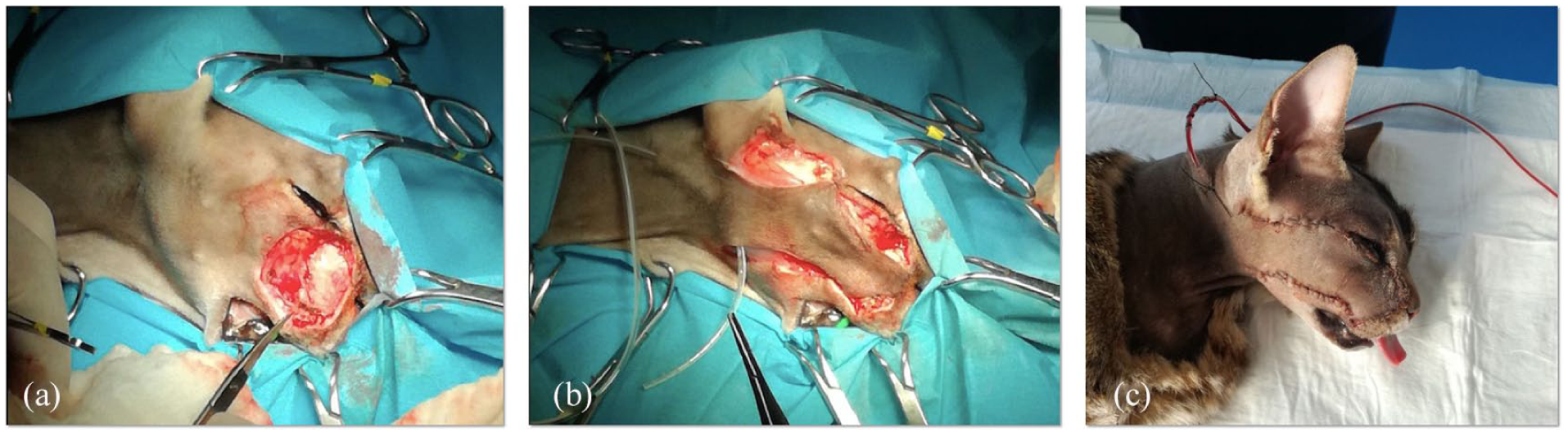
Intraoperative picture. The tumour was (a) excised and (b) a single advancement flap was created to correct the surgical defect. (c) At the end of the procedure, a closed suction drain was positioned before wound closure
The patient was hospitalised for postoperative care and analgesia; the drain was removed 24 h after surgery and the patient discharged on the same day.
Histopathology confirmed an STS, consistent with fibrosarcoma, characterised by peripheral aggregates of small mature lymphocytes resembling FISS morphology (Figure 5). The association of neoplastic spindle cells and lymphocytic infiltrate led to the application of the FISS histological grading score and the tumour was classified as a grade II STS. The ventral margin of the sample was infiltrated by tumour cells.

Histopathology section. Neoplastic cells expand the dermis, the tumour appears to be moderately differentiated, no necrosis is observed and mitoses are 1 per 10 high-power field (HE×400). Aggregates of small mature lymphocytes are observed mainly at the periphery of the tumour (arrow)
Adjuvant doxorubicin was started 20 days after surgery. Three total treatments were administered every three weeks at a dose of 25 mg/m2 as a slow IV infusion, following administration of maropitant at 1 mg/kg IV. Adjuvant chemotherapy was overall well tolerated: a sporadic, self-limiting VCOG grade I GI toxicity (nausea and vomiting) was reported. No recurrence was noted throughout the treatment protocol. Overall, the cat received a total dose of 150 mg/m2 doxorubicin, which was equally divided between the neoadjuvant and the adjuvant protocols. The patient was re-evaluated every 3 months following completion of chemotherapy; no evidence of local recurrence was detected and thoracic radiographs did not show any changes compatible with distant metastases (Figure 6). However, at the time of the third follow-up revisit, local recurrence was suspected and confirmed on cytology. The cat remained disease-free for 259 days following surgery and it is alive at the time of writing.

The patient at the time of follow-up, 170 days following surgery. The wound is healed and there is an acceptable cosmetic appearance There are no signs of local tumour recurrence
Discussion
This case report describes the use of neoadjuvant chemotherapy in a case of feline STS; although orbitectomy was strongly suggested to possibly achieve complete margins in our case, this option was declined by the owner. The type of surgical approach used was the likely reason the tumour appeared to be incompletely excised; however, the DFI was >8 months. The clinical suspicion of mesenchymal neoplasia was confirmed by cytology and a definitive diagnosis achieved on histopathology. The histopathological features of the tumour (ie, proliferation of neoplastic mesenchymal cells together with lymphocytic aggregates at the periphery of the sample) had important similarities to those features that are usually observed in cases of injection-site sarcomas, which is the reason why the FISS grading was applied. 1 The histological grade is considered to be one of the most important prognostic factors for both local tumour recurrence and metastatic rate in human and canine STSs.29,30 Tumour grade has been evaluated as a potential prognostic factor for FISS, with patients affected by grade III tumours having a higher risk of developing distant metastasis in one study. 31 However, tumour grade could not be definitely associated with a higher chance of local tumour recurrence in cats, and, as such, the usefulness of histological grading in predicting the outcome has been questioned.1,31–33 Little is known about STSs and their histological grading in cats; therefore, any correlation between tumour grade and prognosis in this case may be biased by the use of the grading criteria established for FISS.
Owing to the presence of lymphocyte infiltration on histopathology, a traumatic or primary inflammatory injury was suspected to be the inciting cause of the tumour in our case, similarly to what has been reported for FISS. 12 Generally, the head and neck region is not commonly affected by STSs in cats: in one study investigating surgery for the treatment of 42 non-visceral STSs, only 2/42 tumours were in this location, with the majority of STSs affecting the trunk. 13 In cats, the onset of sarcomas secondary to vaccination, long-acting antibiotics or steroids, benzonylurea pesticide lufenuron, non-absorbable suture material, microchip implants, retained surgical sponges, fluid ports or trauma has been documented.3–11,34,35 In fact, morphological features of this STS on histopathology paralleled those generally described for FISS, 12 where the presence of inflammation was characterised by peripheral, nodular lymphoid aggregates, as observed in our case. Chronic inflammation has been associated with a wide range of malignancies and is well known to have a role in the pathogenesis of a variety of cancers.36–38 Moreover, tumour onset has been linked to chronic inflammation elicited independently on the initiating cause and it is probably caused by growth factors produced by inflammatory cells. 39
In the light of the clinical and CT findings, the tumour could not be completely removed with a conservative surgery. The authors elected to start a neoadjuvant chemotherapy protocol, with the intent of achieving cytoreduction in view of a curative-intent surgery. The role of neoadjuvant chemotherapy has been investigated in FISS. One study found no difference in outcome between those cats treated with neoadjuvant doxorubicin and surgery and those patients treated with surgery alone. 23 In another study, a reduction in tumour size was observed in 5/21 cats, with 3/5 experiencing a complete response following a median of three courses of neoadjuvant epirubicin. Local tumour recurrence was detected in 14% of cases and the 2 year survival rate was 81% (median survival time was not reached). 24 In this case report, a PR was observed following three biweekly treatments. Neoadjuvant doxorubicin was administered at a dose of 25 mg/m2 every 2 weeks, aiming for an acceptable degree of cytoreduction prior to surgical excision. 40 The authors elected to choose a fortnightly intervals to shorten the period of time between treatments and try to achieve a measurable response; given the good tolerability following the first treatment, chemotherapy was continued at the same time interval for another two administrations.
The histological appearance of the surgical margins revealed evidence of residual disease. Completeness of surgical margins is widely recognised as a crucial prognostic factor for local tumour recurrence in human and canine STSs.29,30
Controversies exist on whether infiltrated histological margins are a negative prognostic factor for FISS: in one study, tumours with incomplete margins recurred about 10 times more frequently than in those patients that underwent complete excision. 1 Following surgery, adjuvant RT on microscopic disease was also discussed with the owner; however, for logistical reasons, this option was declined.
Chemotherapy was therefore continued to possibly reduce the chance of local recurrence, although its role in this setting is controversial. Treatment was continued every three weeks following surgery, as per the owner’s request, for logistical reasons. No differences in chemotherapy adverse events were noted between the neoadjuvant and adjuvant doxorubicin administration.
Conclusions
This case report suggests that neoadjuvant doxorubicin might be considered in cases of feline STSs, as similarly reported for FISS, and it appears to be associated with low-grade toxicities. The role of adjuvant chemotherapy in this setting remains unclear and would need further investigations in large-scale studies.
Footnotes
Acknowledgements
The authors would like to thank Dr Andrea Botazzoli for providing the CT pictures.
Author note
This case report was presented in abstract form at the ISFM Congress, Sorrento, Italy, 27 June–1 July 2018.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study involved the use of client-owned animal(s) only, and followed internationally recognised high standards (‘best practice’) of individual veterinary clinical patient care. Ethical approval from a committee was not therefore needed.
Informed consent
Informed consent (either verbal or written) was obtained from the owner or legal guardian of all animal(s) described in this study for the procedure(s) undertaken. For any animals or humans individually identifiable within this publication, informed consent for their use in the publication (verbal or written) was obtained from the people involved.