
Abstract
Objectives
Biological behaviour and treatment options of non-injection-site soft tissue sarcomas (nFISS) in cats are less well understood than in dogs. The aim of this retrospective study was to assess the outcomes of cats with nFISS following treatment with adjuvant radiotherapy.
Methods
The medical records of cats with soft tissue sarcomas in locations not associated with, and histology reports not suggestive of, injection-site sarcomas were reviewed. All cats underwent adjuvant radiotherapy, either hypofractionated (32–36 Gy delivered in weekly 8–9 Gy fractions) or conventionally fractionated (48–54 Gy delivered in 16–18 3 Gy fractions) to microscopic disease.
Results
In total, 18 cats were included in the study, 17 with extremity nFISS and one with facial nFISS. Nine received radiotherapy after a single surgery and nine after multiple surgeries for recurrent nFISS. Eight cats were treated with a hypofractionated protocol and 10 with a conventionally fractionated protocol. The median follow-up time was 540 days (range 51–3317 days). The tumour recurred in eight (44.4%) cats following adjuvant radiotherapy; it recurred in three (37.5%) cats following a hypofractionated protocol and in five (50%) cats following a conventionally fractionated protocol. The overall median progression-free interval (PFI) for 17/18 cats was 2748 days, while the median PFI for the 7/8 cats with recurrence was 164 days. The recurrence for one cat was reported, but the date was unknown and it was therefore censored from these data. When stratifying based on the protocol, the median PFI for hypofractionated and conventionally fractionated protocols was 164 days and 2748 days, respectively. Statistically, there was no significant difference between the two protocols (P = 0.636).
Conclusions and relevance
Adjuvant radiotherapy resulted in good long-term tumour control in 12/18 cats with nFISS. Further studies in larger populations are required to assess the significance of radiation dose and fractionation on tumour control and the effect of multiple surgeries prior to initiation of radiotherapy on outcome.
Introduction
Soft tissue sarcomas (STSs) are reported to account for 7–9% of all malignant skin and subcutaneous tumours in cats 1 and include fibrosarcoma, perivascular wall tumour, non-plexus derived peripheral nerve sheath tumour, liposarcoma, myxosarcoma, pleomorphic sarcoma (or malignant fibrous histiocytoma), malignant mesenchymoma and undifferentiated sarcoma. 2 These tumours are considered as a group because they typically have similar pathological appearance and clinical behaviour, although this may be an overly simplistic interpretation. They may arise in any anatomic site, have locally expansile growth patterns, tend to appear pseudoencapsulated, have poorly defined histological margins and have a low-to-moderate local recurrence rate following surgical excision. 3
Biological behaviour of STSs in cats is not well understood and is assumed to be similar to dogs; however, no approved histopathological grading system exists for cats. A grading scheme for STSs from human medicine4 that differentiates grades based on cellular differentiation, presence or absence of necrosis and mitotic count (MC) (Table 1) has previously been used to categorise canine STSs and has been used in some studies.5,6 Further studies are required to determine whether this grading system has prognostic value in cats. The lack of information regarding prognostic values and grading system is partly due to the relative rarity of feline non-injection site sarcomas (nFISSs). In contrast, so-called feline injection site sarcomas (FISSs) have been extensively studied, and more robust prognostic criteria exist for this subtype of sarcoma. Factors reported to be associated with local control in FISS include completeness of excision, size of the tumour, MC and anatomical site of the tumour, and factors such as size of the tumour, MC and development of distant metastasis were reported to be associated with overall survival in FISS.7–13 In one study, a high grade was associated with development of distant metastasis, 13 although subsequent studies failed to show the correlation.9,12
Canine soft tissue sarcoma grading system 4

hpf = high power field
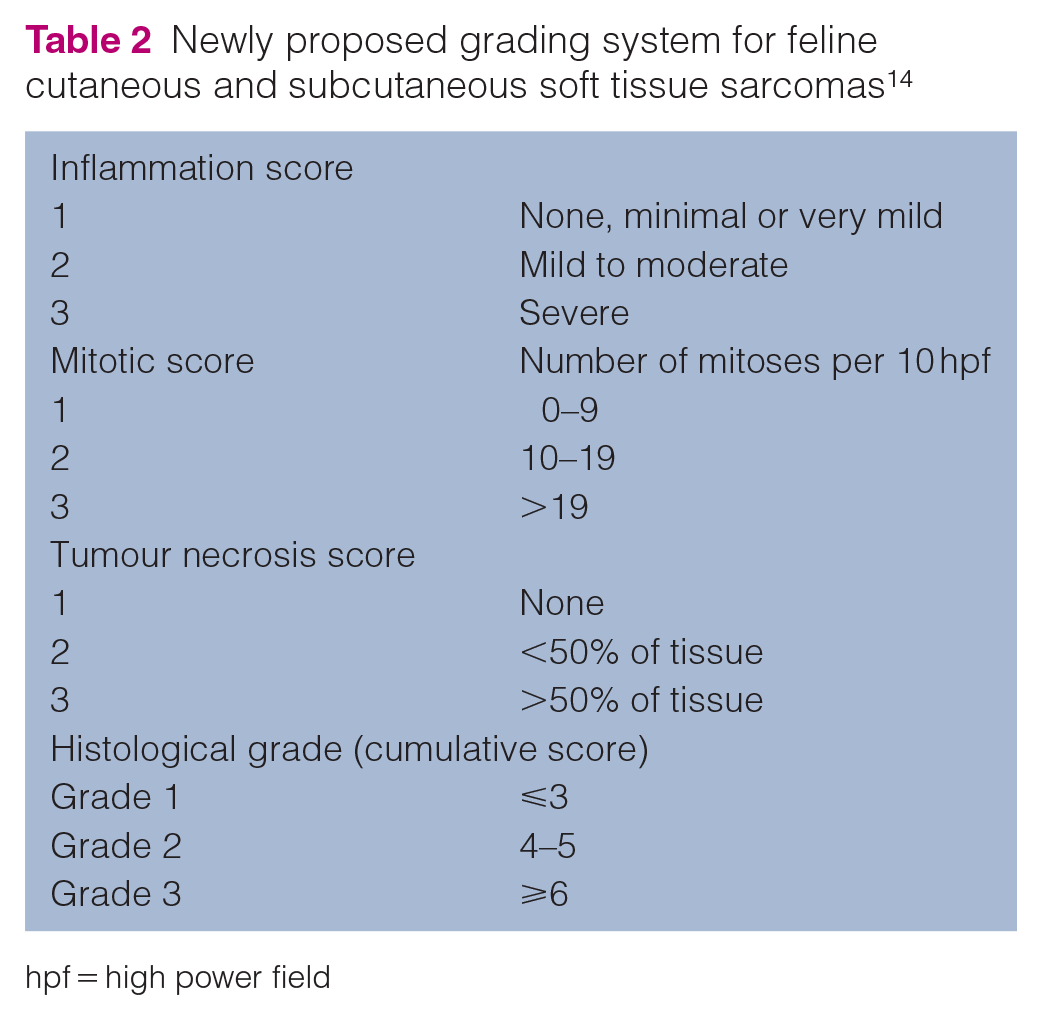
Recently a study was published, which listed prognostic factors and proposed a new grading system for all feline cutaneous and subcutaneous STSs. This grading system would allow one grading system for both FISS and nFISS and was shown to be more predictive of the prognosis based on the grade assigned (Table 2). 14 Subsequently, however, a review of histological grading systems in veterinary medicine was published and discouraged the application of the new grading system proposed until larger prospective studies are performed, due to lack of information on the proportion of FISSs and nFISSs, and lack of information on the status of surgical margins. 15
Newly proposed grading system for feline cutaneous and subcutaneous soft tissue sarcomas 14
hpf = high power field
While there is no gold standard for differentiation between FISS and nFISS in cats, various histological features have been identified that are suggestive of a diagnosis of FISS. Cats with FISS tend to be younger (median 8 years) than cats with nFISS (median 11 years).16–18 Certain anatomical areas may be more suggestive of FISSs, as they occur at sites typically used for vaccination and injections, such as the interscapular region, the lateral thoracic or abdominal wall and the lumbar region. They occur more frequently in the hypodermis, while nFISSs occur more frequently in the dermis. The preferential development in the hypodermis is believed to be due to subcutaneous administration of vaccines and injections.5,16,19 FISSs tend to have histological features that correspond to aggressive biological behaviour more often than nFISSs, which is consistent with the higher number of high-grade tumours in the FISS classification. Marked nuclear and cellular pleomorphism was a feature of 60–64% of FISSs, whereas it was seen in only 17–36% of nFISSs.5,16 Another feature of FISSs is increased tumour necrosis and higher mitotic activity.5,16 More than 20 mitotic figures in 10 high power fields (hpf) were noted in 50% of FISSs and only 13% of nFISSs, whereas less than 10 mitotic figures were present in only 10% of FISSs and 61% of nFISSs. 5 Therefore, when applying the canine grading system, FISSs are reported to have a higher tumour grade; 70% were classed as high grade, as opposed to only 9% of nFISS in a study by Aberdein et al. 5 The presence of a peripheral inflammatory cell infiltrate consisting of lymphocytes and macrophages is more commonly seen in FISSs and was reported in 59–100% of tumours as opposed to 0–33% in nFISSs5,6,16 as well as the presence of multinucleated giant cells, which was observed in 30–50% of FISSs and 0–13% of nFISSs.5,6 A prominent myofibroblastic component,6,20 and often the presence of macrophages containing blue-grey intracytoplasmic material, was also reported in multiple FISS studies.6,16,19,20 Based on these characteristics, it is suggested that FISSs and nFISSs arise as a consequence of different oncogenic mechanisms. In particular, the pathogenesis of FISS is likely secondary to chronic inflammation with neoplastic transformation of the mesenchymal cells that participate in the connective tissue repair. 19 Immunological response to tumour antigens may also contribute to the inflammatory response. 16 Immunohistochemistry revealed additional differences between the two tumour types. Of FISSs, 64–70% were shown to express smooth muscle actin as opposed to 20–29% of nFISSs.5,6 However, expression of desmin was similar between FISSs and nFISSs.5,6,21
While general recommendations regarding treatment options and their prognosis are well known for FISSs, to date there are no studies reporting the clinical management of nFISSs and the standard of care is extrapolated from canine patients.
In dogs, definitive treatment options for STSs depend on tumour size, tumour location, clinical stage, histological grade and completeness of surgical margins. 22 Local tumour control is the most important management consideration because of their locally aggressive behaviour. The mainstay of treatment is wide surgical resection,22–24 but adjuvant radiation therapy can play an important role in local tumour control, especially for incompletely resected STSs.25–30
The aim of this retrospective study was to evaluate and assess the outcomes of cats with nFISSs following surgical excision and adjuvant radiotherapy, with regard to the progression-free interval (PFI). A secondary objective was to assess the prevalence of metastasis in this population.
Materials and methods
Patients
Medical records of all cats with histologically confirmed STSs that underwent radiotherapy at a single UK referral centre between 2006 and 2017 were reviewed.
Only cats with STSs in locations not associated with injection sites, and histopathology reports not suggestive of FISS, were included in the study. Sites defined as injection sites were interscapular/scapular, flank/paralumbar, dorsolateral thorax, dorsal area of back and cervical region. Records were reviewed for exclusion of cats with tumours located in an area consistent with any of the recommended vaccination sites, when cats were vaccinated according to the feline vaccination guidelines initially published by the American Association of Feline Practitioners in 1998, 31 and later updated in 2006 32 and 2013. 33 Records were also reviewed for exclusion of cats where the site of injection of other medications was recorded and associated with the site of the tumour. A histopathology report suggestive of FISS included all of the following histological features: marked nuclear and cellular pleomorphism; moderate to marked tumour necrosis; high mitotic activity (>10 mitotic figures per 10 hpf); presence of a peripheral inflammatory cell infiltrate consisting of lymphocytes and macrophages; and presence of giant multinucleated cells, regardless of the degree of inflammation.
Inclusion criteria required a histopathology report from the whole tumour, and a minimum of 28 days follow-up after completion of radiotherapy. The study included only cats that presented either with inadequate clean but narrow margins defined as neoplastic cells within <5 mm of the surgical margin or with only microscopic disease left behind.
Cats were excluded if the tumour occurred in the nasal or oral cavity, and if any other neoadjuvant or adjuvant treatment (eg, chemotherapy) was used. Histopathology reports were reviewed by three clinicians (two diplomates in oncology; ALZ, SM and AH), all authors of this paper.
Clinical information
Data collected from medical records included signalment (age, sex, breed), concurrent diseases, results of staging tests performed (haematology, biochemistry, radiography, ultrasound, CT), number of surgeries and date and cause of death or loss to follow-up.
Tumour information
Data collected from medical records and histopathology reports included the following: tumour presentation (first occurrence or recurrent); anatomical location (head or extremities); histopathology findings (nuclear and cellular pleomorphism, presence of necrosis, mitotic count, presence of peripheral inflammatory cell infiltrate and giant multinucleated cells, grade of the tumour if applied, status of surgical margins and final diagnosis); and PFI (time between initiation of the radiotherapy and detection of local recurrence or metastasis).
Radiotherapy information
Data collected from medical records included the following: type of radiotherapy protocol (conventionally fractionated vs hypofractionated); total dose delivered; average energy (6 MV) of radiation beam; type of planning modality used (manual vs computer planning and type of accessories used for the planning); and reported toxicity (acute and late). Toxicity was graded according to the Veterinary Radiation Therapy Oncology Group (VRTOG) criteria (Table 3). 34
Veterinary Radiation Therapy Oncology Group morbidity scoring scheme for skin/hair 34

Radiotherapy
All cats were treated with external-beam megavoltage radiotherapy with a 6 MV linear accelerator (Varian Clinac 600C). Radiation was delivered via 6 MV photons with either a single beam or parallel opposed beams. Hypofractionated protocols consisted of four weekly fractions and conventionally fractionated protocols consisted of 16–18 daily fractions. All radiation therapies were planned by a diplomate in radiation oncology.
Manual planning was used in all cats. Tissue-equivalent bolus material of 0.5–1 cm was used in all cats to improve dose distribution and to adjust the dose depth profile to include superficial tissues in the target volume. Blocks were used for beam shaping and to preserve vital structures. The clinical target volume (CTV) was planned to include the surgical scar and a surrounding margin of clinically normal tissue to account for subclinical microscopic disease, commonly 3 cm where possible. The specific assignment of the lateral margins varied in different directions based on the incision location. On the extremity cases, this included the width of the limb and spared only a thin skin strip to preserve the lymphatics. The proximodistal margin information was not clearly documented as, unfortunately, the size of the tumour/length of the scar was not commonly reported in the clinical record.
Endpoint recording: follow-up procedures
If the cat was not evaluated at the referral centre, follow-up information was obtained by medical record review obtained from the referring veterinary surgeon.
PFI was calculated for each cat and defined as the time (days) between the initiation of radiotherapy and the onset of local recurrence of tumour or distant metastasis. The remaining cats were censored to the day of death or to last follow-up.
Follow-up time was calculated for each cat and defined as the time (days) between the initiation of the radiotherapy and the day of death or to last follow-up.
Statistical analysis
The Kaplan–Meier method and the log-rank test were used to compare PFI between the hypofractionated and conventionally fractionated protocols. Other variables, such as MC, grade of the tumours, number of surgeries performed before initiation of radiotherapy and time between the last surgery and initiation of radiotherapy were evaluated for prognostic significance.
Data were analysed with SPSS statistics software programme 27.0. P values <0.05 were considered significant.
Results
Population
A total of 18 cats were included in the study (Table 4). The median age was 9.5 years (range 3.8–17.6). There were six spayed females, nine castrated males, two female entire cats and one male entire cat. Of these, 14 (77.8%) were domestic shorthair cats, two were domestic longhair cats, one was a Burmese and one was a Korat.
Signalment

hpf = high power field; FN = female neutered; DSH = domestic shorthair; HF = hypofractionated; MN = male neutered; DLH = domestic longhair; CF = conventionally fractionated; F = female entire; M = male entire
Seven cats (38.9%) had haematology performed, five (27.8%) had packed cell volume (PCV) and total solids (TS) and one haematology and PCV/TS. In one of the cats, mild leukocytosis due to neutrophilia and monocytosis was reported. All cats had at least basic biochemistry performed (urea, creatinine, glucose, serum alanine aminotransferase, alkaline phosphatase and lipase).
A total of 11 (61.1%) cats had thoracic radiographs performed. Two cats had radiographs of the affected limb and one cat had radiographs of the abdomen. One of the cats with thoracic radiographs had subsequent abdominal ultrasound performed. One cat with the STS located on the head had CT of the head and thorax. Only one cat had fine needle aspiration of the regional lymph nodes. In these staged cats, no regional or distal metastatic lesions were detected.
Six cats (33.3%) had fine needle aspirates of the tumour taken before the first surgical intervention at the referring veterinary surgeons, and only one cat had a biopsy of the tumour before the first surgery.
One of the cats was also diagnosed with a mast cell tumour and a trichoblastoma. The trichoblastoma was completely excised at the time of the second excision of the STS. The mast cell tumour was completely excised at the time of the third revision surgery for the STS. One of the cats was diagnosed with pyogranulomatous steatitis in the interscapular region based on fine needle aspiration. None of the masses were associated with the site of the STS in these two cats. One cat was on treatment with carbimazole for hyperthyroidism, one was diagnosed with idiopathic cystitis and one was diagnosed with bronchitis at the time of staging based on CT of the thorax and bronchoalveolar lavage. The cat was treated accordingly.
Tumour characteristics and location
Regarding the tumour location, 17 (94.4%) cats had tumours on the extremities and one had a tumour on the head. Of the tumours on the extremities, 12 (70.6%) were located on the forelimbs, six on the right forelimb and six on the left forelimb, with only one located above the elbow at the level of the caudal aspect of humerus and 11 of them located distal to the elbow, nine at the level of the carpus or distal to it. Five tumours (29.4%) were located on the hindlimbs, two on the right and three on the left, with only one located above the stifle at the level of the lateral femur, one at the level of stifle and three at the level of the hock or distal to it.
Eight tumours were described as STSs with one of them being most likely a peripheral nerve sheet tumour and 10 were described as fibrosarcomas.
MC, defined as the number of mitotic figures in 10 consecutive hpfs at 400 × magnification, was reported in 15/18 cases. Of them, eight (53.3%) tumours had an MC <9 and seven (46.7%) had an MC ⩾9.
The canine grading system was applied in 15/18 cases. Of the 15 cases, eight (53.3%) were classified as low-grade, four (26.7%) as intermediate-grade and three (20%) as high-grade tumours.
The surgical margins were reported in all submitted samples. In 15 (83.3%) cases, tumour cells extended to the margins of the samples evaluated. In one case, 1 mm margins were reported; in one case, the pathologist reported the margins as narrow and indicating barely adequate excision, but the margins were not quantified; and in one case, the pathologist reported the margins were tumour free. However, the margins were again not quantified and, due to the location of the tumour (palmar aspect of the metacarpus), wide excision (>5 mm) was considered to be highly unlikely.
Surgical procedures
Nine cats (50%) had only one surgical procedure prior to radiotherapy, four (22.2%) cats had two surgical procedures, four (22.2%) had three surgical procedures and one (5.6%) cat had four surgical procedures prior to initiation of radiotherapy. The median time between the first and second surgery was 169 days (range 23–647 days). The median time between the second and third surgery was 91 days (range 18–952 days). All subsequent surgeries were performed due to local recurrence.
The majority of cats (15/18) had the initial surgery performed by the referring veterinary surgeon. The debulking surgical revision prior to starting with adjuvant radiation therapy in cats that underwent multiple surgeries was performed by a diplomate in surgery in 8/9 cats.
Radiotherapy
The median time from the last surgery to the start of radiotherapy was 28 days (range 13–69 days).
Eight cats were treated with a hypofractionated radiotherapy protocol (three cats with 8 Gy × 4 and five cats with 9 Gy × 4) and 10 cats were treated with a conventionally fractionated radiotherapy protocol (eight cats with 3 Gy × 16 and two cats with 3 Gy × 18). Biological effective dose (BED) was calculated for each protocol and is described in Table 5.
Biologically effective dose

BED3 = biologically effective dose using α/β = 3; BED10 = biologically effective dose using α/β = 10; BED4.9 = biologically effective dose using α/β = 4.9
Acute toxicity was reported in six (75%) cats that underwent a hypofractionated protocol, including VRTOG grade 1 toxicity in five cats (alopecia) and grade 2 toxicity (moderate dermatitis) in one cat. In the cats that underwent a conventionally fractionated protocol, acute toxicity was reported in six (60%) cats, all with VRTOG grade 1 toxicity (alopecia, dry/minimal/mild dermatitis). In terms of late toxicity, VRTOG grade 1 leukotrichia was reported in three (16.7%) cats. All of them underwent a conventionally fractionated protocol.
Outcomes
The tumour recurred in eight (44.4%) cats following adjuvant radiotherapy (Table 6). It recurred in three (37.5%) cats following a hypofractionated protocol and in five (50%) cats following a conventionally fractionated protocol.
Outcomes
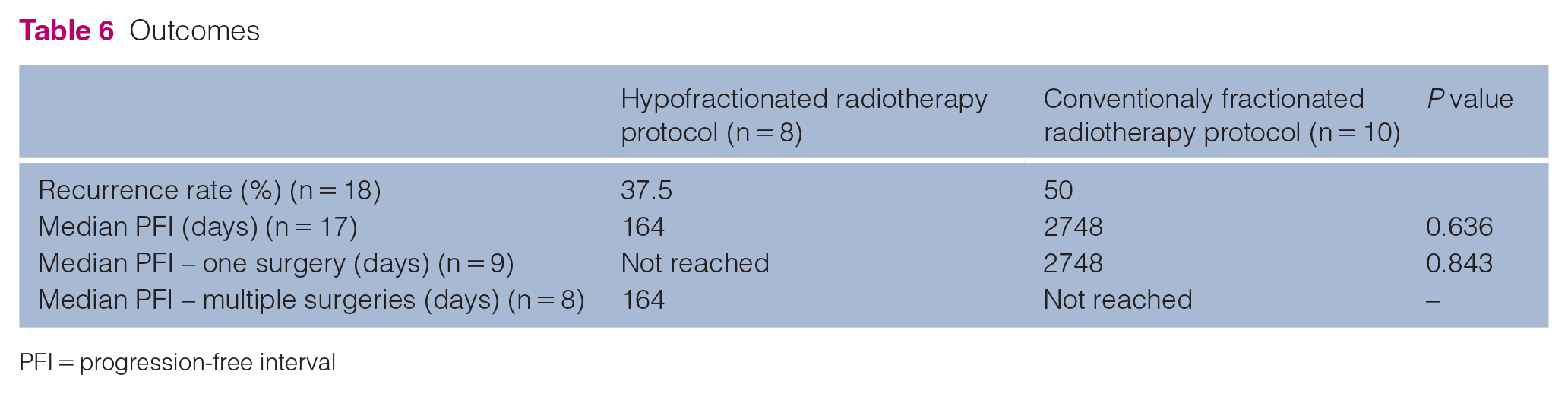
PFI = progression-free interval
The median follow-up time for which the cats were monitored was 540 days (range 51–3317 days).
The overall median PFI for 17/18 cats was 2748 days while the median PFI for 7/8 cats with recurrence was 164 days. The recurrence for the other cat was reported, but the date was unknown and it was therefore censored from these data. When stratifying based on the radiotherapy protocol, the median PFI for the hypofractionated protocol was 164 days compared with 2748 days for the conventionally fractionated protocol. Statistically, there was no significant difference between the two protocols (P = 0.636) (Figure 1).

Progression-free interval (PFI) for hypofractionated and conventionally fractionated radiotherapy protocols. PFI is not statistically significant between the two protocols (P = 0.636)
When assessing the grade of the tumours that recurred, the grade was reported in 6/8 cases. The tumour recurred in four (50%) low-grade tumours, one (25%) intermediate-grade tumour and one (33.3%) high-grade tumour. In the group treated with a hypofractionated radiotherapy protocol, the grade was reported in only 1/3 cases and it was reported as intermediate grade. The MC in this case was 6/10 hpf. This patient underwent multiple surgical excisions before initiation of adjuvant radiotherapy. The other two cases had an MC of 30/10 hpf and 50/10 hpf. Both had only one surgical procedure before initiation of radiotherapy. In the group treated with a conventionally fractionated radiotherapy protocol, one tumour was reported as low grade and one as high grade in the patients that underwent a single surgical excision before initiation of adjuvant radiotherapy. The MC was reported only for the high-grade tumour as 15/10 hpf. The remaining three tumours were reported as low grade in the patients that underwent multiple surgical excisions before initiation of conventionally fractionated radiotherapy protocol. The MC was reported as 1/10 hpf in one case and 4/10 hpf in two cases.
When comparing the two protocols in patients that underwent a single surgical excision before initiation of the radiotherapy (9/18 cats), the median PFI for the patients treated with a hypofractionated radiotherapy protocol (6/18) was not reached and for the patients treated with a conventionally fractionated radiotherapy protocol (3/18) it was 2748 days. There was no statistically significant difference between them (P = 0.843).
When comparing the two protocols in patients that underwent multiple surgical excisions before initiation of the radiotherapy (8/18 cats), the median PFI for the patients treated with a hypofractionated radiotherapy protocol (2/8) was 164 days, whereas for the patients treated with a conventionally fractionated radiotherapy protocol (6/8) it was not reached. A comparison between the two protocols was not possible due to the small sample sizes in these groups of cats.
MC (<9 vs ⩾9), grade of the tumour, number of surgical procedures (single vs multiple) before initiation of adjuvant radiotherapy and the time between the last surgery and initiation of radiotherapy (<4 weeks vs >4 weeks) independently of adjuvant treatment chosen were evaluated for prognostic significance. There was no statistically significant difference noted (Table 7). In three cases the MC was not reported and in three cases the grade of the tumour was not reported by the pathologist. In addition, there was one patient where the date of recurrence was unknown and was therefore censored from the data. Therefore, 14/18 cats were included in the evaluation of prognostic significance for MC and grade of the tumour and 17/18 cats for number of surgical procedures before initiation of radiotherapy and the time between the last surgery and initiation of radiotherapy.
Evaluation of variables with potential prognostic significance for progression-free interval (PFI) independently of adjuvant radiotherapy treatment protocol chosen

MC = mitotic count
At the time of our retrospective analysis, five (27.8%) cats were euthanased: two due to tumour recurrence; two due to unrelated causes; and one for an unknown reason. In the follow-up period, only one cat was documented with distant metastatic disease (pulmonary metastasis). The cat had multiple surgeries before initiation of the adjuvant conventionally fractionated radiotherapy protocol. The tumour was classified as low grade.
Discussion
The epidemiology, pathogenesis, characterisation and recommendations for treatment and prevention of FISSs have been extensively researched; however, this information is lacking for nFISSs. It is too often assumed that tumour behaviour in cats is similar to that seen in their canine counterparts; thus, tumours are often managed similarly to what is recommended for canine patients. To date, there are no large studies reporting the efficacy of surgery with adjuvant radiotherapy in nFISSs in cats.
Several prognostic and predictive factors have been considered in a clinical setting for canine STSs. MC, histological grading and completeness of surgical margins are thought to be the most valuable and they were therefore assessed in our population of cats. 2
High MC, independent of grade, is associated with recurrence, reduced tumour-free interval, metastases and reduced survival time in canine STSs and a cut-off of 9 mitotic figures per 10 hpf has shown to be prognostically significant in the canine population.25,30,35 MC (<9 vs ⩾9) was therefore evaluated in our population of cats for prognostic significance; however, no statistically significant difference was observed (P = 0.936). This may be due to our small sample size or may be an indication that MC is not prognostically significant for nFISS. In addition, the area in which the mitotic figures were counted was not specified. The specification of the final magnification (×400) does not adequately define the area of cells counted as it also depends on the field number (FN) on the ocular. The standard area for reporting is 2.37 mm2 (40 × objective and 10 × ocular with a FN 22 mm) and the two most common FNs are 20 and 22. The difference in area with these two oculars is not great (17%), but if the FN in one ocular was 18 and another was 26.5, for example, the difference is approximately 47%. Obviously, the impact on MC would be large and possibly affect the cases with MC close to our cut-off of 9 of being grouped wrongly, which could influence the prognostic significance. 36 Furthermore, there is no standardisation regarding the area of the tumour to be evaluated for MC, which could introduce further bias. A second review of the histology for the patients would have been beneficial for this study, but due to the long time period over which patients were evaluated, this was unfortunately not possible.When applying the canine grading system in the present study, 8/15 (53.3%) were classified as low-grade, 4/15 (26.7%) as intermediate-grade and 3/15 (20%) as high-grade tumours in cases where the grade was assigned. This is in accordance with canine STSs, where low-grade tumours predominate and represent 51–84%, and high-grade tumours are uncommon when assessing the tumours diagnosed at primary care practices; however, in studies assessing the grade of STSs managed at referral practices, high-grade, tumours appear to be more common (22.7–29%). 37 Grade has proven to be a useful prognostic indicator, especially in terms of predicting recurrence and for indicating concern for metastasis in canine patients. 2 Therefore, the grade of the tumour was assessed for prognostic significance in our population. No statistically significant difference was observed when comparing low-grade with intermediate- and high-grade tumours (P = 0.760). This grading system has not been validated in cats and hence these data should be interpreted with caution when prognosticating for feline patients. It would be interesting to assess if there would be a difference in our results if these cats were graded based on the newly proposed grading system for feline STSs. 14
Tumour location may affect resectability and ability to achieve complete excision. The majority of the tumours in the present study were located on the extremities (94.4%), and only one cat had the tumour located on the head, which most likely led to tumour cells extending to the margins of the submitted samples in most cases (15/18). Extremities were also the most frequent location of nFISS in the study by Aberdein et al (37.5%), where the tumours appeared on the head in 25% of cats. 5 Doddy et al, on the other hand, reported the most frequent location of nFISSs to be the head (50.3%) and the tumours in that study were located on the limbs in 21.3% of cats. 16 Selection bias may have contributed to the high numbers of tumours being located on the extremities, in particular on the distal aspect, in order to ensure only true nFISSs were included. In canine STS, studies describe trends suggesting that localisation to the limbs may be prognostic for longer survival, lower metastasis and better response to treatment; however, there are several studies that did not identify the differences based on location.2,35,38
The goal of STS treatment is to achieve local disease control. The principal treatment in the management of canine STSs is therefore surgical excision, but radiotherapy also plays an important role in local tumour control, especially for incompletely resected and unresectable STSs. Incomplete surgical margins were reported in the majority of cats in this study (15/18) and extrapolating from canine patients, high risk of local recurrence would be expected.
Overall, dogs treated with radiotherapy following incomplete surgical excision of STSs have a good prognosis. 25 In two published studies, the reported local recurrence rate was 18% 26 and 21% 28 following adjuvant hypofractionated radiotherapy; in four other studies, the recurrence rate was similar following conventional fractionated radiotherapy at 17–20% with reported median times to local recurrence of 213 days, 700 days, 798 days and 2631 days.25,27,29,30 Direct comparison between studies, however, is impossible due to the number of different variables: number of surgeries before initiation of radiotherapy; radiotherapy protocol used; different grades of the tumours; and adjuvant treatments used (eg, chemotherapy). All the studies also lack a control group.
In the present study, the overall local recurrence rate was 44.4% (8/18 cats). A total of 37.5% (3/8 cats) had recurrence following a hypofractionated protocol and 50% (5/10 cats) following a conventionally fractionated protocol, which is higher than what is reported for canine STSs treated with surgery and adjuvant radiotherapy. This might be due to the high number of cases with incomplete surgical margins in our study. Also, no other adjuvant therapy (eg, chemotherapy) was used in any of our cases in comparison with canine studies, which may have contributed to delaying progression time in dogs.25,30 The exact localisation of the recurrences was also not specified in our clinical records (eg, within the radiotherapy field, at the borders, outside the radiotherapy field), which would be helpful to identify potential cases of geographical miss.
When comparing the hypofractionated and conventionally fractionated radiotherapy protocols, no statistically significant difference was observed in median PFI between them (P = 0.636). This may be due to the small number of cases; however, differences in group characteristics may have a role as well. In the hypofractionated group, 75% of the cats (6/8) had only one surgery before initiation of radiotherapy, as opposed to only 30% of cats (3/10) that had one surgery before initiation of radiotherapy in the conventionally fractionated group. Concurrently, all the high-grade tumours reported in the study were treated with a conventionally fractionated protocol. Studies in cats with FISS have shown that cats that underwent multiple surgeries before initiation of radiotherapy had significantly shorter overall PFI and were therefore more difficult to treat than first-occurrence tumours.7,39,40 It has been theorised that the reason for this is because the cumulative trauma from multiple surgeries may lead to increased tumour hypoxia and other favourable microenvironmental parameters known to confer resistance to irradiation and which may lead to treatment failure. 41
Interestingly, in the study by Rossi et al, evaluating adjuvant radiotherapy in FISS, the cats with primarily occurring FISS appeared to benefit most from postoperative conventionally fractionated radiotherapy. The same benefit was not evident in cats that underwent multiple surgeries and they concluded that a hypofractionated protocol would therefore be more appropriate for these patients. 40 In the current study, there was no statistical difference in median PFI for the cats that had only one surgery before initiation of radiotherapy when comparing the two protocols (P = 0.843). Owing to the small number of cases, comparison between the cats treated with multiple surgeries before initiation of either the hypofractionated or conventionally fractionated protocols was not possible. A larger population of cats with nFISSs would need to be evaluated in order to evaluate if there are differences in the response to different radiotherapy protocols between the two subpopulations of feline STSs. This would be helpful information, particularly when treating older patients or patients with a high risk of anaesthesia-related morbidity. If the tumour control outcome is similar, then a shorter treatment course may be more suitable for this type of patient. However, this should be balanced against the increased risk of late complications due to large fraction dose size and high BED3 in hypofractionated protocols, which is more important in a young patient that might live long enough with a good prognosis for long-term control.
The impact of time between surgery and initiation of adjuvant radiotherapy on patient outcome has been evaluated in a few FISS studies. Cohen et al showed that the disease-free interval decreased as the time between the surgery and radiotherapy increased; however, Rossi et al failed to show this correlation.7,40 In the current study, no statistically significant difference was noted in cats when the time between the surgery and radiotherapy was <4 weeks vs >4 weeks, independently of adjuvant treatment chosen (P = 0.289).
The radiation protocols were also assessed based on the concept of BED. BED is a way to compare the biological effect of different radiation protocols on normal cells and tumour cells, which helps compare the risks of side effects as well as probability of tumour control. It is calculated from the number of fractions, the dose per fraction and the alpha/beta ratio (α/β) of the tissue in question (BED = nd[1+d/(α/β)], where n is the number of fractions, d is the fraction size and α/β is a constant). Early responding tissues comprising cells that are radiosensitive will typically have a high α/β ratio compared with more radioresistant late responding cells and tissues. In general, a high α/β ratio is assigned when comparing either acute effects or tumour response of two different protocols. In contrast, an α/β ratio of less than 4 (most often 2 or 3) is assigned when comparing the potential risk of late effects between protocols. Although radioresponses of normal cells are more likely to be similar from one individual to another, the radioresponses of tumour cells vary significantly from one tumour type to the other. Because of variability of radiosensitivities between tumours, as well as, to a lesser degree, between individuals, this is a very simplistic approach and far from accurate. Unfortunately, α/β ratios are difficult to determine, and it requires a very timely process in the laboratory. Therefore, these are not readily available for each individual tumour type and definitely not for each individual tumour. We therefore often need to extrapolate from the literature should we choose to reach for a more accurate comparison. Unfortunately, there are no estimates available for neither feline nor canine STSs in the literature. In one recent study evaluating radiosensitivity in various human STS cell lines, the median α/β ratio was 4.9. 42 We chose to assign an α/β ratio of 4.9 and 10 as well, to calculate the BED of the four radiation therapy protocols administered to our cats to compare the potential effectiveness of each protocol on tumour control. Then BED was calculated using an α/β ratio of 3 to compare the potential late side effect risk of each protocol. The results can be found in Table 5. Looking at our results in Table 5, the BED values suggest that protocol 4 × 9 Gy is just as effective on tumour control as protocol 18 × 3 Gy when using an α/β ratio of 10 (BED values of 68.4 vs 70.2, respectively), but slightly more effective on tumour control than 18 × 3 Gy when using a more realistic α/β ratio of 4.9 (BED values of 102.1 vs 87.1, respectively). Should our patients survive long enough, protocol 4 × 9 Gy holds a significantly higher risk of late tissue complications compared with the 18 × 3 Gy (BED values of 144 vs 108, respectively). When deciding on the most appropriate treatment option, both the chances of successful tumour control and the risk of tissue complication needs to be taken into account. For the treatment of STSs in dogs, protocols with a BED4.9 of 87–97 Gy (eg, 18 × 3 Gy and 20 × 3 Gy protocols) have resulted in a relatively good success rate at achieving tumour control. Further studies are required to establish the appropriate BED for nFISS and a future challenge would be to find a successful protocol at the appropriate BED for nFISS that also has a lower BED3 value to minimise complication risk. Perhaps adding an additional adjuvant therapy might also be necessary to achieve this goal.
The acute adverse effects of radiotherapy were reported to be mild and self-limiting in the majority of cats. The incidence of reported late toxicity in this study was also very low. This might be surprising given the high dose per fraction (9 Gy) used in 5/8 patients treated with a hypofractionated radiotherapy protocol and, therefore, high BED3. This is most likely a result of the retrospective nature of the study and loss to follow-up in many of the cats. Of the cats treated with a hypofractionated protocol, 50% were lost to follow-up/died within 18 months following initiation of radiation therapy. Since late side effects may not occur for many years after treatment, a follow-up time of 18 months may not have been sufficient time for late effects to have developed.
Metastatic disease was not evident in any cat that was staged before radiotherapy, and subsequently reported in only one cat in this study. Lung metastases was diagnosed 240 days after initiation of the radiotherapy, which was 902 days since the tumour was initially noted. Interestingly, the tumour was evaluated as low grade by the pathologist, and the cat was treated with a conventionally fractionated protocol.
The low number of cases due to the rarity of this tumour type in cats and loss to follow-up in many of the cats in the study restricted us from drawing further conclusions from this study. For this reason, the survival data in this study were not reported and local recurrence of the tumour was used as the primary outcome measurement. Confidence intervals due to low case numbers were therefore not reported either. A further important limitation of this study is that the radiotherapy protocols were not standardised due to the retrospective nature of the study. The histopathology samples were reviewed by different pathologists, making the comparison among the histopathology reports impossible. There were three reports where the grade of the tumour was not assigned and in three reports the MC was not reported. One report did not have either grade or MC reported. Also, not all cats had thoracic imaging performed before initiation of radiotherapy and post-treatment monitoring was not established; therefore, the prevalence of metastasis may be higher. Finally, we acknowledge that there are no gold standard guidelines for definitive differentiation between injection site and non-injection-site STS in cats; however, very stringent criteria were used in order to exclude the potential cases of injection site sarcoma from the study.
Conclusions
The study suggests that local tumour control could be more challenging in nFISS in comparison with STS in dogs since the recurrence rate is much higher than that reported in canine literature. However, this study demonstrates that adjunctive radiotherapy did result in good long-term tumour control in 12/18 cats. Further studies in larger populations are required to assess the significance of radiation dose and fractionation on tumour control and the effect of multiple surgeries before initiation of radiotherapy on outcome.
Footnotes
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognised high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed and/or this work involved the use of cadavers. Ethical approval from a committee was therefore not specifically required for publication in JFMS. Although not required, where ethical approval was still obtained, it is stated in the manuscript.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (experimental or non-experimental animals, including cadavers) for all procedure(s) undertaken (prospective or retrospective studies). No animals or people are identifiable within this publication, and therefore additional informed consent for publication was not required.