
Abstract
The present research investigated the relationship between self-respect (i.e., a person’s belief of possessing the same rights as others) and depressive symptoms. Based on earlier longitudinal findings that self-respect fosters assertiveness and that assertiveness negatively predicts depressive symptoms, we tested these relationships in Western and non-Western countries. Additionally, we explored associations with suicidal ideation. Across seven countries (N = 2408) we found that self-respect and depressive symptoms were negatively correlated. In addition, we found evidence for an indirect path via assertiveness as well as negative correlations with suicidal ideation in countries with available measures. Finally, within-manuscript meta-analyses confirmed the main path between self-respect and depressive symptoms across all seven countries. This research presents the first evidence for the negative association between self-respect (feeling equal to others) and depressive symptoms and highlights new directions for linking self and self-regard to mental health.
Introduction
Depression is a common mental illness worldwide. According to the World Health Organization, in 2015 approximately 322 million people—4.4% of the world population—suffered from depression (World Health Organization, 2017). With a reported lifetime prevalence of up to 20% internationally (Kessler and Bromet, 2013), it is clear that depression and symptoms of depression constitute a worldwide burden for societies. Depressive episodes are accompanied by experiences of depressed mood (feeling sad or empty) and/or a loss of pleasure or interest in activities over a longer time period. Depressive symptoms also go along with feelings of excessive guilt and/or low self-worth and thoughts about death or suicide. Both the number of depressed individuals and the number of suicide attempts have increased worldwide in past years, beginning before the Covid-19 pandemic (Naghavi, 2019; World Health Organization, 2021). In 2019, an estimated 703,000 people died by suicide and the global age-standardized suicide rate was 9.0 per 100,000 people (World Health Organization, 2021).
Moreover, depression is responsible for a number of additional costs and disadvantages for individuals and societies. For example, depression negatively affects educational (Fletcher, 2010) and labor market outcomes of affected individuals (Lerner and Henke, 2008), and increases healthcare utilization and costs (Boer et al., 1997). Depression is negatively related to household income and the probability of being married (Smith and Smith, 2010). In conclusion, depression represents a burden for individuals and societies from both a psycho-social and economic perspective. The aim of the present research is to identify novel protective factors against depression, focusing on individuals’ self-respect.
The Role of individuals’ self-view in depressive symptoms
Deficits in a person’s self-view are a defining element of depression. The ICD-10 definition states “self-esteem and self-confidence are almost always reduced and, even in the mild form, some ideas of guilt or worthlessness are often present” (https://icd.who.int/browse10/2019/en#F33). Researchers have started recognizing the importance of focusing on people’s self-views for fully understanding depression. In line with this, research shows that global self-esteem (Rosenberg, 1965) is negatively related to depressive symptoms (Orth et al., 2009; Wouters et al., 2013). Although these findings are consistent across studies and have been validated longitudinally and within meta-analyses (Sowislo and Orth, 2013), some researchers have questioned whether global self-esteem is a useful concept in psychological research, especially with regard to its value for interventions. For example, in a review, Baumeister et al. (2003) did not find any evidence that boosting self-esteem (e.g., by therapeutic interventions or school programs) led to the predicted benefits for mental health. In our opinion, this is due to the global nature of the conceptualization and measures of self-esteem (for a similar argument see Baumeister et al., 2005). More specifically, within the global self-esteem concept, perceived self-competence and self-love/self-liking are intermingled, and aspects of perceived self-equality are mostly neglected. However, it is precisely this concept of perceived equality of the self that might be particularly relevant for depression and that we focus on in the present research.
Self-respect and its origin
Past research has largely focused on the global self-esteem concept, which is often operationalized with the Rosenberg scale (e.g., Orth et al., 2018; Pegler et al., 2019; Twenge and Campbell, 2002). Recent research shows, however, that global self-esteem contains three distinguishable subdimensions: self-liking/self-confidence, self-competence (Tafarodi and Swann, 1995, 2001), and self-equality (see Renger, 2018). This means that self-evaluations of being likable, competent, and equal are usually averaged (by building global self-esteem means) and cannot be investigated separately. In this research, we focus on the third aspect, namely self-equality, i.e., a person’s belief in possessing equal rights and dignity; a facet of people’s self-view that has mostly been overlooked until now (Renger, 2018; Renger et al., 2020). This self-view has been referred to as self-respect (Darwall, 1977; Honneth, 1995). Seeing the self as possessing the same rights as others is different from seeing the self as competent or likable. Self-respect is also different from self-efficacy. Whereas self-respect describes an individual’s sense of having the right (i.e., being allowed) to do or say something, self-efficacy relates to a person’s conviction of being able to do or say something (Bandura, 1977).
These differences between the different forms of self-regard become clearer when looking into the origins of these concepts. Researchers agree that self-confidence/self-liking are formed by need-based care, love, and affection (e.g., Bowlby, 1983, 2005), for example through parental or peer support and acceptance (Gabriel et al., 2008; Tafarodi and Swann, 1995; Tafarodi et al., 2010; Wilkinson and Parry, 2004). Self-competence and self-efficacy are shaped through performance feedback, praise, and achievement-based social esteem (Honneth, 1995, 2012) and can be decreased for adolescents by parents who are psychologically controlling (Salafia et al., 2009). Self-equality/self-respect is formed by the treatment of others as an equal counterpart who is respected and taken seriously. 1 The latter process can be hindered through discrimination or social injustice. More specifically, a broad range of research shows that people from disadvantaged groups (e.g., people of colour, women, older people, sexual minorities, people with disabilities, etc.) are often not recognized as equals, experience more unequal treatment (e.g., Augoustinos and Reynolds, 2001; Brooks, 2019; Sisselman-Borgia et al., 2021; Sue et al., 2007; Peterman, 2018), and often show a diminished sense of perceived entitlement to equal treatment (Jost, 1997; Major, 1994; Möller and Danermark, 2007; Presbey, 2003). In addition, social injustices regarding, for example, socioeconomic status create unequal opportunities with regard to educational resources (e.g., Paulus et al., 2021), as well as, voting availability (e.g., Peterman, 2018). Recent research also demonstrated that people with disabilities receive less equality-based respect experiences in the public domain and in turn show a lower level of self-respect compared to people without disabilities (Martiny et al.,). In summary, we argue that internalized equality (i.e., self-respect) is a self-evaluation that can be distinguished from other self-evaluations previously discussed in the literature and that it has independent origins.
Self-respect and depressive symptoms
Self-respect as an internalization of one’s own equality allows the individual to perceive the self as possessing the same rights as others and therefore owning an equal space in society and in the world. We therefore argue that self-respect can affect the development of depressive symptoms (1) directly and (2) indirectly via assertiveness. Related to the first aspect, high self-respect ensures that individuals ascribe an equal importance to their rights as to others’ rights. In other words, individuals who do not perceive themselves as having the same right to their own (independent) space as others are not able to perceive and set boundaries that signal to others that they must not cross a certain line. If individuals blur the lines between their own and others’ spaces it is more difficult to decide where their and others’ rights and duties start and end. As a consequence, people with low self-respect are more likely to care more about others’ concerns than their own (Helgeson and Fritz, 1998; Renger, 2018). As a result, overinvolvement in others’ problems, self-neglect, and externalized self-evaluation can follow (Fritz and Helgeson, 1998; Helgeson and Fritz, 1998). These consequences often lay the foundation for depression (Aubé et al., 2000; Jin et al., 2010).
The assumption that self-respect and depressive symptoms are related is also supported by findings that members of minorities, such as sexual or ethnic minorities, suffer from depression more often than members of majority groups (e.g., Lewis, 2009; Przedworski et al., 2015; Valentine and Shipherd, 2018). As described above, members of these minority groups are more likely to experience discrimination and have a reduced sense of entitlement (e.g., Major, 1994; Möller and Danermark, 2007; Presbey, 2003), which may explain the association between self-respect and depression.
Related to the second aspect, high self-respect enables individuals to assertively protest if others inappropriately invade their space (Renger et al., 2020). This relationship between self-respect and assertiveness was confirmed both correlatively and longitudinally (Renger, 2018; Renger et al., 2020). Previous research also showed that the link between self-respect and assertiveness is robust even when controlling for other self-evaluations such as self-liking, self-competence, global self-esteem, and psychological entitlement (Renger, 2018, Study 2). In fact, to our knowledge, no prior research has found a relationship between concepts like global self-esteem, self-liking, or self-competence and assertiveness (for an overview see Renger, 2018), highlighting the unique relationship between self-respect and assertiveness. Moreover, a connection between not assertively expressing thoughts and feelings (“silencing the self”) and depression has been demonstrated across cultures (Jack and Ali, 2010). A lack of self-assertive behavior was associated with an increased risk for the occurrence of depression across time (Ball et al., 1994), and has also been discussed as a central element in the development and treatment of depression (Speed et al., 2018). In the present research, we bring together these paths linking self-respect with assertiveness on the one hand, and assertiveness and depressive symptoms on the other, by testing the mediating role of assertiveness and investigating the hypothesized paths across different countries.
Depressive symptoms and suicidal ideation
Major depressive disorder (MDD), and also mild or moderate depressive symptoms, increase the likelihood of suicidal ideation and suicide attempts especially during the depressive episodes (Cukrowicz et al., 2011; Riihimäki et al., 2013). A meta-analysis of 166 longitudinal studies confirmed that depressive symptoms, including subclinical ones, predict suicidality across all age groups (Ribeiro et al., 2018). One particular correlate of depression, low self-esteem, has been found to increase the likelihood for suicidal ideation (Bhar et al., 2008; Overholser et al., 1995; Wild et al., 2004; but see also Yao et al. [2014], who found correlations between high self-esteem and suicidal ideation). As discussed above, self-respect represents a previously neglected form of self-evaluation that has not yet been studied separately. The feeling of not having the same rights as others and the associated perception of not having a separate or own “space” in life might also be relevant for suicidal ideation. We test this direct link exploratorily. However, the primary effect is expected to be mediated via depressive symptoms.
The present research
Although most countries around the world have signed the Universal Declaration of Human Rights, differences in legal or lived rights can be found between countries, for example with regard to equal rights for women and men (e.g., Alikarami, 2019; Freeman, 2022; Tohidi, 2016). As a consequence, it is likely that differences in the absolute levels of internalized equality (i.e., self-respect) exist. More specifically, in Western, as compared with non-Western countries, equal rights and equal treatment are a reality for a greater number of people (World Economic Forum, 2019). However, the mere existence of equal rights does not guarantee that people will be treated accordingly. Only to the extent that people are treated as equal individuals by others can they internalize this in their self-image and this psychological process should be the same across countries. In the present research we thus were mainly interested in the correlations between self-respect and depressive symptoms, assertiveness, and suicidal ideation irrespective of (differences in) absolute values. We argue that the associations should be the same across different countries as these relationships represent basic psychological processes. We were thus not interested in cultural differences but in similarities and therefore the generalizability of the proposed relationships across countries.
In Study 1, we collected data in three European countries (Germany, Norway, and Spain) to test whether self-respect and depressive symptoms are negatively correlated. In Study 2, we expanded our investigation to non-European countries (Iran, South Korea, and Indonesia) and included additional measures of assertiveness and suicidal ideation. We hypothesized a direct path between self-respect and depressiveness and additionally an indirect path via assertiveness. In addition, we explored the link between self-respect and suicidal ideation and potential indirect paths via assertiveness and depressiveness. In Study 3, we sought to replicate our findings using different measures of assertiveness, depressive symptoms, and suicidal ideation in an English-speaking country (United Kingdom). Finally, we tested the overall significance for the hypothesized paths across all seven countries using within-manuscript meta-analyses. Ethical approval for Studies 1 and 2 was obtained from the first author’s university ethics committee; for Study 3 it was obtained from [University of Glasgow], the former university of the second author. Materials for all studies are provided in the Supplemental Material, and data and analysis script are available at OSF (https://osf.io/aecs3/).
Study 1
The aim of Study 1 was to test the correlation between self-respect and depressive symptoms in three European countries. WHO depression prevalence estimates for Germany (5.2%), Norway (4.7%), and Spain (5.2%) are rather high compared to other countries’ rates worldwide, with the lowest around 2.9% and highest around 6.3% (World Health Organization, 2017). Despite differences in prevalence, we predicted that the association between self-respect and depressive symptoms would be the same in terms of direction (i.e., negative) and magnitude in all countries.
Method
Participants
Participants were invited to participate in an online questionnaire in German, Norwegian, or Spanish and had to be at least 18 years old to participate. We recruited participants from multiple online platforms and social networks, such as Facebook, and email distribution lists at psychology and sociology departments at different universities. The questionnaire was completed by 448 participants (148 in Germany, 177 in Norway, and 123 in Spain). Parts of the data from the Norwegian sample were used in another article that investigated associations between stigma and self-respect (Martiny et al.). Participants were able to participate in a lottery for vouchers with a total value of around 150 Euro per country. We excluded 12 participants (6 from Germany, 3 from Norway, and 3 from Spain) who failed more than one of the three attention checks 2 or indicated on a dichotomous item at the end that they had not answered the survey seriously. Mean age of the remaining 436 participants was 33.0 years (SD = 14.19 years; range 18–77 years). There were 317 women and 113 men (6 other). For education level and occupation see Supplemental Material (Appendix A).
Measures
Self-respect
Self-respect was measured with Renger’s (2018) four-item self-respect scale (e.g., “In everyday life I always see myself as a person with equal rights”). Responses to the four items were provided on 7-point Likert scales ranging from 1 (not true at all) to 7 (completely true). The measure was translated into the three languages (Norwegian, German and Spanish) and checked by at least two native speakers in each country.
Depressive symptoms
To assess depressive symptoms, we used the 10-item version of the CES-D (Center for Epidemiologic Studies–Depression) scale, which was designed for use as a depression screening tool in the general population (Grzywacz et al., 2006; Kohout et al., 1993). Participants indicated how they felt during the last week (e.g., “During the last week, I felt depressed”) on 7-point Likert scales ranging from 1 (seldom or never) to 7 (most of the time or always). We used validated translations of the scale for the German (see Riediger et al., 1998), Norwegian (see Clausen and Slagsvold, 2005) and Spanish (see González-Forteza et al., 2011) questionnaires.
Demographics
At the end of the questionnaire, participants were asked to indicate their gender, age, education level, and occupation.
Results
Means, standard deviations, bivariate correlations, and Cronbach’s alpha for all measures in Study 1 (Germany, Spain, and Norway).

Note. If not indicated otherwise N was 430. Gender was coded one for male and two for female (6 non-binary persons were not included). Education was coded 0 for low education and one for high education. The depressive symptoms scale only included the six items that were used in the CFAs and SEMs. The correlation between self-respect and the depressive symptoms scale with all 10 items was similar in sign, magnitude, and significance. Cronbach’s alpha is provided in the diagonal.
*p < .05, **p < .01, ***p < .001.

SEM for the relationship between self-respect (SR) and depressive symptoms (DS). Standardized factor loadings and regression weights are shown (p-value is two-tailed). Note. *p < .05, **p < .01, ***p < .001.
The results from the three European countries showed that self-respect was significantly and negatively related to depressive symptoms even when controlling for age and gender. A model with fixed regression weights equally fit the data as a model with unconstrained regression weights, indicating that the relationship did not significantly vary between countries.
Study 2
In Study 2, we expanded our investigation to non-European, non-Western countries (Iran, South Korea, and Indonesia). In order to investigate mediating relationships, we included measures of assertiveness and in South Korea and Indonesia also suicidal ideation. Depression prevalence for these countries is officially lower than for the European countries (Iran: 4.9%; South Korea: 4.1%, Indonesia: 3.7%). Regarding suicide rates, WHO estimates from 2019 rank South Korea 4th worldwide with 28.6 cases per 100,000 inhabitants, whereas Indonesia scores much lower with 2.4 cases (World Health Organization, 2021).
Although the appropriateness and the absolute values of assertive behaviour vary between cultures (Bresnahan et al., 2002), the negative relationship between assertiveness and depressiveness has also been found in Iran (Rezayat and Dehghan Nayeri, 2014), South Korea (Jung, 2014), and Indonesia (Fuspita et al., 2018). This means that people who behave assertively are more likely to show less depressive symptoms, shown here also in non-Western countries. We thus tested assertiveness as a mediator between self-respect and depressive symptoms. In addition, we explored whether self-respect was linked to suicidal ideation, either directly (exploratory hypothesis) or via depressive symptoms. As noted above, the latter path might also be mediated via assertiveness, but we did not have a hypothesis regarding the path from assertiveness to suicidal ideation.
Method
Participants
Participants were invited to participate in an online questionnaire in Farsi, Korean, or Indonesian and had to be at least 18 years old to participate. Participants were invited via social media platforms (in Iran only via Instagram) and personal email contacts from native speakers who grew up in the respective countries. The questionnaire was completed by 1815 participants (1533 in Iran, 119 in South Korea, and 163 in Indonesia). In South Korea and Indonesia participants were able to participate in a lottery for gift cards or cash worth 100 Euro each. We excluded 15 participants (2 from South Korea, 13 from Indonesia) who failed more than one attention check2 or indicated at the end that they did not answer seriously (these checks could not be included in the Iranian questionnaire). Mean age of the remaining 1800 participants was 31.2 years (SD = 8.7 years; range 18–74 years). There were 1384 women and 416 men. For education level and occupation see Supplemental Material (Appendix A).
Measures
Self-respect
Self-respect was measured with the same scale as in Study 1. The measure was translated and checked by at least two native speakers in each country.
Depressive symptoms
Depressive symptoms were administered with the same scale as in Study 1. The validity of the CES-D has been demonstrated in various Asian settings, for example Iran (Sharif Nia et al., 2021), Korea, and Indonesia (Mackinnon et al., 1998).
Assertiveness
Assertiveness was assessed using the 8-item Negative Assertion Subscale (NAS) of the Interpersonal Competence Questionnaire (ICQ; Buhrmester et al., 1988), which measures an individual’s ability to assert displeasure with others (e. g., “Saying ‘no’ when an acquaintance asks you to do something you don’t want to do”) on a 7-point Likert scale.
Suicidal ideation
Suicidal ideation was measured with two items of the Suicide Behaviors Questionnaire - Revised (SBQ-R; Osman et al., 2001). Participants in South Korea and Indonesia were asked to respond to the question “How often have you thought about killing yourself in the past year?” on a 7-point Likert scale from 1 (never) to 7 (very often), and “How likely is it that you will attempt suicide someday?” on a 7-point Likert scale from 1 (never) to 7 (very likely). They also had the option to choose the answer “I cannot or do not want to specify” which was treated as a missing value (rSpearman-Brown = 0.79 [South Korea], rSpearman-Brown = 0.79 [Indonesia]).
Demographics
At the end of the questionnaire, participants were asked to indicate their gender, age, education level, and occupation.
Results
Means, standard deviations, bivariate correlations, and Cronbach’s alpha for all measures in Study 2 (Iran, South Korea, and Indonesia).

Note. If not indicated otherwise N was 1800. Gender was coded one for male and two for female. Education was coded 0 for low education and one for high education. The suicidal ideation scale was not administered in Iran. The depressive symptoms scale only included the six items that were used in the CFAs and SEMs. The correlations with the depressive symptoms scale with all 10 items were similar in sign, magnitude, and significance. Cronbach’s alpha is provided in the diagonal.
*p < .05, **p < .01, ***p < .001.

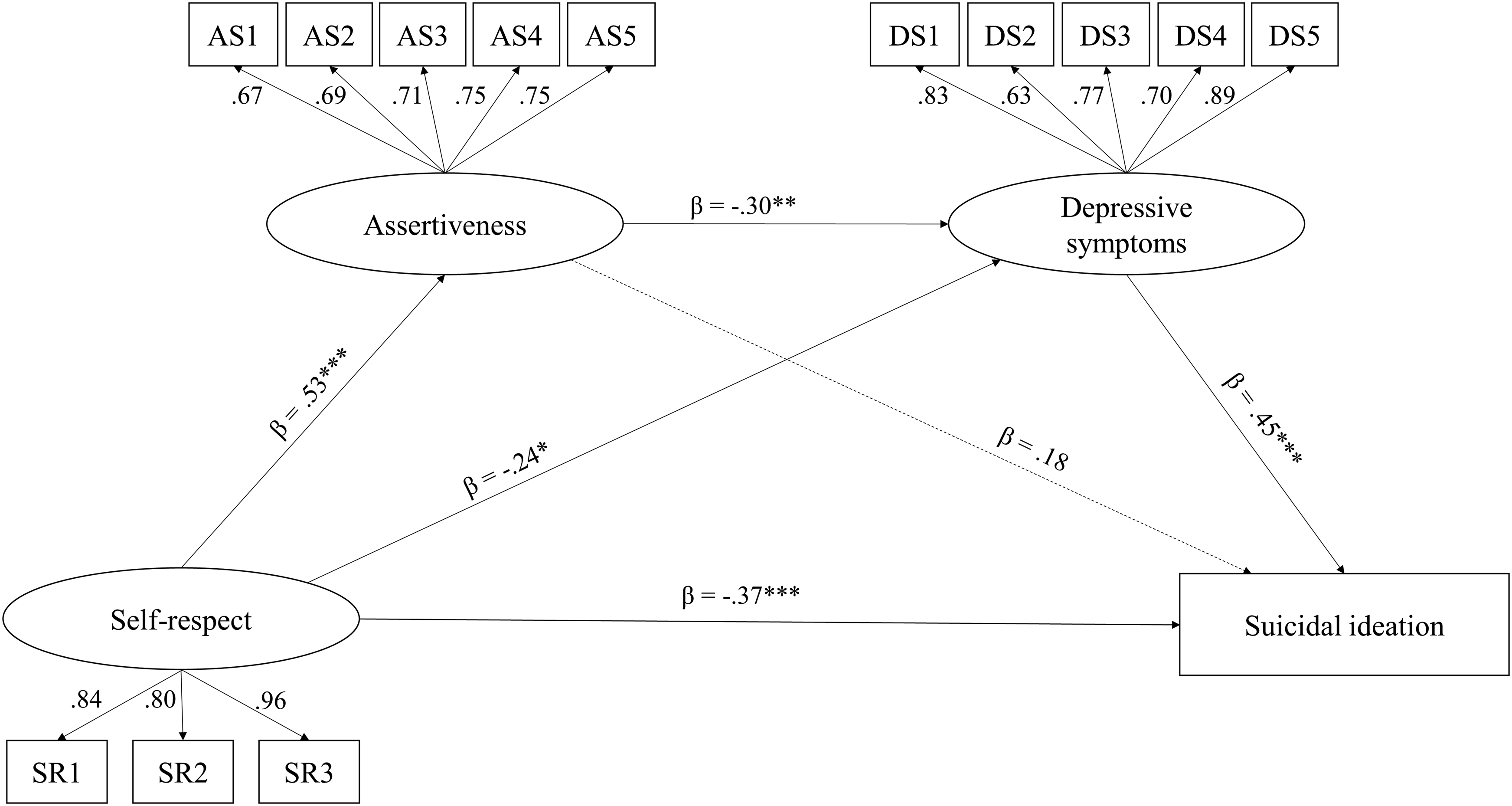
SEM for the relationship between self-respect (SR), assertiveness (AS), and depressive symptoms (DS) across three countries (Iran, South Korea, Indonesia). Ranges for standardized factor loadings and regression weights are shown (p-values are two-tailed). Note. *p < .05, **p < .01, ***p < .001.
In South Korea and Indonesia, we additionally included a measure of suicidal ideation. Self-respect was negatively correlated with suicidal ideation (r = −0.23, p < .001). CFA showed that for self-respect, assertiveness, depressive symptoms, and suicidal ideation, a four-factor solution showed a significantly better fit (CFI = 0.95, TLI = 0.94, RMSEA = 0.04, SRMR = 0.06) than a one-, two-, or three-factor solution (CFIs ≤ 0.92, TLI ≤ 0.91, RMSEA ≥ 0.04, SRMR ≥ 0.07). We also tested for measurement invariance (see Appendix D). There was a statistically significant difference between the scalar and metric model (Δχ2 = 26.313, Δdf = 16, p = .050), indicating weak factorial invariance (constrained loadings; CFI = 1.00, TLI = 1.03, RMSEA = 0.00, SRMR = 0.07). SEM-multiple group analyses showed that the paths between self-respect and assertiveness, between self-respect and depressive symptoms, and between depressive symptoms and suicidal ideation were significant across countries (see Figure 3), and that the path weights did not differ significantly between countries (Δχ2 = 10.579, Δdf = 6, p = .102; CFI = 0.94, TLI = 0.93, RMSEA = 0.04, SRMR = 0.08). These effects remained stable when controlling for age and gender. SEM for the relationship between self-respect (SR), assertiveness (AS), depressive symptoms (DS), and suicidal ideation (SI) across two countries (South Korea, Indonesia). Ranges for standardized factor loadings and regression weights are shown (p-values are two-tailed). Note. *p < .05, **p < .01, ***p < .001.
Next, we tested the indirect effects of self-respect on suicidal ideation via assertiveness and/or depressiveness. The indirect effect via depressiveness was significant (β = –0.18; 95%-CI = [–0.29; –0.08], z = –3.43, p < .001) whereas the effects via assertiveness (β = –0.00; 95%-CI = [–0.08; 0.06], z = –0.26, p = .79) and via assertiveness and depressiveness (β = –0.02; 95%-CI = [–0.06; 0.01], z = –1.23, p = .22) were not.
Study 3
The aim of Study 3 was to replicate the observed relationships using different measures of assertiveness and depressive symptoms to generalize the observed effects across different measures. This study was run in the United Kingdom and focused on students, a population that has been found to show high prevalence of depression and suicidal ideation (Akram et al., 2019; Eskin et al., 2016). By focusing on students, we minimize age as a confounding factor (see positive correlations of self-respect with age in Studies 1 and 2). A student sample, therefore, represents a conservative test of our model.
Method
Participants
Participants were recruited via email, social networks, and posters on the campus of [University of Glasgow] university and invited to a study about health and everyday life on campus and had to be at least 18 years old. The Royal Conservatoire of Scotland’s LGBTQ + society and the university’s Equality and Diversity Unit promoted the study on their respective social media channels. One hundred and seventy two participants completed the survey. There were 148 women and 24 men (Mage = 21.6 years, SD = 2.9 years, range 18–42 years), with 83 identified as heterosexual and 89 as non-heterosexual.
Measures
Self-respect
Self-respect was assessed with the same scale as in Studies 1 and 2. The self-respect measure had previously been validated in an English-speaking sample (α = 0.89; Renger, 2018, Study 3).
Assertiveness
Assertion of one’s personal rights was measured using the 8-item Negative Assertion Subscale (NAS) of the Interpersonal Competence Questionnaire-Revised (ICQ-R; Buhrmester, 2002; e.g., “How good are you at voicing your desires and opinions?”) on a 5-point Likert scale ranging from 1 (poor at this) to 5 (extremely good at this).
Depressive symptoms
Depressive symptoms were assessed using the 7-item depression subscale of the Depression, Anxiety and Stress Scales (DASS-21; Lovibond and Lovibond, 1995; e.g., “I felt down-hearted and blue”) on a 4-point Likert scale from 0 (did not apply to me at all), 1 (applied to me to some degree or some of the time), 2 (applied to me to a considerable degree or a good part of the time) to 3 (applied to me very much or most of the time).
Suicidal ideation
Suicidal ideation was assessed with the suicidal ideation scale (Osman et al., 2001). Due to different scale labels and anchors these items could not be averaged. In our analyses we thus focused on the item used in Study 2 (“How often have you thought about killing yourself in the past year?”) on a 5-point scale with 1 (never), 2 (rarely/1 time), 3 (sometimes/2 times), 4 (often/3–4 times), 5 (very often/5 or more times).
Demographics
Age, gender, and sexual orientation (heterosexual vs non-heterosexual, e.g., lesbian, gay, bisexual, pansexual, or asexual) were assessed at the beginning of the questionnaire.
Results and discussion
Means, standard deviations, bivariate correlations, and Cronbach’s alpha for all measures in Study 3 (UK).

Note. N was 172. Gender was coded 0 for male and one for female. Sexual orientation was coded 0 for non-heterosexual and one for heterosexual. The scales only included the items that were used in the CFAs and SEMs. Cronbach’s alpha is provided in the diagonal.
*p < .05, **p < .01, ***p < .001.
SEM for the relationship between self-respect (SR), assertiveness (AS), depressive symptoms (DS), and suicidal ideation (SI) in the UK. Standardized factor loadings and regression weights are shown (p-values are two-tailed). Note. *p < .05, **p < .01, ***p < .001.
In addition, the following indirect effects were significant: Self-respect → Assertiveness → Depressive symptoms (β = –0.16; 95%-CI = [–0.27; –0.05], z = –2.80, p < .01), Self-respect → Depressive symptoms → Suicidal ideation (β = –0.11; 95%-CI = [–0.20; –0.01], z = –2.17, p < .05), Assertiveness → Depressive symptoms → Suicidal ideation (β = –0.13; 95%-CI = [–0.24; –0.03], z = –2.46, p < .05), and Self-respect → Assertiveness → Depressive symptoms → Suicidal ideation (β = –0.07; 95%-CI = [–0.13; –0.01], z = –2.38, p < .05).
Our results from Study 3 confirmed the paths found in Study 2 between self-respect, assertiveness, depressive symptoms, and suicidal ideation using different measures and an English-speaking sample. In addition, we again found indirect effects, suggesting that the relationship between self-respect and depressive symptoms is in part explained by assertiveness. Further, the relationship between self-respect and suicidal ideation was in part explained by a path through assertiveness and depressive symptoms. Interestingly, the path between self-respect and suicidal ideation was still significant even when controlling for the other possible paths.
Within-manuscript meta-analyses
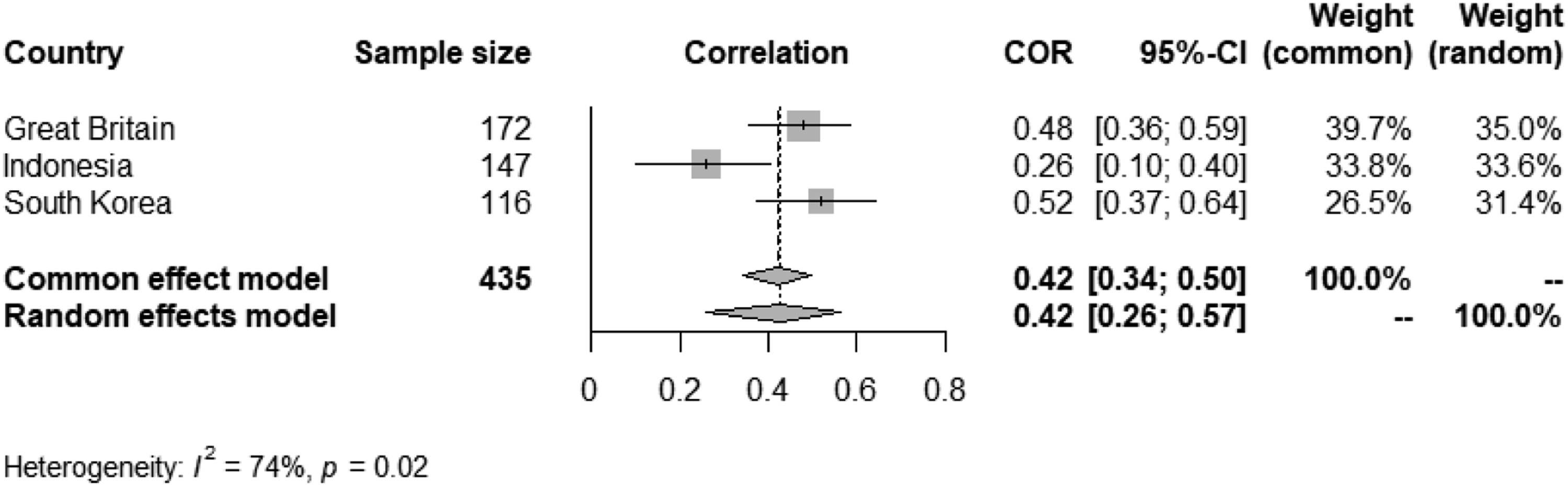
To estimate whether the relationships observed in different countries hold overall, we conducted several within-manuscript meta-analyses based on bivariate correlations and sample sizes (using the meta package in R with restricted maximum-likelihood as estimator). The I2 heterogeneity statistic is the percentage of variability in the effect sizes that is not caused by sampling error (a I2 above 25% is considered low heterogeneity, a I2 above 50% as moderate heterogeneity, and a I2 above 75% as substantial heterogeneity; see Higgins and Thompson, 2002; Higgins et al., 2003). Because we detected at least some between-study heterogeneity and because it is conventional to use a random effects model, we not only calculated the fixed or common effect model but also the random effects model (Harrer et al., 2021). Combining data from all seven countries, we found significant meta-analytic relationships with moderate heterogeneity between self-respect and depressive symptoms (all seven countries, see Figure 5), between self-respect and assertiveness (four countries, see Figure 6) and between self-respect and suicidal ideation (three countries, see Figure 7).
4
In addition, significant meta-analytic relationships were found for the paths between assertiveness and depressive symptoms (see Figure 8) and depressive symptoms and suicidal ideation (see Figure 9), both indicating moderate heterogeneity. Forest plot for the relationship between self-respect and depressive symptoms based on bivariate correlations and sample sizes. Note. correlation = observed study effect size (hatch mark), study weight (grey square), and study confidence interval (horizontal line); diamond = pooled effect of the common effect model and pooled effect of the random effects model; Solid vertical line = the point on the x-axis equal to no effect; COR = bivariate correlation; 95%-CI = 95% confidence interval; weight (common/random) = Weight of the effect size; I2 = heterogeneity statistic and p-value. Within-manuscript meta-analysis for the relationship between self-respect and assertiveness based on bivariate correlations and sample sizes. Note. correlation = observed study effect size (hatch mark), study weight (grey square), and study confidence interval (horizontal line); diamond = pooled effect of the common effect model and pooled effect of the random effects model; solid vertical line = the point on the x-axis equal to no effect; COR = bivariate correlation; 95%-CI = 95% confidence interval; weight (common/random) = weight of the effect size; I2 = heterogeneity statistic and p-value. Within-manuscript meta-analysis for the relationship between self-respect and suicidal ideation based on bivariate correlations and sample sizes. Note. correlation = observed study effect size (hatch mark), study weight (grey square), and study confidence interval (horizontal line); diamond = pooled effect of the common effect model and pooled effect of the random effects model; solid vertical line = indicates the point on the x-axis equal to no effect; COR = bivariate correlation; 95%-CI = 95% confidence interval; weight (common/random) = weight of the effect size; I2 = heterogeneity statistic and p-value. Within-manuscript meta-analysis for the relationship between assertiveness and depressive symptoms based on bivariate correlations and sample sizes. Note. correlation = observed study effect size (hatch mark), study weight (grey square), and study confidence interval (horizontal line); diamond = pooled effect of the common effect model and pooled effect of the random effects model; solid vertical line = indicates the point on the x-axis equal to no effect; COR = bivariate correlation; 95%-CI = 95% confidence interval; weight (common/random) = weight of the effect size; I2 = heterogeneity statistic and p-value. Within-manuscript meta-analysis for the relationship between depressive symptoms and suicidal ideation based on bivariate correlations and sample sizes. Note. correlation = observed study effect size (hatch mark), study weight (grey square), and study confidence interval (horizontal line); diamond = pooled effect of the common effect model and pooled effect of the random effects model; solid vertical line = indicates the point on the x-axis equal to no effect; COR = bivariate correlation; 95%-CI = 95% confidence interval; weight (common/random) = weight of the effect size; I2 = heterogeneity statistic and p-value.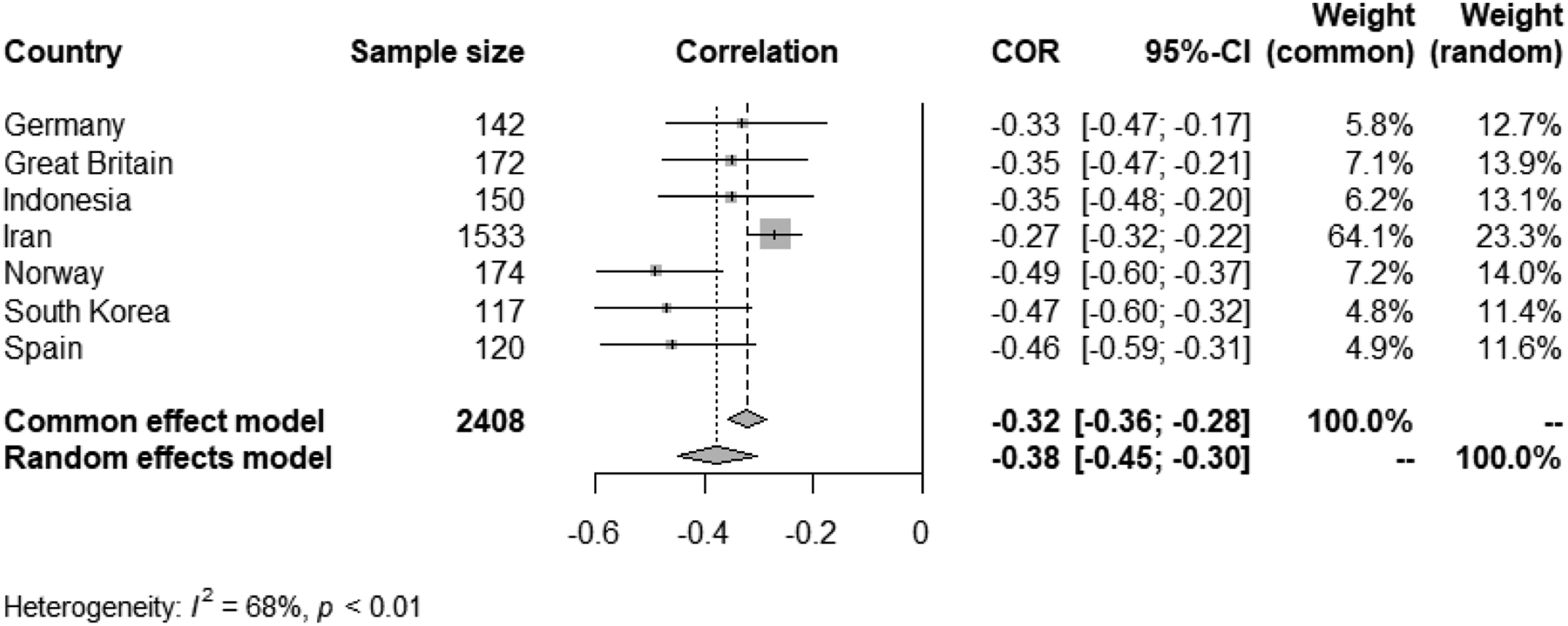



As indicated in Footnote 3, there seems to be some variation between countries for the path between self-respect and suicidal ideation (see Figure 7). In fact, the path models show that whereas the direct path was significant in the UK sample, it was not significant in the South Korean and Indonesian sample. Bivariate correlations between self-respect and suicidal ideation were, however, significant in all three countries. Further research is needed to explore the role of feeling equal to others in suicidal ideation.
Discussion
Even if people live in a country where they are equal before the law, it does not necessarily mean that everyone has internalized this equality to the same degree. Self-respect is not about having or knowing, but about believing in one’s own rights (Feinberg, 1980) and is therefore a self-evaluation that might vary between individuals in Western and non-Western countries (cf. World Economic Forum, 2019). In the present research, we investigated the health correlates of self-respect across different countries. More specifically, we tested associations between self-respect, assertiveness, depressive symptoms, and suicidal ideation in samples from seven different countries (Germany, Norway, Spain, Iran, South Korea, Indonesia, and the UK). We found support for all hypothesized paths and meta-analyses across all samples confirmed their significance (for each criterion variable data from at least three countries was available). As our central hypotheses predicted, self-respect was negatively related to depressive symptoms and also to suicidal ideation.
Results from the non-Western countries (see Figure 2) as well as from a student sample in the United Kingdom (see Figure 4) also pointed to a potential mediating role of assertiveness and depressive symptoms. While this mediating relationship needs further attention in future research, results clearly confirmed direct negative associations of self-respect with depressive symptoms and further with suicidal ideation (i.e., not mediated via assertiveness).
Overall, the relationship between self-respect and the mental health outcome variables was weaker in some of the non-Western countries. Western and non-Western countries often differ in equality norms and levels of democracy but it would be too speculative to name this as the cause of the differences found. Instead, we think that the consistency of the relationships across countries (with varying strength) provides robust evidence for our hypotheses. This means that even in countries where equality is by no means granted for everyone, as soon as individuals have the possiblity to internalize their own equality (i.e., have high self-respect), they behave more assertively, show fewer symptoms of depressiveness, and report fewer suicidal ideation.
Considering self-respect as third self-dimension
Our research shows that the internalization of not owning an equal space and equal rights (i.e., low self-respect) is associated with depressive symptoms and suicidal ideation. This association supports self-respect as a third distinct factor of people’s self-evaluation, in addition to self-liking and self-competence (the main components of global self-esteem; Tafarodi and Swann, 2001). This tripartition allows for a more differentiated perspective on human self-evaluation and on distinct sources and antecedents: whereas self-love/self-liking is nourished through need-based care (Bowlby, 1983, 2005) and interpersonal love and affection, self-competence is facilitated through achievement-based social esteem (e.g., praise) (e.g., Salafia et al., 2009). Self-respect is fostered through experiences of equality-based respect, that is, being taken seriously and as a person of equal worth (Honneth, 1995; Möller and Danermark, 2007; Presbey, 2003; Renger, 2018).
The importance of respect experiences as an antecedent of self-respect is especially pronounced in minority contexts. A broad range of research has shown that people from disadvantaged groups (e. g., people of color, women, older people, sexual minorities, people of low SES, people with disabilities) are often not treated with equality-based respect (Augoustinos and Reynolds, 2001; Sue et al., 2007) and often show a diminished sense of perceived entitlement to equal treatment (Renger et al.,; Jost, 1997; Major, 1994). In line with this, in the present research, we observed a correlation between self-respect and gender (Study 1), meaning that women indicated lower levels of perceived self-equality. In addition, in Study 3, students who indicated being non-heterosexual showed lower levels of self-respect compared with heterosexual students. In light of the fact that members of disadvantaged groups suffer more often from depression and suicidality (Haslam et al., 2019; Lewis, 2009; Marshal et al., 2011; Missinne and Bracke, 2012; Przedworski et al., 2015; Smith et al., 2020; Valentine and Shipherd, 2018), our findings strongly suggest that it might be worthwhile to take a closer look at self-respect and its role in mental health.
Limitations and strengths
Although our sample was relatively heterogeneous regarding several sociodemographic variables, the present samples are not representative for the respective countries (e.g., regarding gender distribution). Our focus was rather to empirically test a theoretically derived model while controlling for possible confounding variables as well as sociodemographic variables (cf. Brewer, 2000). Future research should replicate the findings with representative samples.
In the current studies, we were able to demonstrate metric invariance across countries (see Supplemental Material, Appendix D). Metric invariance does not allow for comparison of means across countries but it means that factor loadings in the measurement part in each cultural group are identical which is considered as sufficient for the interpretation of latent variables in path analyses (see e.g., He and Van de Vijver, 2012). In the present studies, we excluded some items from scales because CFAs indicated low factor loadings (e.g., for the depression scale, see Study 1). Two of these items (8 and 10) have also been excluded in prior research (e.g., in the European Social Survey; Van de Velde et al., 2010). Although we think that the remaining items capture the core of the respective concepts, future research is needed to confirm the validity of the shortened scales.
The current research was based on correlational data and causal relations should thus be interpreted with caution. It is important to note, however, that the main paths of our model had been previously supported in longitudinal studies. It has been demonstrated that self-respect predicts assertiveness over time (Renger, 2018), assertiveness leads to lower levels of depressive symptoms (Ball et al., 1994; Jack and Ali, 2010), and depressive symptoms increase the likelihood for suicidal ideation (Ribeiro et al., 2018). The novelty of the present research lies in comparing the relative strengths of these established paths across different countries, and it draws attention to self-respect as an important correlate of depressive symptoms in both Western and non-Western countries. In fact, both causal directions that could be implied from the observed correlations are interesting in themselves: if low self-respect in fact causes depressive symptoms, then prevention programs and health care policies should be adapted to foster respect experiences and self-respect as buffers and resilience factors. If, on the other hand, low self-respect stems from depressive symptoms, then therapies and interventions should incorporate self-reflection regarding people’s internalized equality.
New Avenues for Treatment and Intervention: Fostering Self-Respect as a Specific Component of One’s Self-Evaluation
Deficits in one’s self-view are a defining element of depression. Past research has shown that interventions to improve self-esteem are often not successful (Baumeister et al., 2003, 2005). One possible reason may be that global self-esteem is very broad and mainly concerned with generally feeling good about the self (Rosenberg, 1965). It could therefore be worthwhile to focus on specific subdimensions of people’s self-evaluations. Based on the current findings, we suggest focusing on self-respect, as this cognitive component may be easier to change than more emotional subdimensions. A positive correlation between age and self-respect in Studies 1 and 2 supports the idea that change in this subdimension of one’s self-view is possible.
Interventions and therapy could specifically focus on the link between perceptions of not having equal rights and entitlements with depressive symptoms. This could for example include a focus on cognitive manifestations (e.g., thoughts of inferiority or inadequateness, self-blame and self-criticism, or indecisiveness), motivational manifestations (e.g., paralysis of the will or increased dependency) and delusions (e.g., convictions of worthlessness that nearly 50% of depressed persons suffer from) associated with depression (Beck and Alford, 2009).
Our research shows that lower self-respect is not only negatively related to depressive symptoms, but also to thoughts about suicide. Suicidal thoughts are usually strongly characterized or even predicted by thoughts about worthlessness, a reduced sense of the right to live (Bolton et al., 2008; Goodwill, 2021), or the feeling of not perceiving one's own space and feeling trapped (Kidd, 2004). The common theme of perceived worthlessness and lack of seeing an (equal) space for oneself could help inform future interventions and prevention programs for preventing depression and suicide. In addition, the path via assertiveness could also be used to design fruitful interventions (Speed et al., 2018). Fostering self-respect will likely affect assertiveness; a link that has, so far, not been shown for global self-esteem or any of its subdimensions (Baumeister et al., 2003; Renger, 2018).
It is promising that assertiveness induced via (self-)respect is limited to socially appropriate non-aggressive forms of assertiveness and protest (Renger, 2018; Renger et al., 2020), because seeing the self as an equal implies seeing others as equals as well. This dual role of considering own and others’ rights simultaneously could foster a balance between an egoistic focus on the self and an overly altruistic focus on others, which is beneficial for mental health in general.
Supplemental Material
Supplemental Material - Why the belief in one’s equal rights matters: Self-respect, depressive symptoms, and suicidal ideation in Western and non-Western countries
Supplemental Material for Why the belief in one’s equal rights matters: Self-respect, depressive symptoms, and suicidal ideation in western and non-western countries by Daniela Renger, Aischa Reinken, Sabrina Krys, Maria Gardani and Sarah E Martiny in Health Psychology Open.
Footnotes
Acknowledgements
We thank Damra Aksoy, Jonas Josten, Alba Henares, Firman Tambunan, Dejan Živanović for the help with collecting data and Elizabeth J. Parks-Stamm for her valuable feedback on the manuscript. We acknowledge financial support by DFG within the funding programme Open Access-Publikationskosten.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We acknowledge financial support by DFG within the funding programme Open Access-Publikationskosten.
Supplemental Material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.