
Abstract
This study described the prevalence of suicidal behaviors and depression among adolescents in Hanoi, Vietnam, and examines the associated factors. In 2019, a school-based survey was conducted in three high schools in Hanoi and 661 high students were included into the study. We found that the prevalence of 12-month suicidal thoughts, suicide plans, and suicide attempts were 14.2%, 5.5%, and 3.0% respectively. Notably, the depression score mean was 16.1±4.9, among major predictors of suicidal ideation. Therefore, developing psychological care services in school is imperative to the early detection of mental disorders and the prevention of suicidal behaviors for the students.
Keywords
Background
Suicide, defined as the act of deliberately killing oneself (World Health Organization (WHO), 2020), is emerging as a priority in global public health, particularly for adolescents and young adults (Fleischmann and De Leo, 2014). Based on current trends, the World Health Organization (WHO) estimates that in 2020, there will be approximately 1.53 million individuals worldwide who will die of suicide, with 10–20 times this number in suicide attempts worldwide (Bertolote and Fleischmann, 2015). Globally, suicide was ranked as the second leading cause of premature mortality among individuals aged 15–29 years and the third leading cause among those 15–44 years old (Bertolote and Fleischmann, 2015). Suicidal behavior includes suicidal ideation (frequent thoughts of ending one’s life) and suicide attempts (the actual event of trying to kill one’s self) (Garfunkel et al., 2007), with suicidal attempt being the strongest predictor of successful suicide (O’Connor et al., 2013). Suicide attempts in particular are an important risk factor; those with a history of suicide attempts have 50–100 times higher risk of dying by suicide than those without such history (Shain, 2007).
Previous studies have explored the prevalence and determinants of adolescent suicidal behaviors. Risk factors for suicidality are best understood using an ecological model. At the individual level, females with a current or past history of alcohol abuse, smoking and mental disorders were more likely to conduct suicide attempts (Bertolote and Fleischmann, 2015; Bertolote et al., 2010; Oppong Asante et al., 2017). At the interpersonal level, a current or past history of being bullied, exposure to violence, and poor relationships with family and school (Kokkevi et al., 2012; Mueller et al., 2015) were described as associative factors. While suicidal behaviors have been well-studied in high income countries, there is a smaller evidence base from low- and middle-income countries (LMICs), where 75% of all suicides occur (World Health Organization (WHO), 2014). This is partly attributed to the lack of surveillance systems to monitor adolescent health and health behaviors, such as the Youth Risk Behavior Surveillance System (YRBSS) in the USA (Brener et al., 2004) and the Health Behavior in School-aged Children Study in Europe (Currie et al., 2009).
Depression, another common mental disorder among adolescents worldwide, is defined as a state of low mood and aversion to activity, with an estimated 1-year prevalence in 4%–5% mid- to late- adolescents (Costello et al., 2005; De Zwart et al., 2019). According to Gledhill et al, it was estimated as one of the major predictors of suicidal behavior among children and adolescents (Gledhill and Hodes, 2008). In order to support this view, a study of students from Tehran University also showed that depression had the most contribution, along with anxiety, mental health, resiliency, and daily stresses in predicting suicidal ideations (Izadinia et al., 2010). This is also true in the opposite direction, a longitudinal study among German students illustrates that positive mental health seems to confer resilience and moderate the impact of depression on suicide ideation; in those students who reported higher levels of positive mental health, depression severity showed no association with suicide ideation over time (Teismann et al., 2018).
Vietnam is a low and middle income country (LMIC), despite adolescents playing a pivotal role in economic development and accounting for nearly 10% population of the country, the country does not routinely conduct either school or community-based surveillance to monitor adolescent health and risk behaviors (PopulationPyramid.net, 2019). Vietnam has had two national surveys, in 2005 and 2010, specifically targeting the health of young people (Survey Assessment of Vietnamese Youth—SAVY I and II) (Vietnam UNFPA, 2015). SAVY I and II reported the percentage of suicidal ideation increased significantly for adolescents in just five years, from 3.4% in 2005 to 4.1% in 2010. Besides producing a national report, Vietnam also conducted a school-based student health survey (GSHS), in 2013, that included in a GSHS of Association of Southeast Asian Nations (ASEAN) member states (2007–2013). The results showed that the highest prevalence of suicidal ideation was in the Philippines (17.0%) and Vietnam (16.9%) (Peltzer and Pengpid, 2017). In 2012, a cross-sectional study of 1247 students conducted in 3 countries—China, Thailand, and Vietnam—showed that the 12-month prevalence of suicidal ideation was highest in Vietnam (Kay et al., 2012). To our best knowledge, despite the high and increasing prevalence of suicidal behaviors among adolescents, research into the risk factors that correlate with suicidal behaviors, especially depression has been extremely limited in comparison to other countries. Therefore, this study was conducted with the aim of describing the prevalence of suicide behaviors and depression, and factors associated with them among high school students in Hanoi, Vietnam.
Methods
Participants
Study setting and participants
This study was conducted from August to September 2019 in Cau Giay District—an urban district located in the West of Hanoi, the capital city of Vietnam. It is one of the most rapidly developing urban districts in Ha Noi, with a young population structure as well as high rate of successful secondary school completion and university entrance exam results from high school students (Cau Giay District Information Portal, 2020). Three chosen high schools included the following: Cau Giay High School (CG), Yen Hoa High School (YH) and Nguyen Binh Khiem High School (NBK). The first two schools are public schools, and the other is private. Study design, sample size, and sampling
The multi-stage cluster sampling techniques was employed. (1) Schools were randomly chosen from a list of 13 high schools in the Cau Giay district. (2) In these schools, two classes were randomly picked from a list to represent each grade, from grade 10–12, and a total of 6 classes per school were included in the study. (3) For each class, all students were involved in the study. We selected students based on the following criteria: student agreed to be involved in the study and having the permission from parents (5% were refused). All the eligible students were clearly explained the study objectives. If they agreed to participate in the study, they were asked to provide written, informed consent from their parents to confirm their participation. In total, 661 high-school students (15–19 years old) from the 3 previously mentioned high schools were included in this study.
Procedures
Measures and instrument
Two questionnaires were used, these are the Youth Risk Behavior Surveillance (YRBS) (Felts et al., 1996) and Modified Depression Scale (MDS) (Dunn et al., 2012).
The Youth Risk Behavior System Surveillance (YRBSS) is a systematic, epidemiologic, surveillance system prepared by the Center for Disease Control and Prevention (CDC) for the purpose of monitoring youth risk behaviors (Baheiraei et al., 2012). The questionnaire for YRBS includes six categories of behaviors: (1) unintentional injuries and violence; (2) tobacco use; (3) alcohol and other drug use; (4) sexual behaviours; (5) dietary behaviors; and (6) physical activity (Brener et al., 2002).
Modified Depression Scale (MDS) was used in this study for the purpose of measuring depressive symptomatology within the past 30 days (Dahlberg, 2005), which inquiries about the frequency of six symptoms of depression including: sadness, irritability, hopelessness, sleep disturbance, difficulty concentrating, and eating problems with five-point response scale: (1) never, (2) rarely, (3) sometimes, (4) often, and (5) always.
All dependent and independent variables was presented in Appendix 1.
Data collection
The questionnaire was designed via a website Kobotoolbox (https://ee.kobotoolbox.org/x/#pN9QBSEE). Students answered the questionnaire after accessing the Kobotoolbox link by tablet. Each student was offered a tablet to answer the questionnaire by themselves after listening to the questionnaire explanation from the data collector team. The answer sheets are automatically aggregated on Kobotoolbox’s website at the end of the investigation.
Data analysis
Both descriptive and analytical statistics were carried out using Stata 15 software (Stata Corporation). P-value lower than 0.05 was considered as a statistically significant. ANOVA and Chi-square tests were used to assess the existence of relationships between our outcomes and demographic characteristics; the prevalence of health-related behaviors and exposures; and accessibility to mental health support methods across three schools. Due to the multilevel characteristics of the dataset that the students were nested in classes and schools, we performed the three-level random intercept logistic and linear mixed model to examine the effects of individual-level, class level and school level to suicide ideation and depression.
Ethical consideration
The protocol of this study was approved by the Institute Review Board, Hanoi University of Public Health. Students were only surveyed after parent permission was received. All students in the study were asked for their consent before collecting data, and all had the right to withdraw from the study at any time without any threats or disadvantages.
Results
Sociodemographic characteristics and health-related behaviors
Regarding the sociodemographic characteristics of students, 46% of total respondents were male, 42.4% were female, while 6.1% of participants were bisexual and 4.4% did not know about their sex orientation. The vast majority of participants belonged to the Kinh ethnicity (98.9%), which is the largest ethnicity in Vietnam. Most students described themselves as non-religious (80.5%). The number of students was divided relatively equally across grade levels (nearly 33% in each grade). Regarding health-related behaviors and exposures, over half of students reported ever drinking alcohol (55.5%), while 15.6% of students had smoked cigarettes. Beside drinking alcohol, 10% of respondents reported having been bullied within the previous 12 months, either physically or online (Appendix 2).
Suicidal behavior and depressive symptoms
Table 1 demonstrates the distribution of MDS scores in each of the three schools and in total. Overall, the average depression score across all students was 16.1 (out of 30), with the highest mean MDS score occurring at NBK (p < 0.01). In general, students in NBK and YH more likely to report experiencing depressive symptoms across all MDS items. Notably, over one-fifth of students usually or always felt sad or irritable in the last 30 days (21.0% and 22.9%, respectively) and these figures in NBK were significantly higher than YH and CG (p = 0.05 and p = 0.02 respectively). In terms of eating problems and hopelessness, 19.0% and 18.5% of students often experienced eating problems and feelings of hopelessness about their future respectively. The highest percentage of eating problems and feelings of hopelessness about the future were in NBK High School, but the differences were statistically significant only for the hopelessness variable (p = 0.02). In terms of sleep problems, 23.4% of students reported usually or always having sleep-related difficulties, with statistically significant differences across the three schools (p = 0.03). Finally, in regards to concentration problem, over one-fourth of students reported usually or always experiencing difficulties in concentration
Descriptive statistics for the modified depression scale (MDS) by each item and the total score.
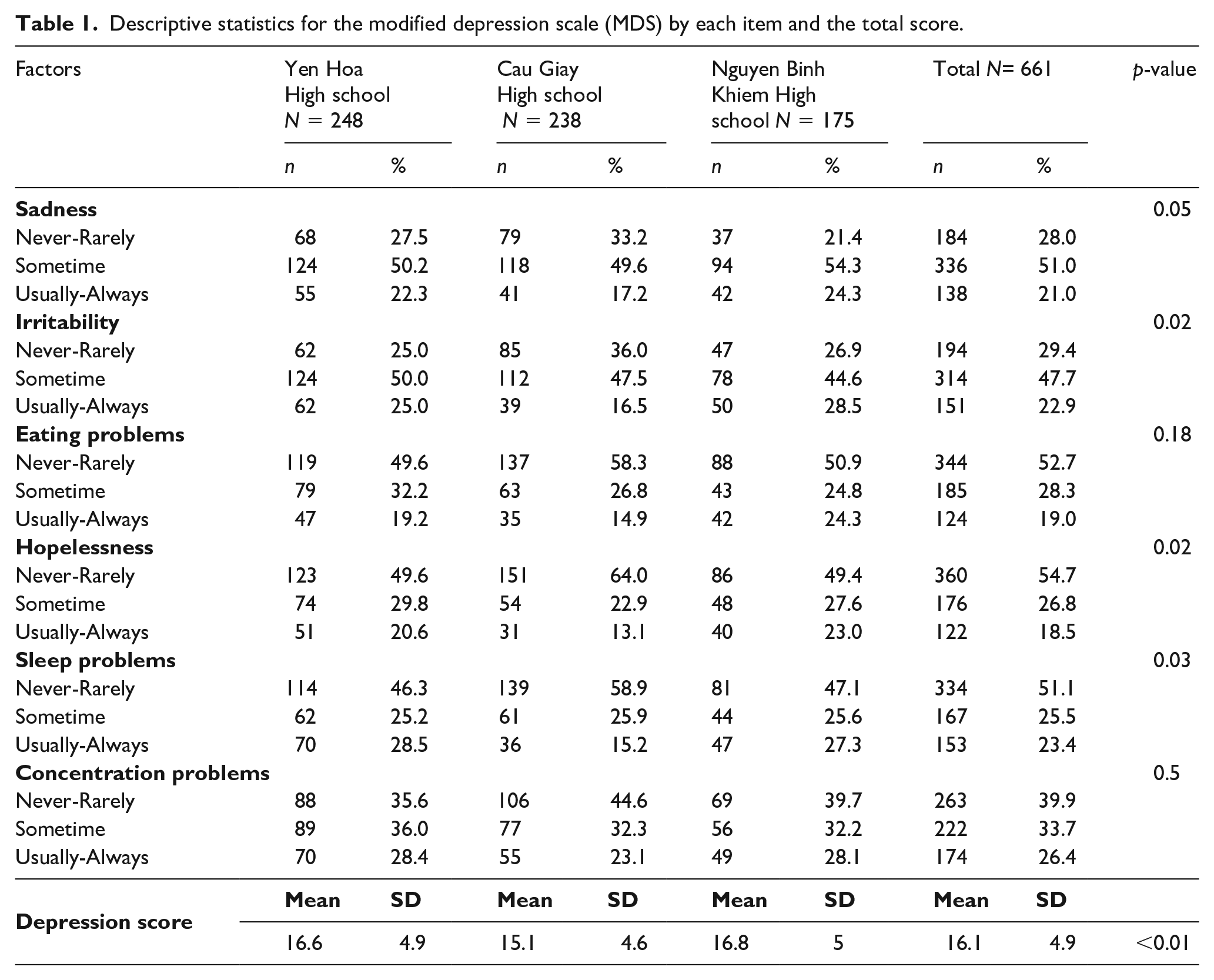
Table 2 shows the 12-month prevalence of suicidal behavior and injury due to suicide attempts and suicide methods of respondents. Of the 661 participants, 94 (14.2%) experienced suicidal ideation, and among these 94 students, 36 (38.3%) had also made a suicide plan and 20 (21.1%) made a suicide attempt. Suicidal ideation, plan and attempts were most common at NBK (16.6%; 41.4%; and 27.6% respectively). Three students—one at each school—had received injuries due to suicide attempts. The most popular method was using sharp objects (9 times) followed by self-immolation (4 times).
12-month prevalence of suicidal thoughts, suicidal plans, and suicide attempts in respondents.

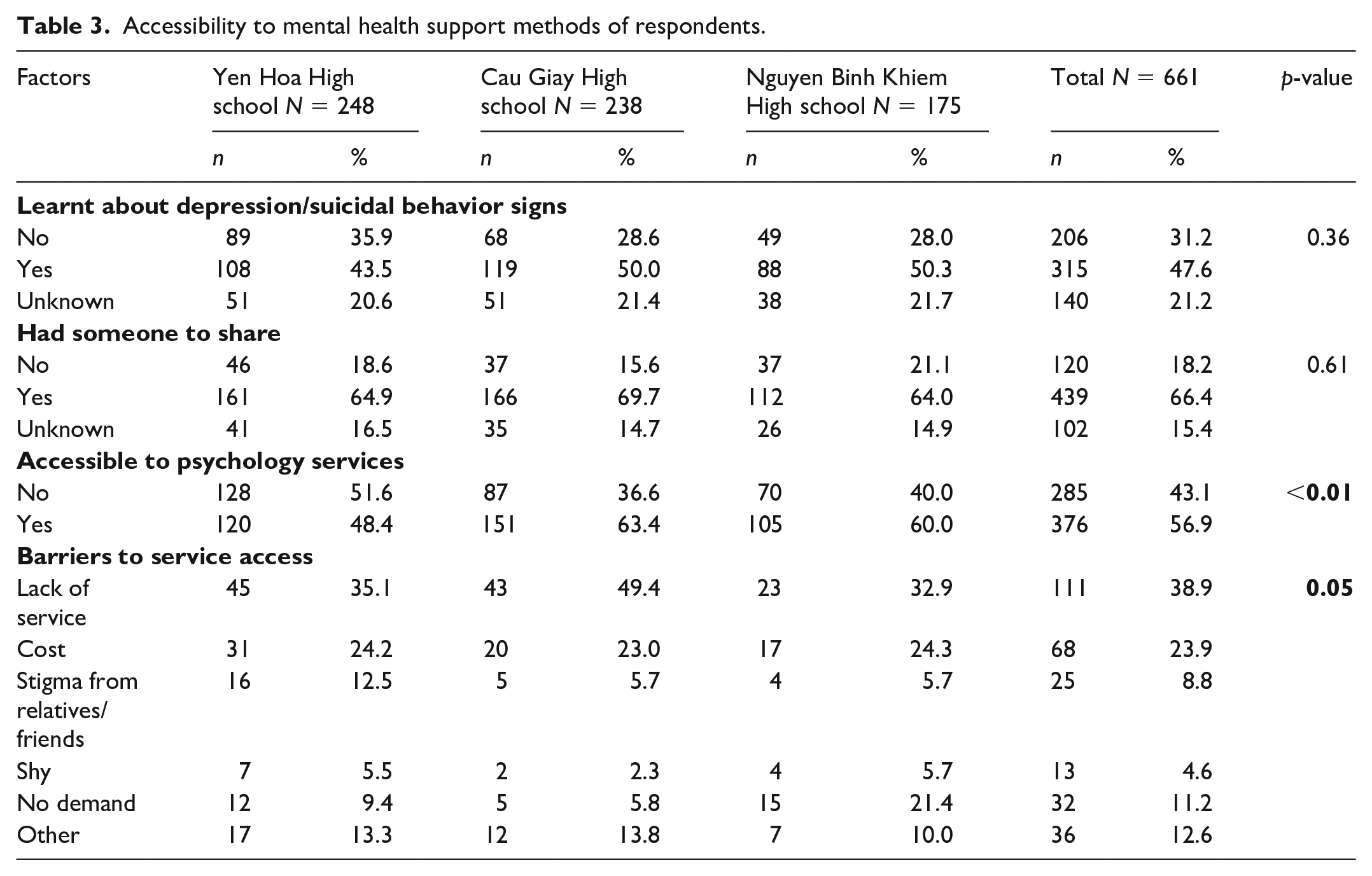
Table 3 shows the level of access to mental health support for students. Over one-third (31.2%) of students reported that they had never been informed about the prevention and treatment of depression and suicidality. Additionally, nearly one-fifth of students described not receiving any supports from friends (18.2%). In terms of accessing psychology services, 43.1% of students said they could not easily access psychological support services, with significantly higher percentage so reporting in Yen Hoa and NBK (p < 0.01). The most common barrier is the shortage of services in the community (38.9%), and financial concerns (23.9%).
Accessibility to mental health support methods of respondents.
A 3-level random intercept logistic and a three-level random intercept linear mixed model was applied to examine the effects of individual, class and school level of suicidal ideation and depression, due to the clustering characteristics of the data. In the null model for suicidal ideation, the intra class correlation (ICC) was negligible while the figure for depression point was 0.01 in school level and 0.05 in class level, which meant the school and class variance accounted for 6% of the total variability in depression point. In the final model (Table 4), when other variables were considered, the variance at the class and school levels still stayed significant but only accounted for 1.6% of the variability in the outcome.
Multilevel analyses the effects of individual and school-level on suicidal ideation and depression among high school students in Hanoi.

p < 0.01, **p < 0.05, *p < 0.1.
: Reference group.
The fixed part of the model shows that depression was strongly associated with suicidal ideation. More specifically, with each one-point increase in depression score, the odds of suicidal ideation increased 1.2 times (p < 0.01). Students who are female, bisexual or unknown gender had higher depression scores than male participants (Coefficient was 1.85 (1.07–2.62), 1.81 (0.3–3.32) and 3.78 (2.05–5.52) respectively)) and were more likely to have suicidal ideation, with statistical significance (OR = 3.81, 95%CI: 1.39–10.45 for unknown gender group). High academic performance was negatively associated with depression (Coef. = −3.8, 95%CI: –6.27; –1.34). Violence was also shown to relate to depression, with 3.18 (1.24–5.11) and 2.39 (0.74–4.04) point increasing in depression point for students who had a high exposure to violence and truancy due to violence. Lastly, easy to access psychology support services could decrease the depression point (Coef. = 1.25, 95% CI: –1.97; –0.53).
Discussion
Main findings
Our results confirm that suicidal behaviors and depression are a common problem among adolescents in Vietnam (Kay et al., 2012; Nguyen et al., 2013). This study found the high 12-month prevalence of suicidal behaviors and depression scores mean among adolescence in Cau Giay district, Hanoi, Vietnam. Consistent with findings from around the world (Bachmann, 2018; Patton, 2014; Swahn and Bossarte, 2007), there were several associative factors with suicidal behavior and depression such as being bisexual and unknown gender, victimization and lack of mental health support. The most common suicide attempt methods for young people in Vietnam were the use of sharp objects, followed by self-immolation, hanging and falling from a height.
Suicidal behaviors
Our study demonstrates that the last 12-month prevalence of suicidal behaviors was 14.2% for suicidal ideation, 5.5% for suicidal plan and 3.0% suicide attempts respectively. These results were in line with the findings from a school-based survey conducted in 32 low- and middle-income countries that the 12-month prevalence of suicidal ideation ranged from 11.7% to 16.7% and suicidal plan range from 5.5% to 8.7% (McKinnon et al., 2016). However, our result is higher than a cross-sectional survey of 17,016 youth aged 15–24 years in 2011 in Hanoi that found less than 1% of young people had attempted suicide and 3.2% of young people had suicidal ideations in their lifetime (Blum et al., 2012). This may be indicate an increasing trend of suicidal behaviors in adolescents when compared with results from Survey Assessment of Vietnamese Youth—SAVY II in 2010 (4.1% young population had suicidal ideations in their life) (General Statistics Office Of Vietnam (GSO), 2020).
There are several reasons that can explain this increasing trend of suicidal behavior among adolescents in Vietnam. First, among social demographic factors, our study found that the LGBT group had suicidal behaviors higher than male and female groups, consistent with a previous study (Almeida et al., 2009). For 10 years, the number of LGBT people, a vulnerable group, has increased in Vietnam. In the local context, although the public awareness about LGBT group has improved in Vietnam during the past 10 years, they still suffers pressure and stress from social stigma (Ha, 2013). The situation can be more prevalent in a high school, because the adolescents at this age are often more sensitive than other students. One study revealed that gay, lesbian, and bisexual adolescents tend to try suicide attempts higher four times than the heterosexual youth (Bagley and Tremblay, 2000). Therefore, high schools in Vietnam should promote communication on gender equality to prevent gender discrimination in school and thereby avoiding suicidal behaviors.
Second, depression was one of the major predictors for suicidal ideation in our study, which was in line with a study of Klomek et al (Klomek et al., 2007). In fact, pressure to achieve high academic performance may be the main culprit of depression in high school students, especially in East Asian cultures (Yadusky-Holahan and Holahan, 1983). One survey conducted in Korea revealed that nearly 34% of Korean adolescents have suicide ideation due to academic pressure (The Korea Herald, 2019). In Vietnam, many parents provide supplementary education to advance their children’s competitive capacity for university entrance exams among high school students (Dang Hai-Anh, 2007). Moreover, the supplementary study associated academic stress, mental health disorders and a high level of depression with suicidal ideations in students in Vietnam (Pham, 2015). Therefore, Vietnamese parents should reduce the pressure on the university entrance exam, and at the same time, arrange supplementary education for their children to help them reduce academic stress.
Finally, in terms of health risk behaviors, this study found that being physically bullied and having frequent exposure to violence are significantly associated with having suicidal thoughts, which was also found among European countries (Centers for Disease Control Prevention, 2014; Kokkevi et al., 2012; National Center for Injury Prevention and Control, 2014). Students who are bullied are often vulnerable, timid and lack confidence, so it is often difficult to integrate or build positive relationships with friends. They may be apprehensive to go to school or to a crowded place. At a severe level, students may have suicidal thoughts or behaviors (Nguyen Thi Thu and Minh, 2013).
Depression score
In Vietnam, our paper is one of the first studies using the MDS tool to examine depression among adolescents, which includes in a Compendium of Assessment Tools of Center of Diseases from the United States (US) (Dahlberg, 2005). In comparison with a previous study using the MDS tool in the US, our findings suggested that the depression score mean was 16.1 (SD = 4.9), a higher result than that of a school-based survey in Boston, Massachusetts (13.3, SE = 0.17) (Dunn et al., 2012).
The high mean of depression scores among adolescents in Vietnam may be due to several reasons. Among demographic variables, LGBT and female students were at a significantly greater risk of depression and this finding is strongly supported by past research (Almeida et al., 2009). The gender difference in depression first emerges at puberty, with studies finding higher prevalence in girls starting at age 11. Furthermore, the hormonal changes that accompany menstruation each month can bring on mood changes similar to those that occur in depression (Havard Medical School, 2020). Vietnam does not have sex education classes in schools, while US students study this during secondary schools. Therefore, female students should be trained on how to deal with hormonal changes and reducing bad mood during menstruation. In addition, we found that average academic performance is a risk factor of depression, while high academic study performance is a protective factor of depression, this is consistent with the finding from a study in Pakistan 2015 (Khurshid et al., 2015). Those who have average academic performance may be under more pressure from their parents than those who have high academic performance, as their parents tend to put less academic pressure on their children.
Among risk behavior variables, being bullied online, truancy and frequent exposure to violence were major predictors of depression. These results are strongly supported by previous studies (Phuong et al., 2013). Bullying and frequent exposure to violence put stress on students, which may make them feel insecure in environments such as school. Consequently, they tend to be truant and isolate themselves from friends, teachers or even family members. Therefore, schools should have stricter rules to reduce the amount of school violence while also organizing more extracurricular activities to strengthen the relationship between students and teachers.
In regards to the accessibility of psychology services, we found that awareness about depression or suicidal behavior signs and being able to access psychology services are protective factors of depression, similar to previous findings (Cuijpers et al., 2016; Fazel et al., 2014; McKinnon et al., 2016). High school students in the US study psychology, including the definition of depression and how to prevent depression and suicidal behaviors in their schools (American Psychological Association (APA), 2020). In our study, one-third of students reported that they had never studied about awareness, prevention and treatment of depression and suicide. Students also reported that they had difficulty accessing mental health support services due to a lack of services and worrying about cost.
The government of Vietnam has taken steps to improve health system responses to depression among adolescent students, the Ministry of Education and Training has also issued guidelines requiring high schools to establish a psychological counseling department (PCD) to provide psychological counseling services to students (Ministry of Education and Traning (MOET), 2020), psychological counseling departments (PCD) in high schools are responsible for psychology counseling and offer programs to improve students’ knowledge of mental health difficulties. Although there are no statistics on the number of PCDs or the effectiveness of PCDs in the education system in Vietnam, several high schools have reported that the members of their PCDs are not psychology counselors, but are teachers (Can Loc High school, 2018–2019).
As a result, PCD members have limited knowledge of psychology and counseling skills needed to provide advice regarding academic issues, reproductive health, relationship problems and career counseling. Therefore, high schools in Vietnam should establish PCDs with staff members requiring a Bachelor of Psychological Counseling, school leader representatives and representatives of parent associations. After establishing PCDs, the PCD should promote communication about signs of depression and suicide, while at the same time, coordinate with the school to organize extracurricular activities for students to reduce academic pressures and strengthen relationships between peers and teachers.
Recommendations
Based on the evidence mentioned above, our study suggests the following recommendations:
For the family level, parents should arrange supplementary education for their children to help them reduce academic stress.
For the school level, schools should firstly increase school safety to reduce bullying rates and organize more extracurricular activities to strengthen the relationship between students and teachers. This will help the school environment become more friendly and embracing with students. Secondly, high schools should establish PCDs with members requiring qualifications in Bachelor of Psychological Counseling, representatives of school leaders and representatives of parent associations in order to promote awareness and communication about depression, suicide, gender equality, sex education and organize free counseling activities for students.
Strength and limitation
This study was subjected to several limitations. First, the study used a self-reported survey. Therefore, there may be an information bias. The survey team tried to minimize students’ misunderstanding by training the data collectors very carefully. The data collectors were present while students completed the questionnaires and were responsible for explaining the questionnaire if needed. Secondly, the data was cross-sectional, which limited our ability to monitor trends in youth risk behaviors.
Apart from these disadvantages, our study has several strengths. Firstly, this current study provides up-to-date evidence on suicidal behavior and depression among adolescents in Vietnam. Secondly, our study recruited students from both private and public high schools. It allowed us to obtain a sample size with diverse sociodemographic backgrounds, increasing the generalizability of the study population.
Footnotes
Appendix
Sociodemographic characteristics related behaviors of respondents.

| Factor | Total N = 661 | |
|---|---|---|
| n | % | |
|
|
||
|
|
||
| Grade 10 | 227 | 34.3% |
| Grade 11 | 220 | 33.3% |
| Grade 12 | 214 | 32.4% |
|
|
||
| Kinh | 654 | 98.9% |
| Others | 7 | 1.1% |
|
|
0.0% | |
| Non-religious | 532 | 80.5% |
| Buddhism | 121 | 18.3% |
| Christian | 6 | 0.9% |
| Others | 2 | 0.3% |
|
|
||
| Bad | 13 | 2.1% |
| Average | 180 | 29.2% |
| Good | 424 | 68.7% |
|
|
||
| Male | 305 | 46.1% |
| Female | 280 | 42.4% |
| Gay/Lesbian | 7 | 1.1% |
| Bisexual | 40 | 6.1% |
| Unknown | 29 | 4.4% |
|
|
||
|
|
||
| Low | 450 | 68.1% |
| Moderate | 187 | 28.3% |
| High | 24 | 3.6% |
|
|
78 | 11.8% |
|
|
62 | 9.4% |
|
|
103 | 15.6% |
|
|
367 | 55.5% |
Acknowledgements
We extend our sincere appreciation to the students, teachers at Cau Giay, Yen Hoa and Nguyen Binh Khiem High Schools, for their participation. We also thank the Hanoi University of Public Health University for supporting fund to conduct this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.