
Abstract
Alopecia areata (AA) affects men at similar rates to women, yet comparatively little is known about men’s experience of the condition. We interviewed a demographically diverse group of 18 men with AA to explore this gap. From qualitative thematic analysis, participants’ accounts described a profound yet often-minimised impact of AA on their lives, in the context of poor public awareness and misguided assumptions about AA in men. Conversely, this adversity appeared to facilitate personal growth for many. These findings can help health professionals better understand men’s gendered experience of AA, which we discuss through the lens of masculinities theory.
Introduction
Alopecia areata (AA) is an autoimmune condition causing hair loss, with a lifetime prevalence of around 2.5% (Benigno et al., 2020) and 0.21–0.26 new cases estimated per 1000 people in a year in the US and UK (Harries et al., 2021; Mirzoyev et al., 2014). Hair loss from AA can range from patches on the scalp and/or face, to total hair loss on the scalp (alopecia totalis) and the whole body (alopecia universalis) including eyebrows and eyelashes. The precise aetiology of AA remains unclear, though it is known to be genetically mediated in some, with an elevated lifetime prevalence of 6–8% in first-degree relatives of those with AA and numerous genes implicated in AA development (Zhou et al., 2021). Findings on the gender predilection of AA are mixed but overall suggest parity in terms of prevalence between men and women during early-to-middle adulthood, and peak age of onset (though the peak age of onset in men may be narrower) (Harries et al., 2021; Pratt et al., 2017).
Although two-thirds of people with patchy AA will experience complete hair regrowth within 5 years, for many the clinical course of AA involves often unpredictable hair loss, regrowth, and/or recurrence over long periods (Trüeb and Dias, 2018). Interventions targeting hair regrowth for AA display limited efficacy, with no single treatment found to be superior in a recent meta-analysis (Fukumoto et al., 2021). The authors found that commonly adopted treatments, including corticosteroids and phototherapies, show only modest efficacy compared to no treatment, and that only 30% of treated patients experience long-term hair regrowth. In the UK, AA is predominantly managed in primary care, where referral to specialist dermatology professionals is only recommended where differential diagnosis or further specialist treatment is indicated (NICE, 2021) and only a quarter of UK primary care patients with AA are referred to dermatology (Harries et al., 2021).
AA can adversely affect psychological wellbeing through its impact on appearance and unpredictable, chronic nature. Elevated levels of depression, anxiety and health-related quality of life are consistently reported in men and women with AA compared to matched controls (Okhovat et al., 2019; F Rencz et al., 2016a, 2016b; Toussi et al., 2021). Specifically, embarrassment and social interaction have been found as the most affected areas of quality of life, pointing to the prominence of appearance-focused concerns (Toussi et al., 2021).
Qualitative explorations can deepen our understanding about individuals’ lived experience of AA beyond outcome measures alone, helpful in informing specialised psychosocial support for the population (Davey et al., 2019). Themes common across the qualitative literature describe changes to identity marked by shock and despair, attachment to hair, perceived loss of attractiveness, restricted engagement in social, occupational and romantic life, concealment as a primary coping strategy, and an overall narrative of a struggle towards self-acceptance and personal growth (with some perceiving the journey to personal growth as ultimately fulfilling; Aldhouse et al., 2020; Davey et al., 2019; Hunt and McHale, 2005; Jankovic et al., 2016; Montgomery et al., 2017; Stock et al., 2021; Welsh and Guy, 2009). However, most of this research has, by design or otherwise, either exclusively or predominantly focused on women with AA.
The few studies that have explored the lived experiences of mixed gender samples with meaningful representation from men have largely analysed the sample as a whole, with certain themes holding questionable relevance to men, such as a loss of femininity and participants’ experience of cosmetic procedures like wigs, makeup and medical tattooing (Aldhouse et al., 2020; Hunt and McHale, 2005). Where some authors have drawn distinctions between the experiences of men and women in this research, the findings pertaining to men’s accounts are superficial and underexplored. For example, it has been separately reported that men describe less use of support groups than women and fewer attempts to cover bald patches, without further elaboration on the reasons (Hunt and McHale, 2005; Welsh and Guy, 2009). In another study, Barkauskaite and Serapinas (2020) interpreted gender differences between the qualitative accounts of four women and two men with AA in their phenomenological analysis, suggesting that the men expressed more concern about the impact of AA on their ‘social identity’ whereas the women described a broader impact on their self-concept. Clearly, these analyses were limited by only involving two men. Without having posed questions to male participants about their gendered experience of AA in such studies, we currently have a very limited understanding of what it is like to be a man with AA.
There are various gendered factors that may influence men’s lived experience of AA. While much literature has made explicit or implicit inferences about the impact of heightened female appearance pressures related to hair loss on women with AA (e.g. Hunt and McHale, 2005; Tucker, 2009), constantly evolving and complex appearance pressures on men (Jankowski et al., 2018) have been largely ignored. The milieu of masculine ideals inhabited by many men (Levant, 2011) is also likely to shape their experience. This may manifest in terms of how men feel able to navigate their personal, social and medical experience of AA, for example through masculine norms deterring help-seeking behaviours (Hunt et al., 2010), as well as how they experience their masculinity within the context of their AA.
Focusing exclusively on men also enables exploration beyond gender as a homogenous entity (Gough and Robertson, 2017: p.210), to understand how demographic characteristics may relate to men’s experience of AA. Little is known, for example, about how or whether hair loss from AA may be distinctly perceived in men from sexual minority communities. Similarly, little is understood about the meaning attached to hair loss from AA across different ethnicities and cultural backgrounds. There are conflicting quantitative findings regarding the role of age and AA disease duration on individuals’ quality of life across gender (Rencz et al., 2016a, 2016b). While in qualitative and quantitative research on men’s experiences of androgenetic alopecia, or male pattern baldness, younger age of onset has been positioned as burdensome to men’s experience (e.g. Han et al., 2012; Razum, 2021), this has not been explored in male AA.
Aims
The aim of the present research study is to explore men’s experiences of living with AA via semi-structured interviews. This will help to understand the gendered challenges and perspectives that need to be considered in providing psychosocial and practical support to men with AA.
Methods
Design
The study was collaboratively designed as part of a larger research project by two researchers and two staff members of Alopecia UK, a national charity who support individuals affected by any form of alopecia, raise awareness of alopecia, and facilitate research on the condition. Three male public contributors who have AA and an association with Alopecia UK provided input on the design of the study, research materials and suitable questions. We also consulted an academic with expertise in critical perspectives on male hair loss. Collectively, we decided on semi-structured interviews as the most appropriate design for the study.
Recruitment procedures
We recruited participants from a larger sample of men with AA who had completed an online survey study for men with any form of alopecia, which focused on the support needs and preferences of men with alopecia. Within this survey, participants provided demographic data. Seventy-five survey participants expressed interest in being interviewed and provided their contact details. We adopted a purposive sampling strategy with a view to obtaining a demographically diverse group of up to 20 participants in terms of age, race/ethnicity, sexual orientation, relationship status and education level. The two researchers actively prioritised contacting individuals from marginalised demographic groups in the earliest rounds of recruitment to maximise their representation. Black and Asian men, in particular, were underrepresented in the survey sample, so all were contacted. In total the two researchers invited 38 survey participants by their chosen contact method and shared the participation information sheet and consent checklist, 20 of whom did not respond or declined the invitation. We offered participants a £20 online shopping voucher to compensate for their time (though we did not specify the amount in the participant information to avoid any potential for coercion).
Participants
Sample characteristics.

The interviews
The two researchers (first and second authors) conducted the interviews in January-March 2021, during which a mixture of full and partial ‘lockdowns’ due to COVID-19 were in effect across the UK. Researchers offered participants a choice of remotely-mediated interview platforms. Ten interviews were performed via phone or online audio service, and eight via Microsoft Teams. The first author conducted eight interviews and the second author conducted 10. Participants provided verbal consent at the start of the interview.
The researchers followed the interview guide flexibly and responsively according to the relative importance that participants attributed to each topic. After conducting their first interview each, the researchers met to review the guide, subsequently making minor modifications. The guide, shown in full in Appendix A, covered participants’ views and experiences concerning: 1. The role of appearance in society, including portrayal of AA in men and effects on appearance self-perceptions. 2. The impact that AA had on participants’ lives across life domains and in terms of identity. 3. The reactions of other people to participants’ AA and how they perceived such reactions. 4. Management of their AA, whether medical, cosmetic and/or psychological, from health services and self-management. 5. The gendered experience of AA, namely whether men experience AA in any distinct way, and the potential influence of any other personal background factors on their experience.
After covering these topics, the researchers asked participants what advice they would give to their younger self, and if they wished to discuss anything else relevant to their AA. Interviews lasted 38–81 min with a mean of 63 min. The researchers ended data collection once all potential participants from Black and Asian backgrounds (who remained underrepresented in the sample) had had sufficient time to respond to the researchers’ invitation, and on discussion felt there was a general convergence of participants’ accounts. They did not apply a strict data saturation criterion, whereby further data collection is assumed to provide redundant information, as their analytic approach holds knowledge as generated through researchers’ interpretation of data rather than being excavated from the data (Braun and Clarke, 2019b).
Data analysis
The digital interview recordings were transcribed by a third-party service provider. All transcripts were pseudonymised and any clearly identifiable data (e.g. location) removed. The researchers analysed the interview data using reflexive thematic analysis, a method characterised by ness and transparency of researchers’ worldview in generating themes that describe patterns of shared meaning in the data (Braun and Clarke, 2006, 2019a). The researchers shared a critical realist worldview, which posits an existent reality independent to human apprehension, which is only ‘imperfectly apprehendable’ (Guba and Lincoln, 1994) via data, as it is necessarily shaped by participants’ subjectivity (Fletcher, 2016).
The researchers broadly followed Braun and Clarke’s (2006) six-step procedure for reflexive thematic analysis, adopting a largely inductive approach focused at the semantic (i.e. manifest) level. The second author first familiarised themselves with the data by reading and annotating all transcripts, and then generated initial codes corresponding to small units of data in each transcript, compiled in a Microsoft Word document. They then examined the codes to identify patterns of shared meaning across the dataset, interpreting the codes and the data to abstract candidate themes.
Both researchers then reviewed these candidate themes against a subset of transcripts, by actively coding the subset on NVivo version 12, with the first author coding six transcripts and the second author coding 12. In doing so, both researchers constantly evaluated the relevance of the candidate themes to the dataset and reviewed the structural organisation of the themes. The researchers met to reorganise the candidate themes, ensure that the clusters of meaning that were considered most salient were incorporated into the structure, and revise the candidate themes before settling on their final names and definitions. The second author then coded all data to the new structure. By engaging in researcher triangulation in this way, we sought to enhance the breadth of our findings through accommodation of different perspectives (Davey et al., 2019). The three iterations of the authors’ NVivo thematic codebooks are presented in Appendix B. We also sent a summary of our findings to the 16 participants who had requested them, to which four replied without requesting any changes.
Researcher positioning
To aid the researchers’ reflection on the ways in which their theoretical perspectives, lived experiences, environment and personal characteristics may have shaped the data and their analyses, both researchers kept reflexive logs throughout data collection and maintained process notes throughout analysis. For example, the second author noted that he had held assumptions about men being largely unwilling to speak in depth and therefore requiring a high degree of probing during interviews, and how this may have initially affected their interviewing style. The first author noted self-consciousness and concern about participants’ reactions to his scalp and facial hair during interviews conducted via video calls. In terms of personal characteristics, both researchers identified as straight, white men in their 30s with no lived experience of alopecia. Both had experience of interviewing participants with appearance-affecting conditions, including alopecia.
Ethics
Prior to commencing recruitment, we gained ethical approval from the University of the West of England Faculty Ethics Committee, (reference HAS.20.07.201) for the wider research project, which included the interview study.
Results
The researchers’ analysis generated the four themes, each with subthemes, presented in Figure 1. We now summarise each theme and provide illustrative participant excerpts. Thematic map.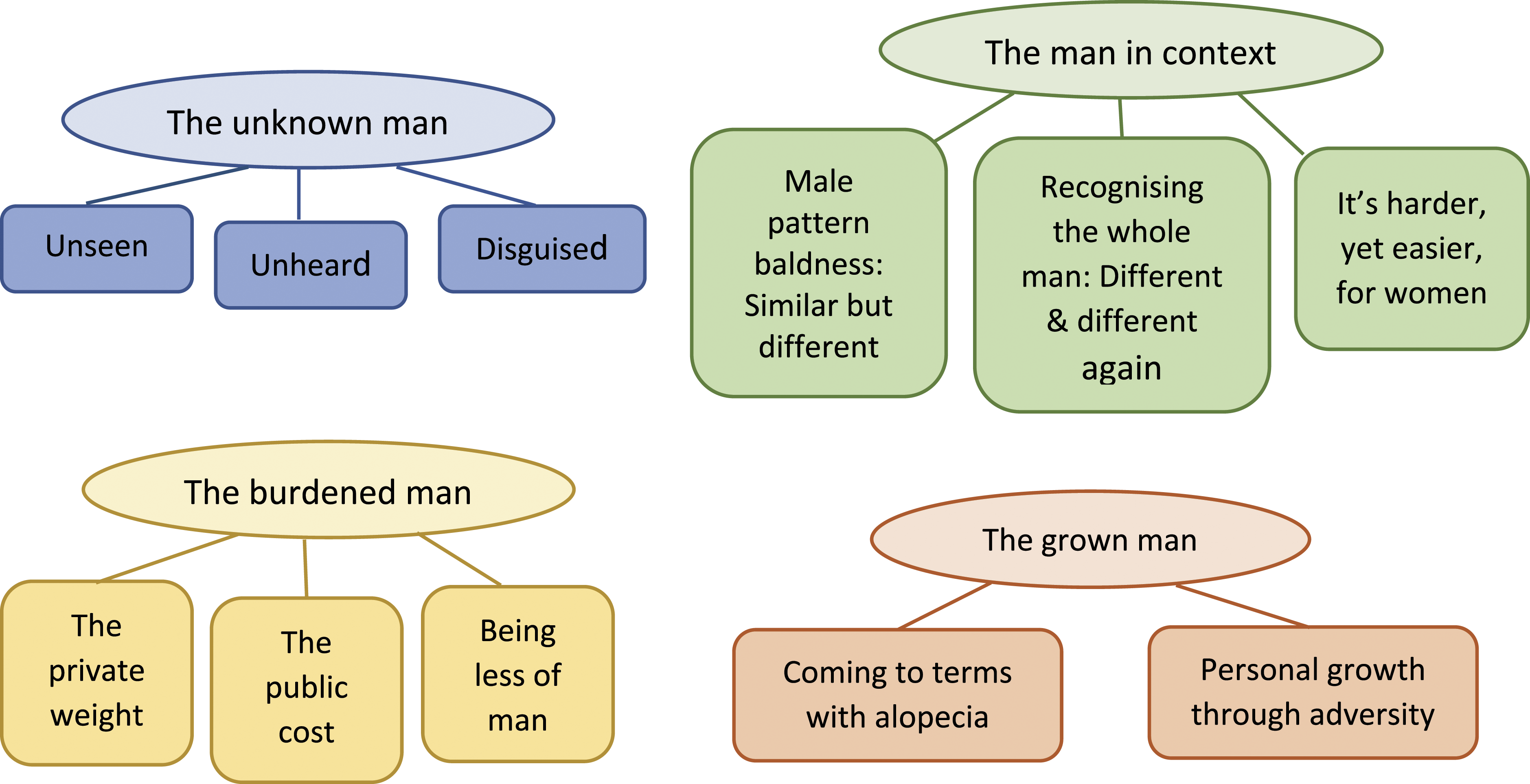
The unknown man
This theme explores the ways in which participants perceived their status as men with alopecia to be largely unknown at a societal and individual level. This sense of being unknown was characterised by a perceived lack of visibility of male alopecia in society and a subsequent lack of public awareness of the condition. Compounding this issue was a perception of minimal opportunity and inclination from most participants to share their experiences of AA and for others to understand their experiences. Most participants also discussed ways in which they had, to varying degrees, made efforts to keep their identity as a man with alopecia unknown through concealment and other strategies, and the challenges associated with these strategies.
The unseen man
With participants noting a prominence of appearance ideals in society, the majority argued that AA was barely represented in mainstream media, so remained generally invisible in everyday life. Though a minority of participants indicated that public awareness of AA had been increasing over recent years, most hoped for greater media representation as a means of raising public awareness. … it would be nice to see more people like me on sort of, like you say, TV and social media and that sort of thing, just to maybe normalise it a little bit more. (Lucian, 38)
In the absence of this representation and with the relative rarity of AA, a minority of participants reported feeling that most people, including themselves before developing AA, were generally unaware of the condition and often struggled to empathise with their experience: to be fair to me, until I had [AA], I didn’t know what it was and then I started noticing people with it more. I suppose it’s the same with anything really, unless you know somebody that’s gone through it or had it, that’s the only way you understand things. (Mason, 26)
The unheard man
A majority of participants indicated that they had rarely spoken about their experience of having AA, with the strong implication being that they had relatively few opportunities to do so: the first [Alopecia UK] trip, I volunteered for that… it was just like ‘I’ve had alopecia for 20 years or something and this is the first time I’ve actually spoken to another person properly [about it].’ (Stefan, 52)
Despite this, most participants who spoke to the topic expressed value in communicating their experiences, whether on an informal basis with friends or family members, with another person who has AA, or in more formal medical or support settings: I think the [Alopecia UK] Facebook group has helped me a lot… because you’re seeing, you know, a lot of other people going through exactly the same sort of things that you’ve been through... (Steve, 46)
A small contingent of participants disagreed, with one participant indicating contentment with practically-oriented self-reliance, while also implicitly recognising the benefit other men might gain from hearing others’ experiences of AA: I’m quite mentally strong … I deal with things in my own way, and I just go into myself. I don’t need to talk about it ... I’m happy to meet people, that’s fine, and share experience, but it’s not going to help me. It’s not practical … I’m a practical man. (Graham, 53)
Most participants also framed a lack of opportunity and/or willingness to talk about their AA within the wider issue of male reticence towards sharing personal feelings. However, they also felt this stemmed from the reactions of others to their AA: … even people that you know try to ignore it … so I’ve found myself bringing it up a lot of the time to people. But people have got that perception like whenever you do bring it up …“Oh, it doesn’t matter, it’s fine, you can’t really tell.” So, it never really leads on to much of a conversation. (Mason, 26)
The disguised man
A minority of participants indicated that having AA acted as a disguise, with others being unable to recognise them, meaning participants could choose to avoid unwanted conversations. say, if I’ve got a friend or a friend from school and I see them in a situation and I know … they don’t recognise me without hair… I don’t want to have a conversation with them because I don’t want them to be, like “Oh, it’s you! You’ve got no hair!”… I actively avoid making conversation with people that I think might not know it is me. (Kieran, 41)
Nearly all participants also described efforts to conceal or minimise their AA to others, via hats, hairstyling to cover patches, coloured powders and pens, wigs, shaving, dyeing regrown hair, microbladed eyebrows and glasses. Most participants stated they did so to control the noticeability of their AA and, in turn, the reactions of others, which some participants described as a relief: … people just see you, you know? You feel a bit exposed in a way. Just … unless you’re covering it up. (Lewis, 17) ... the best thing is when you’re wearing the hat, nobody’s looking and judging. (Max, 29)
These techniques came at a cost to participants. Some were impractical or ineffective in certain contexts such as intimate or outdoor settings, and a minority of participants described feeling inauthentic from trying to conceal their AA. Most felt limited as men in their choice for concealment techniques, hampered by perceptions of vanity and even comical associations in the case of wigs, and concerns over product quality: I had seen men that wore wigs as weak I guess. It’s always portrayed in films as a comedy thing, so that put me off it because I didn’t want to be the guy with the wig … the only other things I know about is tattooed-on scalps and eyebrows but I … don’t think they’re convincing so that’s why I haven’t done that (Cameron, 24)
The man in context
This second theme explores how participants’ experiences of having AA were shaped by contextual factors, namely perceived public attitudes about male hair loss, women’s experience of AA, and participants’ existing personal characteristics. Each of these factors in some way appeared to compound the psychological and social challenges of living as a man with alopecia. Most participants felt these difficulties were minimised and hence exacerbated, both through wrongly held assumptions by others that their hair loss was ‘normal’ male pattern baldness, and the prevailing impression that men have an easier time of hair loss than women. Half of the participants also described how developing AA had compounded an existing sense of ‘difference’ borne from their race, ethnicity, sexual identity and/or medical background.
Male pattern baldness: Similar but different
While acknowledging that men with male pattern baldness may often face psychosocial challenges, a majority of participants described such male hair loss as acceptable, unremarkable or even sexualised by societal standards, and, combined with minimal public awareness of AA, this led to their AA often being mistaken for male pattern baldness. In this context, most felt their experience of AA was minimised: … I don’t really deny it must be hard for people that go bald, particularly when they’re young, that must be awful for some … But … Sometimes it’s embraced, even sexualised a bit but … you don’t see patches [of hair loss from AA in mainstream media] so … to me, it’s a completely different ball game (Simon, 37). I think because men suffer from male pattern baldness it’s almost assumed that if you lose hair as a man then it’s kind of normal and … you should just kind of get over it because, people are going bald all the time (Lucian, 38)
Most participants noted important differences between AA and male pattern baldness, and the subjective impact these could have when people did notice a divergence from male pattern baldness (whether explicitly or implicitly): the way that the hair goes [with AA] is not very pretty ... I think with male pattern baldness, it’s more symmetrical and predictable … it doesn’t trigger other people’s sense of ‘Oh, there’s disease here.’ Whereas, with Alopecia Areata it looks like something is wrong. (Zahid, 41)
Recognising the whole man: Different and different again
Half of the participants considered their experience of AA to have been compounded by other salient and often socially marginalised aspects of their identity or demographic background. Participants identifying as gay discussed how their sexuality interacted with their experience of AA, in terms of perceptions within the gay community and reinforcing stereotypes: … the more attractive you are, the better in the gay community … it’s just completely, like … destroyed my confidence … especially being gay, it has been a lot harder having alopecia (Max, 29). being gay and people sometimes have the assumption that you’re going to be effeminate, and then suddenly you’ve no hairs either as well then, in my mind, it makes a difference. (Lucian, 38)
One participant also reflected on the effects of AA within the context of having received racist discrimination: before the hair loss it was the colour of my… skin… that I was angry with, because of what I was going through... I’d had a lot of race stuff – crap, so it’s been like a life of being angry at my own appearance and the psychology effect was really, really big (Jack, 54).
Other contributory factors mentioned by these participants included existing mental and physical health conditions (including those which affected their appearance already) and neurodiversity. I have mental health issues from an anxiety point of view, when I was young, you know, people would say ‘Oh, he’s shy’ … So, when I’m different to the norm, it is … you know, it just magnifies the problems that I have (Graham, 53). I was diagnosed with Asperger’s syndrome … It’s like two bad things on top of another … my perspective was guaranteed to be unique and possibly worse than normal (Anonymised).
It’s harder yet easier for women
This subtheme presents the paradoxical message conveyed across a majority of interviews that while most people, including many participants themselves, perceive women to be more negatively impacted by AA than men, this assumption itself causes unique challenges for men with AA. … society demands that [women] have hair and … you know, certain qualities and they look a certain way. I think men are much luckier (Shaun, 71). I’m quite open but I don’t know how to deal with it, you know?.. It’s probably more of an isolated experience than women, maybe? And maybe … as a man I don’t really want to talk about it all the time, you know? (Simon, 37)
In essence, though these participants felt that AA could be more damaging for women, this belief may contribute to men’s’ emotional experiences being less well recognised, and to men’s support and aesthetic requirements being relatively overlooked: … what society kind of projects onto us, or expectations for men. So, one of the things that I think’s pretty unfair is that, because you’re a man you shouldn’t really care so much about your appearance. (Zahid, 41). I think it’s easier for [women] to hide [AA], um … through make-up and uh, false eyelashes and eyebrows and all of that … (Tom, 38)
The burdened man
This third theme presents the myriad personal, social and physical challenges that participants described facing in connection with their AA. The personal challenges encompass participants’ reports of how their psychological wellbeing, identity, and their ability to live in the world unencumbered by self-consciousness, had all been compromised. A notable area of concern to most participants was a perception of emasculation as a result of developing AA, especially when body and facial hair were affected, which impacted their sense of identity and attractiveness. The social, or public challenges, included participants’ reports of uninvited attention about their hair loss, a reluctance to engage in certain public activities, and experiences of informing others about their condition.
The private weight
This subtheme captures the ways in which all participants felt their internal world had been affected by having AA. These included self-consciousness about their appearance, struggles with the unpredictability of AA and the often unfulfilled hope of hair regrowth, and mental health challenges: I had a sort of thin [eyebrow] line above each eye and they were clinging on for dear life for a while and then ... I think it was the week before the pandemic started and I actually took a week off work … with depression, so I couldn’t face going in to see people … (Lucian, 38) Other people … don’t judge me. It’s in me. The issue is in my head and how I feel about other people around me and looking at me. Because, I was always … I’m always anxious, so it’s a problem in me. (Graham, 53)
Half of participants also described a loss or change to their personal identity from AA, and for some a realisation of the place hair had held in their self-image: … in … school, I had an awful haircut but I used to … put loads of gel in my hair and have it spiked up … people used to call me Sonic the Hedgehog, which is quite a comedy thing, but it’s just knowing that I don’t have that hair now … it does feel like you’ve lost yourself a bit (Mason, 26)
The public cost
This subtheme extends beyond participants’ private experiences to their overt experiences of AA impacting on their public participation. Most recounted incidents, which most described as being fairly rare, in which mainly male others, ranging from classmates in school to strangers during adulthood, had acted in insensitive, unkind or offensive ways towards them since developing AA: I’d worked on building sites to get through Uni … you know, working class laddish culture and ... you just got the piss taken out of you … and then you’d have other people that would just see it as banter … I hate that word ‘banter’, but they would see it as banter … it hurt me. (Stefan, 52)
Most participants reported periods of reduced social activity, in which they avoided particular people such as historical acquaintances and certain social and public situations (such as those involving crowds): I’d never go anywhere new or unfamiliar. I’d always … if I was having a drink it’d be a drink after work where I work, you know?.. or I’d be like, go to a mate’s house. I’d never to … town, I’d never go somewhere where I’d feel uncomfortable. (Max, 29)
A minority of participants also reflected on how their AA had impacted their professional career. A very small number changed profession to escape perceived scrutiny, while others felt relieved that the COVID-19 lockdown had necessitated home working. Even when their work required them to be in a public setting, participants adjusted their behaviour: when I’m at work – I’m a retail worker– I know it sounds really stupid probably, I try not to turn around. So, when I’m on the till so then nobody’s looking at the back of my head. (Mason, 26)
Conversely, one participant did describe deliberately taking on a job involving high visibility and contact with customers, in order to build resilience: I did a bar job and it was kind of strange really, it was almost like a test to myself, put myself in this very public setting and interact with lots of people where I’ve got no choice but to not wear a hat because it wasn’t part of the uniform. (Richard, 35, AA)
Being less of a man
This third subtheme focuses on felt emasculation expressed by a majority of participants after developing AA, especially those who had lost hair beyond their scalp: … women shave their legs and all that kind of stuff, so that wouldn’t be a big loss for them. Whereas for a man, it’s a perception of your masculinity, big hairy arms, hairy legs, a beard … I guess it feels a bit emasculating because I don’t have… those stereotypical manly features. (Cameron, 24)
A minority of participants wistfully cited facial hair as a marker of masculinity. A small number also described emasculating associations with cosmetics such as wigs, and invoked self-comparisons with pre-pubescent children: losing my beard probably made me feel less masculine. Losing my scalp hair probably didn’t make me feel less masculine but it indirectly did, because I ended up getting a wig. (Zahid, 41). I miss shaving … it’s like a manhood thing isn’t it, shaving? Children don’t shave and the irony for me is I used to have a beard when no-one had beards and now everyone’s got some stylised beard and you can buy every sort of facial hair products … (Tristan, 41)
One participant explicitly linked masculinity to perceived attractiveness: “I absolutely felt less masculine… I felt like a worm… not attractive for sure” (Zahid, 44), and others also described concerns about how AA had affected their attractiveness.
The grown man
In contrast to the preceding themes, this theme recognises participants’ accounts of positive adjustment to AA, often attributed to the passing of time and with older age. This adjustment can be seen in two processes described by most participants: Firstly, the ways they had adapted (or continued to adapt) to their hair loss, learned to live with it, and come to accept, or ‘own’ the condition; and secondly, their efforts to make sense of their AA within the context of their lives, which had facilitated positive personal changes.
Coming to terms with alopecia
Participants often emphasised the importance of adapting to AA and to “just get on with it” (Tom, 38) as critical to progressing beyond AA. Most participants described a process of accepting and even embracing their hair loss. Though a minority still held hope for effective treatment, most reported relinquishing hope in long-term hair regrowth: I just said … ‘It’d be great if it grows back [but] if it doesn’t I’m not going to go out and obsess about finding the solution to it … I just need to get on with being a bit more relaxed in life.’ (Stefan, 52)
Half of participants described shaving areas affected by AA as a seminal act of acceptance, though paradoxically it could simultaneously be seen as a means of controlling their appearance: I actually shaved my eyebrows off and went into work … that was quite tough to do like … the reason I did that was because … when I was going bald, I just shaved it off just to sort of like ‘This is … this is how I am, this is what it looks like so …’ (Lewis, 17)
Personal growth through adversity
This final subtheme illustrates the ways in which most participants felt they had positively changed as a person since developing AA. These men talked about their experiences as having helped them to gain perspective on others’ suffering, feel more grateful, and develop empathy for others, and for some, help others with AA: I think [AA] did kind of provoke a sort of maturity out of me that was potentially almost there, you know? I feel like after that I was a lot … the importance of, like, understanding people’s differences and how they feel about things that you can’t necessarily see. (Lewis, 17) … with regards to volunteering and helping out … often parents [of children who have alopecia] ask a lot of questions and some of the conversations I had, I’ve felt like I’ve been helpful … and that’s one positive that’s come out of [having alopecia]. (Leigh, 33).
Most participants also described AA as a source of personal meaning and a catalyst for self-reflection, including their view of relationships, life philosophy, and a new sense of self-worth based on character rather than appearance: [AA has] had a massive positive on me, I’m definitely a better human being for … looking inwards rather than externally and seeing the good in me as a person rather than just some superficial hair, body, face … May sound a bit odd but I wouldn’t change the experience at all (Stefan, 52) [AA] really has just made me appreciate things a lot more. It’s just really opened my mind to people that stick around you and so on. They don’t stick around because of the way you look or anything, it’s all to do with how you are as a person (Mason, 26)
Discussion
Main findings
By interviewing men with AA, this study offers new insight into the gendered experience of life as a man with the condition. Findings point to men feeling unknown at a societal and personal level, and having an experience shaped by common assumptions and misunderstandings linked to comparisons with male pattern baldness and women’s experience of AA. Participants’ accounts concerning the intersection of having AA alongside appearance pressures related to gay communities and ethnicity also add important nuance to understanding men’s experience.
Perhaps most obviously unique to men was the felt emasculation participants described, especially in relation to hair loss beyond the scalp. Looking at the overall findings now through the lens of masculinities, the most empirically established model is the gender role strain paradigm (GRSP) (Levant and Richmond, 2016; Pleck, 1995), in which the traditional masculine gender role is viewed as a socially constructed set of norms, which, when performed by men, confer tangible interpersonal and reputational rewards and so are socially reinforced, and when violated, are met with social condemnation (Levant, 2011).
One form of gender role strain in the GRSP is discrepancy strain, whereby individuals perceive a discrepancy between their internalised ideal of manhood and their self-image. This discrepancy can be seen in participants’ accounts of emasculation from facial and body hair loss. This adds to an existing complex picture regarding the link between body hair and masculinity, with male grooming practices and body depilation being understood both as desirable and a potential threat to masculinity (Clarke and Braun, 2018; Jankowski et al., 2014). It may be that the involuntary nature of hair loss (rather than through grooming), and the asymmetrical or total nature of hair loss, exacerbates a loss of masculinity in men with AA, especially AA universalis. Investigating the psychosocial impact of such discrepancy strain would be the remit of future quantitative work.
According to GRSP-informed research, men from certain groups in which gender role strain is especially pronounced are also likely to experience trauma strain. Given that heterosexual presentation is a traditional masculine norm (Mahalik et al., 2003), growing up as gay or bisexual has been posited as normatively traumatising (Connell and Messerschmidt, 2016; Sánchez et al., 2010). A loss in masculine capital could therefore impact sexual minority men through trauma strain in addition to discrepancy strain. From participants’ accounts, sexual minority men may also face additional challenges from within their community, within which appearance is often emphasised (Carper et al., 2010; Jankowski et al., 2014), and rates of body dissatisfaction are disproportionately high (e.g. Alleva et al., 2018). Combined, these factors suggest gay and bisexual men may be particularly impacted by AA, so further research on this group of men with AA as well as other appearance-affecting conditions is warranted. Dysfunction strain describes negative consequences of adherence to traditional masculine norms. This can be seen in participants’ accounts of reluctance in voicing their experiences to others, in so doing conforming to masculine norms of self-reliance and emotional control (Addis and Hoffman, 2017: p.171) despite their recognition of the value in sharing with others. Participants also expressed frustration with these masculine norms at a societal level and attributed them to minimisation of men’s distress, such as how they felt expected not to care about their appearance and not share personal feelings. Interestingly, these masculine norms could also be seen in men’s accounts of growth and acceptance (e.g. the need to “just get on with it”), which points both to potential benefits of maintaining masculine norms (perhaps dependent on individual differences in coping strategies), as well as to a pervasive ‘filter’ of masculinity in how men articulated their experiences of having AA. Overall, findings reinforce the need for health professionals to reflect on how masculine socialisation may manifest in male clients with AA, especially when engaging in psychological support (Seidler et al., 2018).
Although confined to one participant who identified with mixed ethnicities, the account of AA as compounding a sense of stigmatised appearance borne from experiences of racism, point to the possible intersection between skin colour and/or ethnicity, and AA, in men’s lived experience. Creadore et al. (2021) found that individuals who viewed headshots, edited to show differing levels of AA, reported a greater shift towards stigmatising beliefs about the headshot subject as AA severity increased for Black men compared to White men or women of either skin colour. This suggests an intersection not just between skin colour and AA, but also male gender, in shaping stigma. Greater exploration of this subgroup’s experiences would be worth pursuing.
Participants’ accounts also highlighted the gendered nature of cosmetic products popular in AA management. For example, men noted comic associations with wigs, and feminine associations with makeup and cosmetic tattooing, and hence a reluctance to use such products. While research shows that women value access to high quality wigs (e.g. Montgomery et al., 2017) and so guidance promoting wig provision such as that from the UK’s National Institute of for Health and Care Excellence (NICE, 2021) is fully justified, it is clear that men’s preferences are not currently incorporated into such guidance. Recognising this gendered issue in such guidance would offer a helpful starting point, while developing support and advice tailored for men, and signposting to such a service or information would be a welcome next step.
Participants’ accounts convey perceived public attitudes towards male pattern baldness as a noteworthy contextual factor in shaping their experience of AA. Being mistaken for having male pattern baldness was cited by participants as a common source of frustration and minimisation, and many made upward comparisons to those affected by male pattern baldness. Participants’ concerns over people’s implicit assumptions that their hair loss is associated with illness or contagion is one supported by recent research examining public responses to images of men with alopecia (Creadore et al., 2021). Research does suggest certain similarities between the experiences of (especially young) men with male pattern baldness and men with AA, with affected men often feeling less attractive, more self-conscious and engaging in efforts to cover their hair loss (Kranz, 2011; Razum, 2021). However, while men with male pattern baldness often attribute loss of attraction to appearing older than they are, participants’ accounts in this study appear to attribute reduced attractiveness in AA to an emasculated, sometimes preadult appearance.
It is also worth considering how this study’s findings relate to our theoretical understanding about psychological adjustment to AA. Researchers have adopted the Commonsense Model of self-regulation in health and illness (Leventhal et al., 2001) to investigate the role of illness perceptions and coping strategies in informing people’s experience of AA (Cartwright et al., 2009; Willemse et al., 2019). In both studies, which had predominantly female samples, individuals’ quality of life was found to be predicted by illness perceptions of worse consequences, strong identification with AA, and a strong emotional response to developing AA. These factors can be seen in this study’s findings, and better understood in terms of how men with AA define them: Consequences were most often described in terms of reduced attractiveness and masculine capital, illness identity was apparent in participants’ description of having highly visible symptomology, and strong emotional responses included shock to self-identity and acute self-consciousness.
Willemse et al. (2019) also found that active emotional coping, such as using humour, positive reframing and acceptance, and sharing feelings with others was associated with better quality of life in participants. While some men in this study did report using such strategies, for example by taking perspective on others’ suffering, and learning to accept their AA, they also described barriers to this broad strategy, especially in feeling unable to share their feelings with others. This is consistent with research showing men on average use more emotional inhibition coping (Matud, 2004).
Participants’ description of personal growth through AA can be understood as posttraumatic growth, a phenomenon in which individuals emerge from stressful experiences related to traumatic life events having endowed meaning to these events, and ultimately find benefit and personal growth from the process (Tedeschi and Calhoun, 2004). Men discussed processes and outcomes commonly associated with posttraumatic growth, such as self-reflection and altered life philosophies, a new-found sense of gratitude, such as for one’s health and social support, as well as rewarding experiences of ‘giving back’ as positive role models for male alopecia (Tedeschi and Calhoun, 2004). Meta-analytical findings suggest that men are less likely on average to experience posttraumatic growth than women (Vishnevsky et al., 2010), which the authors suggested may be due to men’s minimal use of deliberate, contemplative rumination (Treynor et al., 2003). Given participants often talked about self-reflection as a path to personal growth, it may be that encouraging men with AA to do so, whether guided by a professional or via self-guided journaling (e.g. Ullrich and Lutgendorf, 2002), could help facilitate positive adjustment. For example, perspective-taking exercises such as those involving giving perspective to an imagined younger self, which we inadvertently included at the end of the interview, have been shown to increase self-compassion and reduce emotional discomfort in a mixed-gender sample (Boland et al., 2021).
Participants largely endorsed assumptions, which are also echoed in research findings (Tucker, 2009), that women experience a greater negative psychological impact from AA due to heightened appearance pressures. They also highlighted the ironic consequence of this assumption, in which their own psychological experience is minimised. Such minimisation may also become internalised, as has been demonstrated in men’s minimisation of appearance concerns in the general population (Jankowski et al., 2018).
Limitations of the present research
A limitation of this study was the underrepresentation of men from ethnic minority groups. This is especially pertinent given recent epidemiological findings showing that AA is over three times more prevalent in people of Asian ethnicity in the UK (Harries et al., 2021). There were also no Black participants in the sample, significant as this is a group for whom masculinity trauma strain is likely to be pronounced (Johnson-Lawrence et al., 2013), and public stigma towards those with AA in the form of intent to maintain social distance is especially prevalent (Creadore et al., 2021). The timing of the study, amid the COVID-19 pandemic and national lockdowns, is also likely to have affected participants’ accounts and should be borne in mind when interpreting the findings. For example, some men described relief at being asked to work from home so they could avoid social contact.
Conclusions
This study adds much needed depth to our limited understanding of men’s experiences of AA. The findings suggest men can feel unrecognised, isolated and self-conscious about their appearance within an appearance-focused society in which there exists minimal understanding of male AA. Nevertheless, the adversity that AA presents may ultimately also serve as a catalyst for personal growth in affected men. Health professionals involved in supporting men with AA should consider these gendered experiences in their practise, as well as masculine norms that likely mediate many of these experiences.
Supplemental Material
Supplemental Material - Men’s experiences of alopecia areata: A qualitative study
Supplemental Material for Men’s experiences of alopecia areata: A qualitative study by Fabio Zucchelli, Nick Sharratt, Kerry Montgomery and Jen Chambers in Health Psychology Open
Supplemental Material
Supplemental Material - Men’s experiences of alopecia areata: A qualitative study
Supplemental Material for Men’s experiences of alopecia areata: A qualitative study by Fabio Zucchelli, Nick Sharratt, Kerry Montgomery and Jen Chambers in Health Psychology Open
Footnotes
Acknowledgements
The authors would like to thank all the participants who took part in this study, the public contributors who offered their time and lived expertise to develop the study, and Dr Glen Jankowski who gave a valuable critical psychology perspective in reviewing the study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a small grant from the Vocational Training Charitable Trust Foundation.
Data availability statement
We are not able to provide the raw transcript data from which the findings were derived because participants did not consent to their transcripts being shared publicly.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.