
Abstract
Men’s baldness can be structurally stigmatized. For example, commercialized psychology research medicalizes it as a distressing “disease.” A mixed-methods survey on baldness stigma among 357 balding men (49% from Central- and South- America, Africa, Asia) was conducted. Qualitative and quantitative responses were content analyzed into two approximate sets: those (1) impacted by baldness stigma versus (2) those resisting baldness stigma. (1) The former included about half who had internalized baldness stigma agreeing it was disadvantageous (44%) and reporting distress (39–45% e.g. “[I] dread the future”). Participants reported baldness was stigmatized structurally (68%; e.g. “[it’s a] humiliating image”) and were attempting to combat their baldness largely via “treatments” (57%). (2) The latter participant response set resisted baldness stigma by reporting minimal distress, and structural stigma whilst accepting baldness (33–61%). Psychosocial and evidence-based support is needed to help some men resist baldness stigmatization.
Keywords
Stigma and baldness
Baldness is one of the most common bodily changes a man will experience in his life. About half of men will lose their head hair by age 50 and most by age 70 (NHS, 2018). Baldness can start in adolescence but mostly occurs from midlife. Although baldness has no detrimental physical health consequences (Trueb, 2021) and bald men live as long as men with a full head of hair (Menotti et al., 2006; Schnohr et al., 1998), it is heavily stigmatized as a disadvantageous disease (Harvey, 2013; Jankowski and Frith, 2022).
Goffman (1956) originally conceptualized stigma as a near inescapable reduction in humanness based on a perceived negative characteristic (e.g. having a mental illness; Livingston and Boyd, 2010). This influential conceptualization of stigma has been widely applied and variously defined. In their systematic review of stigma research on mental health Livingston and Boyd (2010) extended it to three mutually reinforcing types of stigma. These include structural (cultural, political, and broader pressures that negatively position a group of people) social (hostile relations between people that cement a negative position) and internalized forms of stigma (personal endorsements of negative beliefs about an individual absorbed from social and structural sources). These stigmas may be consequential whether in damaging self-esteem and wellbeing (Earnshaw et al., 2021; Livingston and Boyd, 2010) and in dictating responses (e.g. undergoing hair transplant surgery).
Structural and social baldness stigma
Baldness stigma is most often recognized in its social form. Specifically, experimental and cross-sectional studies consistently show more negative perceptions associated with baldness including aging, unattractiveness, and being less successful (Henss, 2001; Kranz et al., 2019). Baldness’ social stigmatization is complex, however. For example, some people rate baldness as more masculine, honest, and intelligent (Henss, 2001; Jankowski et al., 2021a, 2021b; Kranz et al., 2019) and baldness’ social stigma can be overcome by other individuating information (Kranz et al., 2019). Further research is needed to unpack these findings.
Baldness is also stigmatized structurally through research, organizations, and media. Media structurally stigmatizes a range of health conditions (Earnshaw et al., 2021; Livingston and Boyd, 2010) including by rarely representing baldness (Baldwin, 2005; Jankowski et al., 2014). This leaves the dominant representation of baldness in specific -forums, -social media, and -websites. Most of these platforms are biased including by being funded by anti-baldness businesses. One analysis found between 50% and 71% of popular hair loss YouTube Videos (Behbahani et al., 2020) and hair loss Facebook pages (Gupta and Ivanova, 2020) respectively have commercial links. Even 71% of dermatology organizations have evidenced commercial links (Li et al., 2019). Demonstrably the presence of such commercial biases is reflective of the promotional purpose of these platforms; effectively they advertise anti-baldness products. For example, in Gupta and Ivanova’s (2020) analysis of 500 of the most popular hair loss YouTube “treatment” videos, most promoted anti-baldness products without noting their limitations and with little meaningful disclaimer. Furthermore, the representations of bald men featured tend to be negative across this media. For example, eight popular baldness websites were found by Harvey (2013) to feature bald men as lonely, unlovable, and depressed. In contrast, non-bald men were depicted as happy, successful, and desirable (Harvey, 2013).
Commercially funded research structurally stigmatizes bald people via medicalization, that is, baldness’ transformation into a disadvantageous disease. For example, baldness is increasingly defined as a genetically inherited and hormonally mediated disorder, that is profoundly psychologically, societally, and physically disadvantageous (AGA; Frith and Jankowski, 2024; Jankowski, in prep.). Consequently, anti-baldness products are promoted through research as necessary “treatments to cure the disease” and avoid stigma. A systematic review of baldness psychosocial research (Jankowski and Frith, 2022) found that most studies had commercial links (78%), referred to baldness as a disease (77%) and recommended “treatments” (60%) with minimal discussion of the “treatment” limitations (68%). Furthermore, these psychosocial studies recruited predominantly “treatment-seeking” balding men (68%) who are unrepresentative of the general population of balding men and have been found more likely to internalize baldness stigma (Enitan et al., 2022; Gosselin, 1984; Han et al., 2012; Kranz, 2011). Alfonso et al. (2005) is an example of commercialized psychosocial research that stigmatizes baldness. The study is funded by Merck who manufacture a widely marketed anti-baldness “treatment”, is highly cited and informs dermatological professional guidance (which itself contains commercial biases; Blumeyer et al., 2011). It purports to be about men’s psychosocial experience of baldness but recruits only “treatment-seeking” men via a market research company. It promotes “treatments”, omits their side effects and includes other commercial “spin.” Specifically, when 34 hair loss practitioners (e.g. transplant surgeons) were recently assessed (Jankowski and Kranz, 2024) on their understanding of the study, 42% were misled by the abstracts’ statement. Specifically, they overestimated how many of Alfonso et al.’s balding participants internalized stigma and benefited from “treatments”. Baldness’ structural stigmatization through psychological research emphasizes the need for objective, commercially independent, research.
Research’s structural stigmatization has been facilitated through biased sampling of balding men. As mentioned, most balding male samples overrepresent those who are “treatment” seeking and have internalized stigma. Such samples are also “racially” and nationally unrepresentative. Currently, participants from Britain, the US, Australasia, and Asia dominate in baldness studies (Frith and Jankowski, 2024); as the Global North dominates the social- and health- sciences generally (De-Graft Aikins and Marks, 2007; Thalmayer et al., 2021). Historically however, “race” has been misused as a real biological characteristic to bolster eugenicist claims that baldness evidenced White men’s “hairless” evolutionary superiority (Jankowski, in prep.). Today baldness professionals can study only white scalps and straight hair in medical textbooks (Aryiku et al., 2015). This “race” sampling bias and racist history reflects the likely racist standpoints of those in the field of baldness research. Such researchers fail to understand “race” is a social construction with no biological, genetic, or material basis (De-Graft Aikins and Marks, 2007). Yet enough evidence suggests baldness is common across “racial groups” (Enitan et al., 2022; Yildirim et al., 2022). Subsequently, baldness -knowledge and even -professional care for African men is especially lacking (Aryiku et al., 2015). Thus, baldness research should include internationally diverse, non-commercially biased, samples of balding men. Quantitative research on such samples can help assess the proportion of balding men who actually seek treatments, and have certain balding experiences, against prior skewed estimates.
Baldness’ structural stigmatization through commercially biased research has been facilitated through other methodological biases. This includes limited market research designs, leading-questions, and skewed analyses (e.g. Alfonso et al., 2005). As such baldness experiences remain exploratory requiring qualitative assessments that can better detect underheard experiences. The strengths of a mixed methods approach (Dures et al., 2011) are needed.
Internalized stigma and stigma consequences
Few qualitative studies have been published on balding men’s experiences. Three exceptions show how stigma can be internalized within bald individuals themselves (Ford, 2018; Jankowski et al., 2021a; Razum and Vukasović Hlupić, 2022). Two such studies analyzed bald men’s experiences on popular English-language baldness forums (Ford, 2018; Jankowski et al., 2021a). Both analyses found balding male forum users described it as aging, demasculinizing, and ugly. Some mocked other balding men. A third study of men’s baldness used semi-structured interviews with 11 young (<36 years old) white balding men from Croatia (Razum and Vukasović Hlupić, 2022). Participants indicated baldness could result in a lack of control and a loss of attractiveness and sometimes discrimination in interpersonal and romantic settings. Across the three studies some male participants resisted baldness stigma. For example, by questioning whether stigma could also be a self-fulfilling prophecy and was exaggerated. These men emphasized the neutral experience of baldness they had. These findings need unpacking.
Baldness’s stigmatization may be consequential; influencing how men respond to it. For example, medicalizing- and emphasizing the biogenetic nature- of a bodily issue (e.g. mental distress, abnormal cells) has been found to influence the action or response undertaken by individuals (Nickel et al., 2017). Specifically, individuals are more likely to elect for invasive treatments, to disregard their safety information and to dismiss psychosocial alternatives. Arguably baldness stigmatization is primarily driven by pressures to get balding men to buy anti-baldness products. Whilst it is evident that baldness stigma can become internalized in the individual with bald men reporting distress, concern, and agreement it is a disease (Ford, 2018; Razum and Vukasović Hlupić, 2022), assessing how men actually respond to their baldness (rather than simply perceive its impact) is important.
The current study
Baldness is heavily stigmatized socially, structurally, and internally. Such stigma may have consequences in determining how men are impacted and respond to baldness. However, existing baldness research is often closely tied to anti-baldness businesses and tends to recruit biased samples of “treatment” seeking balding men who are not from Africa or South America. This leaves baldness experiences exploratory and disproportionately skewed toward treatment seeking bald men. The current study therefore used a mixed methods design among a non-biased, diverse, sample of bald men to answer the following questions:
How do men perceive structural and social baldness stigma (if at all)?
How do men internalize baldness stigma (if at all)?
What are the consequences of this stigma on men’s current and anticipated baldness responses?
Data and methods
Participants
Three hundred and fifty-seven men aged 19–64 years old (M = 29.43; SD = 8.94) who had baldness on average for 4.79 years (SD = 4.40) took part. Most indicated their baldness extent was mild (61%), followed by moderate (24%), advanced (10%) and unclear (5%). Most participants were heterosexual (90%) and employed (64%). Half indicated they were single (55%) and 20% indicated they were highly educated (i.e. had a postgraduate degree). Three hundred and forty-six participants indicated their nationality. The most common nationality was Mexican (19%) followed by South African (15%), Portuguese (14%), Polish (12%), British (7%), and Chilean (5%). The remaining 18% indicated they were from 1 of 35 other countries. Half (51%; n = 176) were classified as from the Global North (Europe, North America, or Australasia) and 49% as from the Global South (n = 172; Central- and South- America, Africa, and/or Asia; Dados and Connell, 2012). 348 participants indicated their “race.” These were categorized as White (39%), Hispanic/Latinx (27%), Black (21%), Asian (8%), Mixed (5%), and Arab (1%).
Design
This study concerns all qualitative and some quantitative answers to an online survey about baldness stigma (including structural, social, internalized forms, and consequences of this stigma). These questions were taken from a larger study with two other focuses. One focus was a quantitative assessment of baldness’s relationship to perfectionism and aging anxiety. The results of which are reported elsewhere (Kranz et al., 2023). Another assessed the impact of an experimental manipulation of medicalizing versus de-medicalizing baldness information via a short text (~350 words). The experimental impacts were assessed with specific measures and are reported elsewhere (Razum et al., in prep). All project materials including experimental texts were pre-registered and open access 1 .
Procedure
After receiving institutional ethical approval, in summer 2022, Prolific (the research management company) was utilized for the study. To achieve a “racially” and internationally diverse sample of balding men, two short screening surveys were conducted among English-speaking Prolific users that indicated their sex was male, and their “race” was either BAME (Black, Asian, and Minoritized Ethnic) or White at an approximate 2:1 ratio. Funding for 362 study places were offered to participants whose pre-screen completion time was average (between 30 and 100 seconds; Chandler et al., 2020) and who were balding/bald (54% of BAME and 52% of White approached Prolific users). Three hundred and fifty-seven accepted. Response completions for the qualitative questions ranged from 233 to 348 and for the quantitative ranged from 348 to 356. Participants completed the main survey including initial closed ended questions, then the embedded experiment, and further closed-ended and open-ended questions. Participants then read the debrief and gained their incentive (£5.25).
Measures
Due to a lack of previous research that has typically relied on quantitative market-research surveys (e.g. Alfonso et al., 2005), questions were constructed for purpose based on previous qualitative research with balding men (Jankowski et al., 2021a; Razum and Vukasović Hlupić, 2022) and relevant theory (Harvey, 2013; Livingston and Boyd, 2010) by the first author and refined by the other authors (e.g. so that they weren’t leading). Specifically, we included four assessments of baldness’ structural stigmatization, one of baldness’ social stigmatization, four of internalized baldness stigma including distress, and two of the consequences of baldness stigma.
Social and structural stigmatization (questions 1-5)
Participants completed three quantitative and one qualitative measures/questions relating to social stigma, commercial influences in baldness culture, baldness advertising exposure, cultural baldness stigma, and advertising stigma.
1 Social stigmatization
Participants were asked to indicate on a five-point agreement scale (ranging from 1 = strongly disagree to 5 = strongly agree) that “bald people are perceived more negatively.”
2 Commercial influence in baldness culture estimation
Participants were asked to “please estimate what percentage (if any) of the following sources of information about baldness have commercial biases (e.g. funding or content is provided by a business or individuals that sells anti-baldness drugs, products or services such as hair transplants).” Participants estimated this for five baldness information sources including baldness research, “treatment” YouTube videos; “treatment” Facebook pages; forums and organizations on a numerical scale from 0% to 100%. Scores were averaged with higher scores indicating greater commercial estimations.
3 Advertising exposure frequency
Participants were asked how often they had seen the following on a five-point Likert scale ranging from (1) never to (5) very frequently for the advertising of finasteride (e.g. Propecia®) or minoxidil (e.g. Rogaine®); scalp micropigmentation (SMP; i.e. scalp tattooing of hair follicles); wigs or other hair systems; hair transplants; and other anti-hair loss creams or shampoos. Scores were averaged with higher scores indicating greater exposure.
4 Advertising’s stigma
Participants were asked: “What impact, if any, do these baldness adverts have on balding men do you think?” in an open-ended format.
5 Cultural stigma
Participants were asked: “What role, if any, do you think culture (e.g. social media, advertising, the way men with hair loss are portrayed on television/in the media, jokes or stereotypes) has on how men view their baldness?” in an open-ended format.
Internalized stigma (questions 6-9)
Participants completed two quantitative and two qualitative questions relating to baldness’ internalized stigma.
6 Disadvantage
Participants were asked to indicate on the above five-point (dis)agreement scale that “baldness has no possible advantages to it.”
7 Internalized stigma and distress
Participants’ internalized stigma and associated distress related to balding was assessed with the nine-item Quality of Life with AGA Scale (Razum and Vukasović Hlupić, 2022). Items (e.g. “Baldness makes me less confident in flirting with potential partners” and “Baldness makes me panic.”) were rated on a five-point scale, ranging from 1 (strongly disagree) to 5 (strongly agree). Scores were averaged with higher scores indicate a higher distress relating to baldness. Scale reliability was good, Cronbach’s α = 0.89.
8 Current impact
Participants were asked: “What impact (if any) would you say your baldness has had on you?” in an open-ended format.
9 Anticipated impact
Participants were asked: “What impact (if any) will your baldness have on you in the future do you think?” in an open-ended format.
Stigma consequences (questions 10-11)
Participants completed two qualitative questions assessing their baldness’ responses (or consequences of stigma).
10 Current response
Participants were asked “What have you done (if anything) in response to having baldness?” in an open-ended format.
11 Anticipated response
Participants were asked “Are you considering doing something about your baldness in the future?” in an open-ended format.
Analytical procedure
The quantitative and qualitative questions were analytically integrated, deductively, into two participant response sets in reference to structural-, social-, internalized-, and consequences of- stigma (Dures et al., 2011; Livingston and Boyd, 2010). For the quantitative questions averages and percentages are presented below and are also summarized in Table 1. Percentages do not total 100 as blank and neutral/ambiguous responses are not presented.
Quantitative proportions of question responses that map into the two baldness groups (1) stigma impacted and (2) stigma resistant.
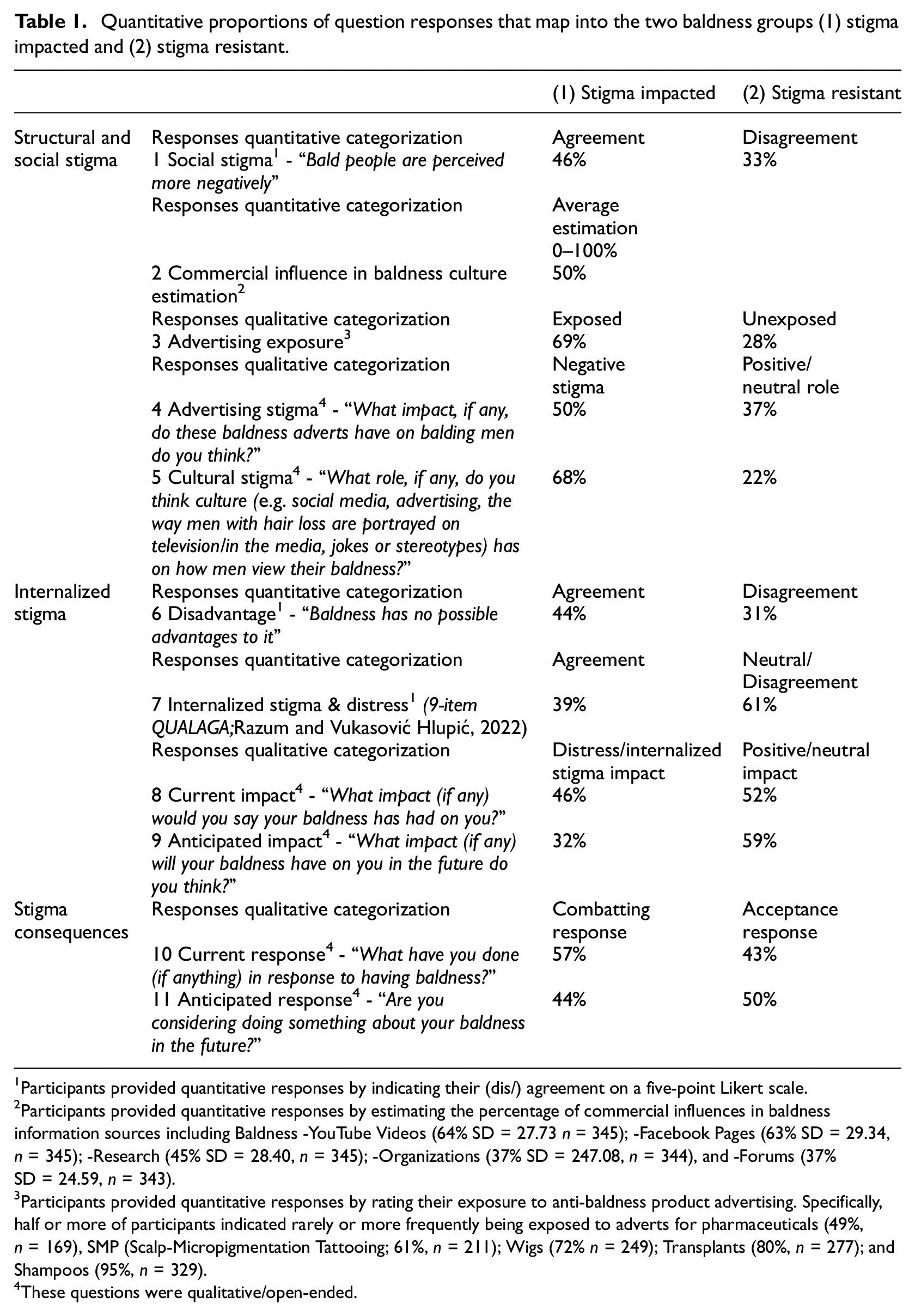
Participants provided quantitative responses by indicating their (dis/) agreement on a five-point Likert scale.
Participants provided quantitative responses by estimating the percentage of commercial influences in baldness information sources including Baldness -YouTube Videos (64% SD = 27.73 n = 345); -Facebook Pages (63% SD = 29.34, n = 345); -Research (45% SD = 28.40, n = 345); -Organizations (37% SD = 247.08, n = 344), and -Forums (37% SD = 24.59, n = 343).
Participants provided quantitative responses by rating their exposure to anti-baldness product advertising. Specifically, half or more of participants indicated rarely or more frequently being exposed to adverts for pharmaceuticals (49%, n = 169), SMP (Scalp-Micropigmentation Tattooing; 61%, n = 211); Wigs (72% n = 249); Transplants (80%, n = 277); and Shampoos (95%, n = 329).
These questions were qualitative/open-ended.
To analyze the qualitative answers a mixed content analysis was conducted. Content analysis has been defined as “[where] the researcher uses analytical constructs, or rules of inference, to move from the text to [answer] the research questions” (White and Marsh, 2006, p. 27). It allows for the retention of in depth meaning, through the broad range of categorizations created, alongside quantification of response prevalence. Categories were informed by medicalization and stigma theory (Conrad, 2007; Livingston and Boyd, 2010), previous evidence of balding men’s coping strategies (Kranz, 2011) and the responses themselves. Credibility and rigor was promoted (Dures et al., 2011; White and Marsh, 2006) through refinement of the categories against raw responses and across questions, a detailed audit trail and analytical consultation from the other researchers. For example, responses were initially content analyzed as “distress” until it became clearer some participants indicated distinctly more distress than others in line with previous meta-analyses (Huang et al., 2021). Thus, these responses were content analyzed into “distress” and “severe distress” categorizations. The analysis was conducted without the first author being aware of participants’ demographics, other responses or condition randomization. Qualitative broad categorizations are reported in text below including proportions whilst Table 2 presents further detail and subcategorizations for these qualitative answers.
Extended qualitative responses to baldness culture, advertising, impact, and response questions.
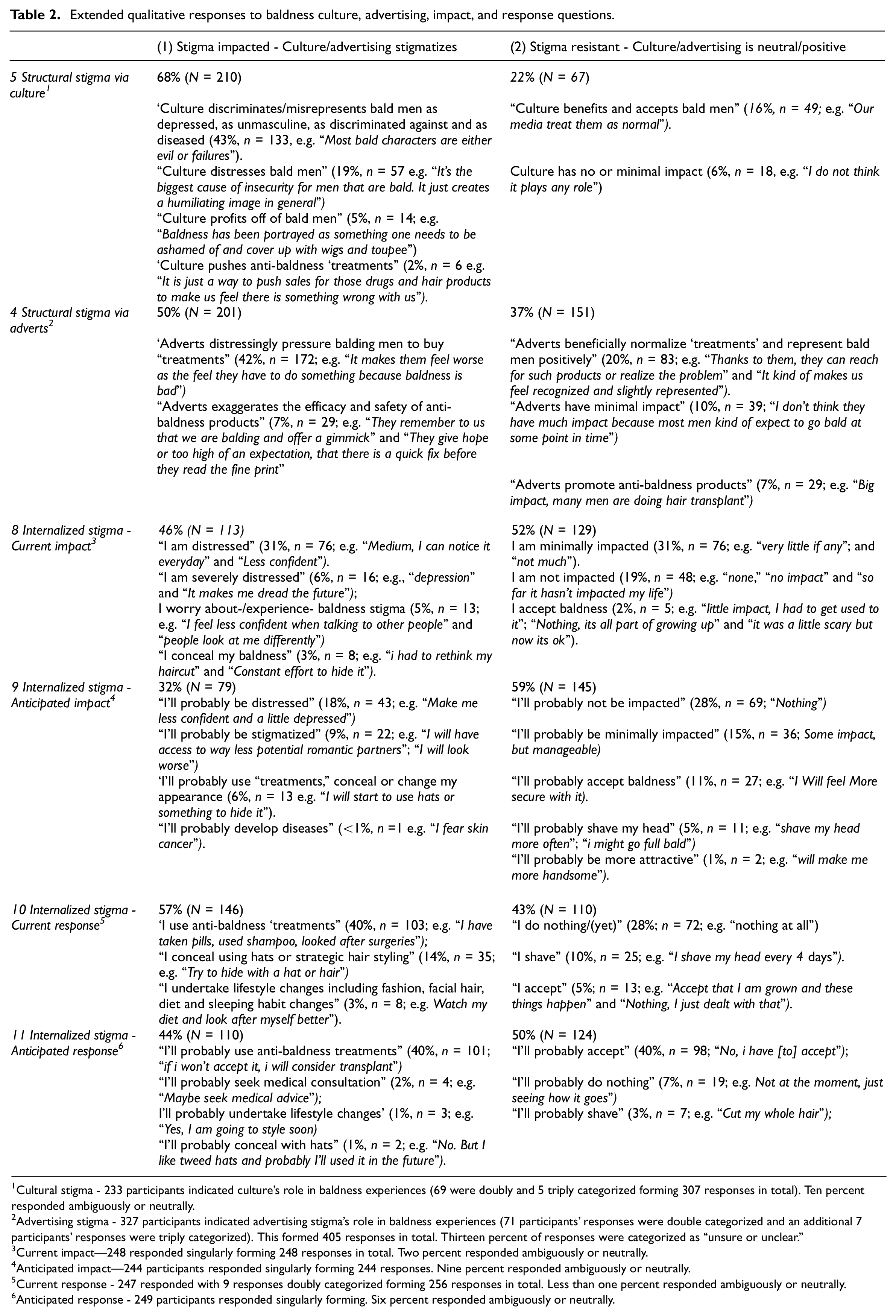
Cultural stigma - 233 participants indicated culture’s role in baldness experiences (69 were doubly and 5 triply categorized forming 307 responses in total). Ten percent responded ambiguously or neutrally.
Advertising stigma - 327 participants indicated advertising stigma’s role in baldness experiences (71 participants’ responses were double categorized and an additional 7 participants’ responses were triply categorized). This formed 405 responses in total. Thirteen percent of responses were categorized as “unsure or unclear.”
Current impact—248 responded singularly forming 248 responses in total. Two percent responded ambiguously or neutrally.
Anticipated impact—244 participants responded singularly forming 244 responses. Nine percent responded ambiguously or neutrally.
Current response - 247 responded with 9 responses doubly categorized forming 256 responses in total. Less than one percent responded ambiguously or neutrally.
Anticipated response - 249 participants responded singularly forming. Six percent responded ambiguously or neutrally.
Chi squares tests and T tests were conducted to analyze any group differences (e.g. global nationality, “race”) in stigma responses. To conduct these analyses, responses were further simplified and collapsed (e.g. Misrepresentation and Distress were content analyzed together as Negative and participants’ multi responses were coded into a singular, dominant, response) to meet the sample size requirements of the tests (e.g. expected cell counts). Furthermore, the “racial” groups: Arabs, Asians, and Mixed were reluctantly collapsed to avoid excluding these responses from the analysis. Additionally, nine participants were excluded due to >70% missing responses.
Results
Social and structural stigma results (questions 1-5)
Around half (46%) of participants expressed agreement that baldness is socially stigmatized. Of 405 advertising stigma answers, 50% were categorized as indicating it was negative for balding men by undermining acceptance and inappropriately pushing “treatments” onto them (e.g. “Undermining confidence”; “They seem to either be too expensive or they don’t work at all. This kind of advertising promotes more stigma around baldness”). In contrast, 20% of responses were categorized as indicating adverts benefited bald men primarily by normalizing beneficial treatments (e.g. “Gives them hope if they don’t like the idea of being bald”; “It helps raise awareness that possible treatment for balding exists”).
Of 307 cultural stigma answers, 68% indicated culture was negative including by distressing, stigmatizing and inappropriately pushing “treatments” onto bald men (e.g. “That we should be ashamed”; “…mainstream media always, portrays [bald] men as insecure and oddly fat & addicted to getting their hair back, which might explain why men hate balding.” In contrast 16% (n = 49) indicated culture was beneficial by associating baldness with positive traits (e.g. as intelligent and masculine) and normalizing it (e.g. “They are portrayed as rich, old and smart” and “I think culture has been moving in the direction of inclusiveness and people with hair loss are not suffering too much these days”). Table 2 presents further details including indicative participant quotes and the proportion of ambiguous or unclear answers.
Participants, on average, indicated that 50% (SD = 27.43) of the 5 baldness information sources had commercial influences and 71% of participants had seen baldness advertising. Table 1 presents the full results.
Internalized stigma results (questions 6-9)
Around half (44%) expressed agreement that baldness has no advantages. Most participants responded neutrally or with disagreement to the QUALAGA measure indicating minimal distress and internalized stigma (N = 349, M = 2.88, SD = 0.88). See Table 1 for the full responses.
Of 248 current impact answers, 52% were categorized as not distressed nor impacted by baldness stigma (e.g. “Non[e], it was just a laughing matter to me nothing serious” and “I accept it with no problem”) whilst 45% were categorized as distressed and concerned by baldness stigma (e.g. “In my confidence when talking to women” and “It brings insecurity”). Of 244 anticipated impact answers, 60% were categorized as expecting baldness to have minimal or no impact in the future (e.g. “I don’t think it will have a notable impact” and “I think (and hope) I will manage to accept it”). In contrast 31% were categorized as expecting baldness to be distressing and stigmatizing in the future (e.g. “depression” and “I will look much older”).
Stigma consequence results (questions 10 and 11)
Of 256 current baldness response answers, 42% were broadly categorized as accepting baldness (e.g. “Nothing, I just dealt with that” and “Accept that I am grown and these things happen”) and 57% were categorized as combatting baldness (e.g. “Try some medicine” and “Grow my hair longer to cover the bald parts”). Of the 249 anticipated response answers, 50% were categorized as anticipating accepting their baldness (e.g. “nothing” and “not really, just accepting it”) and 44% were categorized as expecting to combat baldness using anti-baldness products or to conceal it in the future (e.g. “most definitely will do a transplant if I have the money by then” and “Yes, some sort of medical treatment.”).
Stigma responses differences by “race,” global nationality and experimental group
Chi squares and T Tests revealed no significant differences by “race” (White, Black, Hispanic/Latinx, Arab/Asian/Mixed), global nationality (Northern and Southern) and condition (Control, Medicalized and Demedicalized) on the great majority of stigma responses (e.g. p’s > 0.5, z scores < 1.96). There were just seven exceptions, detailed below.
Group differences in anti-baldness advert exposure
More Global Northern participants reported being unexposed (37%) to wig advertising compared to Global Southern participants (20%; χ2 (1) = 12.59, p = 0.000, z score = 2.1). Fewer Black participants reported being unexposed (14%) to wig advertising compared to other race groups (25–39%; χ2 (3) = 13.59, p = 0.004, z score = −2.3). More Black participants reported being exposed (79%) to SMP advertising compared to other race groups (51–62%; z score = 2.0) and vice versa (χ2 (3) = 15.56, p = 0.000, z score = 2.4).
Group differences in baldness current responses
More Black participants indicated they accepted their baldness (67%) compared to other “races” (30–39%; z score = 2.6) and relatedly, fewer indicated they were attempting to combat (33%) compared to other “races” (61–67%; χ2 (3) = 15.50, p = 0.000, z score = −2.3).
Group differences in baldness social stigma
Fewer medicalized condition participants disagreed that baldness was socially stigmatized (27%) compared to participants in the control (37%) and demedicalized (41%) conditions (χ2 (2) = 13.20, p = 0.001, z score = − 2.2)
Discussion
Impacted: Social, structural, and internalized baldness stigma
Participants’ responses can be divided into two sets. The first set of responses indicated baldness stigma impacts. Specifically, these responses reported social and structural stigma, internalization of stigma and consequently combatting baldness usually through “treatments.”
Bald men impacted by stigma are responding to a reality that others have also recognized. For example, hair loss practitioners (N = 34) recently indicated baldness was structurally- (86%) and socially- stigmatized (50%; Jankowski and Kranz, 2024). Evidence also shows baldness can be socially stigmatized as less attractive and dateable (Henss, 2001; Kranz et al., 2019). Bald stigma occurs through commercial pressures in culture and advertising. Participants estimated that 50% of baldness “culture” (e.g. social media) was commercially influenced and 71% had been exposed to baldness advertising. The distinction between advertising and culture, when it comes to baldness, is blurred. Harvey (2013) identified this across eight popular baldness websites and forums where anti-baldness products featured explicitly (e.g. in the website mastheads) Anti-baldness product promotion is often covert. For example, reviews of hair loss research tend to ignore the commercial biases and the uncritical promotion of commercial anti-baldness products in the studies being reviewed (Huang et al., 2021; Tucker, 2009). As such balding men in this study underestimated commercial influences in research (45%) as have hair loss practitioners (25%; Jankowski and Kranz, 2024). Yet when commercial biases are assessed between 50% and 78% of studies are found to have them (Behbahani et al., 2020; Gupta and Ivanova, 2020; Jankowski and Frith, 2022; Li et al., 2019).
For balding men who are distressed and internalize stigma, psychosocial support is needed. Unfortunately, like dermatological psychology support generally, this is sorely lacking (All Party Parliamentary Group on Skin, 2020). Baldness’ structural stigma needs combatting. Greater transparency and regulation of research commercial biases are thus needed. Commercial influences are inarguably inappropriate for the benign condition of baldness. As some participant suggested, baldness is structurally- and socially- stigmatized as a devastating disease primarily through pharmaceutical, cosmetic and surgical product promotion (Harvey, 2013; Jankowski, in prep.).
Stigma consequences: Product use
Baldness stigma has consequences. About 40% of the bald men who participated in this study resort to anti-baldness products currently or anticipated doing so in the future. This is higher than previous research has found (5–30%; Alfonso et al., 2005; DeMuro-Mercon et al., 2000; Kranz, 2011; Tang et al., 2000). The anti-baldness marketing industry has increased in profits and size since these previous studies were conducted (Relevant Research, Inc, 2022) which may explain our heightened results. Bald men who use “treatments” are more distressed and report more stigma internalization than those who do not (Enitan et al., 2022; Gosselin, 1984; Han et al., 2012; Kranz, 2011).
Using anti-baldness products may be a maladaptive response for bald men. Products may result in further internalization of stigma and other harms not least because of limited efficacy. Two meta-analyses (Adil and Godwin, 2017; Gupta et al., 2018) have found that popular anti-baldness products including finasteride, minoxidil, and dutasteride worked better than placebo and produced some hair regrowth (averaging around 10–20% of scalp density). Unfortunately only hair regrowth of >80% density is rated as cosmetically meaningful (Wyrwich et al., 2023). For modest success, anti-baldness products arguably run high risks. Harms of finasteride, minoxidil, and transplants collectively include scalp infections, heart attacks, sexual dysfunction, and depression (Gupta et al., 2018; Pompili et al., 2021; Satoh et al., 2000). Indeed, 54 countries have issued finasteride safety warnings as of March 2023 (PFS Foundation, 2022).
Participants baldness’ responses may be hampered by anti-baldness stigma. Moynihan et al. (2002: 900) argues that individuals can only give informed consent to any “treatments” (i.e. anti-baldness products) if they are fully “informed about medicalization and disease mongering.” Evidence-based guidance showing the efficacy, safety and commonality of different baldness responses (including acceptance) is needed. Balding men’s responses should be informed by such guidance including when consulting hair loss practitioners (who themselves wish to have more evidence-based baldness guidance; Jankowski and Kranz, 2024).
Resistant: Accepting baldness and resisting stigma
In contrast to those impacted by baldness, another set of participant responses showed resistance to internalized, social, and structural-baldness stigma. For example, most participants did not exhibit baldness distress or internalize stigma quantitatively via the QUALAGA (Razum and Vukasović Hlupić, 2022). Slightly more, but still fewer than half, indicated baldness distress qualitatively (45%). Similar QUALAGA responses were found in another non-biased, sample of balding men (Razum and Vukasović Hlupić, 2022). As mentioned, previous research into internalized stigma and distress are based on predominantly those bald men who are using “treatments” and thus report heightened results (e.g. in Lulic et al., 2017). Our results cohere with more systematic assessments of baldness distress and internalized stigma. Specifically, Huang et al. (2021) meta-analyzed 41 studies with 6,148 bald men. Results revealed on average a negative, moderate, impact on quality of life but no depression or self-esteem issues. Frith and Jankowski (2024) analyzed 37 psychosocial impact studies with 10,620 bald men. Of 28 reasonable-quality assessments of baldness distress (validated and with norms/cut off scores), 12 (43%) indicated that balding men had worse distress, and 16 (57%) indicated that balding men had average or less distress, compared to non-bald/haired men. On average then the psychosocial impact has been previously exaggerated and is in reality moderate, not severe (Frith and Jankowski, 2024; Huang et al., 2021).
Furthermore, previous research has found bald men’s resilience to anti-baldness culture exists in small pockets on hair loss forums (Jankowski et al., 2021a) and even through baldness acceptance groups (Baldwin, 2005). Indeed, the “hyperconnectivity” (Cockerham, 2023: 6) of health digitalization means online support networks for balding men are easier to establish. Funding and resources to ensure such groups remain independent and can foster acceptance are needed.
Participants wish to resist baldness stigma. Specifically, more participants (55%) on average reported anticipating acceptance and not combatting baldness in the future. This was higher than those anticipating distress (31%) or combatting baldness in the future (44%). Evidence shows over time baldness experiences can improve and initial fears of discrimination are worse than the realities of baldness (Gosselin, 1984). Furthermore, social baldness stigma is surmountable once other relevant information about a perceived person is available (Kranz et al., 2019) and may not lead to any social discriminatory behavior (Sigelman et al., 1990). Experimental research has found balding politicians are just as likely to be voted for as their haired counterparts for example (Sigelman et al., 1990). Baldness stigma should also be considered relative to other stigma forms. For example, there have never been laws discriminating against bald men though there have been against long haired men (Baldwin, 2005) and people can hold negative perceptions about a range of appearance attributes with some (fatness, visible disability) being more negatively interpreted than others (such as baldness and glasses). Finally, any disadvantages baldness stigma is said to cause can be countered by advantages. This ranges from increased vitamin D through scalp sun exposure, higher ratings of leadership skills, and an increase in empathy (Jankowski, in prep.). Whilst these advantages might be considered minor; so too might baldness disadvantages. Baldness may best be considered as benign.
“Race”, global nationality, and baldness
There were minimal differences in stigma responses by “race,” global nationality and experimental condition in our sample, thus generally the sample was treated as a whole with a few exceptions. Relative to other participant groups, fewer Black and Global Southern participants reported being unexposed to wig and SMP adverts. Black participants were also more likely to accept rather than combat their baldness. Such results might be an artefact of our sample and a limitation of the imperfect Global -North and -South division classification. Notably, half (50%; N = 88) of those classified as Global Northern were from Poland and Portugal which may differ to other Global Northern countries including the UK, Canada, and North America (N = 42).
Alternatively, Global Southerners’ slightly greater or equal exposure to anti-baldness advertising in this study rebuts the idea that baldness “treatments” are limited to the Global North. Previous research concurs. The International Society of Hair Restoration Surgeons (Relevant Research, Inc, 2022) suggests the global number of surgical and non-surgical hair restoration procedures was 2.2 billion in 2021. It estimates the majority of these are in Asia/Australia (41%), the US/Canada (18%), the Middle East/Africa (17%), Europe (13%), and Mexico/Central-/South- America (10%). These approximate categorizations do suggest that at least a third to half of hair restoration procedures occur in the Global South emphasizing the global reach of anti-baldness products.
We found Black participants indicated more acceptance relative to other “races.” This finding needs further exploration. Across “race” groups, responses were very similar. We are reluctant to assert Black participants are advantaged or protected from baldness stigma noting that intersecting stigmas (e.g. relating to “race” and baldness) may produce complex stigma responses (as in the case of HIV stigma for Black gay men; Earnshaw et al., 2021). Notably Afro-textured hair that is associated with Black people is already stigmatized so Black people’s experience of hair loss may be more complex and reflect a stigma ceiling effect than an “easier” experience in relation to their hair (loss; Clarke-Jeffers et al., 2024).
Baldness stigma theorization
Based on this study’s results and the results of two additional studies (Kranz et al., 2023; Razum et al., in prep.) we propose a theoretical model (Supplemental file: Figure 1: A proposed theoretical model explaining different influences on the level of baldness distress and on the willingness to accept or combat baldness) delineating the different consequences of baldness stigma including responses (willingness to accept baldness or to combat baldness). We propose that the level of internalized baldness stigma and distress influences baldness responses. In turn, internalized stigma may be slightly influenced by psychological traits (e.g. perfectionism; Kranz et al., 2023) and significantly worsened by baldness social and structural stigma. These pressures also influence the responses directly. Thus, a balding person may become increasingly distressed primarily due to social and structural baldness stigma and subsequently pushed to combat their baldness using “treatments” that are widely advertised. The impact of anti-baldness advertising on responses and potentially also internalized stigma may be weakened by messages of baldness acceptance/anti-medicalization, experimental evidence suggests (Razum et al., in prep.).
Limitations and strengths
Our sample is the first internationally and racially diverse, non-product seeking, sample of bald men independently studied before. This was facilitated via Prolific and our use of neutral language in recruitment (e.g. to assess baldness -experiences rather than -distress). Prolific may produce more reliable and diverse participant data relative to other online participation platforms (Adams et al., 2020) but it is not without limitations. This includes potential biases from those who use research platforms versus those who do not. Future research is needed to continue recruiting representative samples of balding men including those outside of Prolific. Due to the prior methodological limitations via market-research surveys in the field, apart from the QUALAGA (Razum and Vukasović Hlupić, 2022), we were unable to use standardized established measures having to self-construct them instead. The broader project incorporated an experimental manipulation of medicalizing baldness information (~350 words). The experimental impacts were assessed with measures specifically designed to assess their impacts and are reported elsewhere (Razum et al., in prep.). This study’s participant responses around stigma did not differ due to the experiment with one singular exception. Specifically, medialized condition participants reported baldness was more socially stigmatized. However, as this was the only difference and there were an equal number of participants randomized into each condition (across “racial” and global nationality groups), our analysis of the stigma responses were treated as a whole. We assessed participants stigma experiences including their experience of structural stigma (oft neglected where stigma research focuses on individual and social forms; Stangl et al., 2019). Nonetheless validated and qualitative measures of stigma are needed in future especially due to the conceptual overlap of stigma in the health field. This requires greater clarity though may also reflect the “messy and entangled nature of people’s lived experiences” (Livingston and Boyd, 2010: 2157). Finally, some categorizations are tentative. Three percent of participants indicated their current response to baldness was a dietary or lifestyle change, for example. These were classified as combatting responses. Yet bald men may undergo lifestyle changes not to distract from their baldness but from a greater sense of liberation in personal style. The tentativeness of these categorizations and multiplicity of bald men’s motivations are thus emphasized. Qualitative interviews, focus groups and advert-elicitation methods may be particularly useful in future.
Reflexivity
As authors, we have a personal and professional insight into the topic. Each of us has independently researched baldness experiences, before collaborating here. We are aware that baldness is a common experience but an overlooked topic in psychology. From a professional perspective, 10 years ago the first author read baldness research during his body image PhD, observing regular commercial funding disclosures. Research challenging psychology’s facilitation of commercial determinants of health (e.g. smoking; Craig et al., 2021; Pelosi, 2019) subsequently shaped this study’s focus and design. Personally, all three authors are White, European, men who have experience of baldness. Our responses differ to it (ranging from shaving/acceptance to concealment) as does the stigma we have experienced. We all aim to be mindful that our own social locations (in “race,” sexuality, global nationality) shape those insights. For example, two of us are gay and suggest homophobia increases baldness stigma experiences via increased appearance pressures. One of us is British, another German and another Croatian. Whilst we are all Globally Northern, we are mindful that Croatia (like other Southeastern countries in Europe) has a significantly lower gross domestic product, and this has emphasized to us how the Global North/South is an imperfect proxy only.
Conclusion
Baldness’ commonality and benign status belies its pervasive stigmatization and medicalization as a disadvantaged disease. Our international and racially diverse sample suggests baldness experiences subsequently come in two-halves. Responses indicated about half of bald participants were impacted by structural and social baldness stigma, had internalized it and were consequentially combatting it. Another approximate half indicated not internalizing baldness stigma and consequentially accepting it. As such bald men face two routes forward. One of acceptance and psychological ease on something difficult to reverse and the other a journey of limited efficacy and potentially hazardous “treatments” for something physically benign. Resources to support men to resist pervasive structural and social baldness stigma and to make evidence-based decisions about “treating” or accepting baldness are recommended.
Supplemental Material
sj-docx-1-hpq-10.1177_13591053241259730 – Supplemental material for Men’s baldness stigma: A mixed methods international survey
Supplemental material, sj-docx-1-hpq-10.1177_13591053241259730 for Men’s baldness stigma: A mixed methods international survey by Glen S. Jankowski, Dirk Kranz and Josip Razum in Journal of Health Psychology
Footnotes
Acknowledgements
The authors wish to thank the participants and our institutions, particularly Leeds Beckett University’s Center for Psychological Research, for supporting this work.
Author contributions
GJ, DK, & JR. Formal Analysis: GJ. Funding Acquisition: GJ. Supervision: GJ, DK, & JR. Investigation: GJ, DK, & JR. Methodology: GJ, DK, & JR. Writing – original draft: GJ. Writing – editing and revising: GJ, DK, & JR.
Data sharing statement
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no external financial support for the research, authorship, and/or publication of this article.
Ethics approval
Ethical approval was gained from the lead author’s institution (LREC 29-MAY-20).
Informed consent
Informed consent for the survey was gained.
Supplemental material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.