
Abstract
This study aimed to evaluate treatment necessity, treatment concern, and willingness to engage in decisional trade-offs in the context of treatment escalation decision-making. Participants (n = 147) recruited online were randomized to read a vignette about escalating care in psoriasis in a 2 (high treatment concern vs moderate treatment concern) × 2 (high perceived treatment necessity vs moderate perceived treatment necessity) design. High treatment concern was associated with choosing to defer treatment escalation and being unwilling to engage in decisional trade-offs if disease risk changed. Results highlight the importance of treatment concern and willingness trade-off in treatment escalation decision-making.
Patients are the primary actors in their own medical care. Shared decision-making is a core component of patient-centered care (Voshaar et al., 2015). Decisions regarding treatment escalation represent a common breakdown in the process of shared decision-making. Treatment escalation is critical in many chronic diseases where an increase in treatment intensity may be required to decrease symptom burden, slow the progression of disease, or improve quality of life (Loudon et al., 2014). While patients may decide not to escalate treatment for many reasons (Donovan and Blake, 1992), differences in patients’ and physicians’ thresholds to initiate or change treatment are a prevalent explanation (Fraenkel et al., 2007; Loudon et al., 2014). Failure to follow evidence-based recommendations to escalate treatment is associated with poor patient outcomes across many diseases (Fraenkel and Cunningham, 2014; Hollon et al., 2014; Smith and Hillner, 2001). Thus, in order to improve uptake of evidence-based recommendations, it is important for psychologists working in medical settings to understand how patients evaluate the relationship between their disease and the need to escalate treatment.
The Necessity-Concerns Framework suggests that patient perceptions regarding need for treatment (perceived treatment necessity), and perceptions regarding the burden of potential adverse consequences of treatment (treatment concern), drive patient engagement with, and adherence to, medical treatments (Horne and Weinman, 1999). Two recent meta-analyses (Foot et al., 2016; Horne et al., 2013) have demonstrated that higher perceived treatment necessity (correlation = 0.17, 95% confidence interval (CI) = 0.14–0.10; odds ratio (OR) = 1.742, 95% CI = 1.569–1.934, respectively) and lower treatment concern (correlation = −0.18, 95% CI = −0.21 to −0.15; OR = 0.502, 95% CI = 0.450–0.560, respectively) have been associated with higher rates of adherence across numerous chronic diseases, including rheumatoid arthritis, asthma, human immunodeficiency virus, and type 2 diabetes mellitus.
The majority of research evaluating the Necessity-Concerns Framework has evaluated relationships between patient perceptions regarding a treatment option they have already agreed to take and adherence to that treatment (Horne et al., 2013). In contrast, treatment escalation is a decision made at a single point in time, ideally using shared decision-making with one’s provider, which precedes medication adherence. Although the Necessity-Concerns Framework still provides some guidance in this context, individual differences that contribute to decisions regarding treatment escalation are likely to differ from individual differences that account for variation in medication adherence. In particular, recent qualitative evidence suggests that the decision regarding treatment escalation leans heavily on the willingness to engage in decisional trade-offs (consider the pros and cons of treatment; Fraenkel et al., 2015b). This grounded theory qualitative study evaluated how people with rheumatoid arthritis make decisions regarding escalating treatment from a non-biologic to biologic medication (Fraenkel et al., 2015b). Rheumatoid arthritis was chosen as a case study because lower than expected rates of treatment escalation from non-biologic to biologics have been well-documented, and delays in treatment result in irreversible progression of the disease (Singh et al., 2012). Non-biologic medications have been widely used for decades and have well-established risk profiles; in contrast, biologic medications are relatively newer medications that are very effective but carry risks of rare but more serious complications. People with rheumatoid arthritis who met objective criteria for treatment escalation completed a stated preference survey, during which they were asked to rate hypothetical pairs including the specific risks and benefits associated with staying with the status quo versus starting a biologic (e.g. ability to work, risk of infection). During the task, participants were instructed to think aloud as they rated trade-offs between two competing attributes.
Several important findings emerged from this study. First, many patients with rheumatoid arthritis who met objective criteria for treatment escalation were not willing to engage in decisional trade-offs regarding treatment escalation. These patients entered the task with their minds already set on either escalating treatment (start the new medication) or maintaining the status quo (continue on their current medication) and did not consider the risk–benefit information presented. In other words, these patients were not truly engaging in a decisional balance; they were unwilling to consider the pros and cons for treatment escalation, weighing the relevant information both for and against treatment escalation, prior to making a decision. Thus, this study identified an important proximal outcome in studies evaluating patient decision-making in treatment escalation: in order to make good choices regarding treatment escalation, patients must first have willingness to engage in decisional trade-offs.
Second, this study extended the previous work evaluating the Necessity-Concerns Framework to the context of escalating treatment. As in the previous medication adherence literature, treatment concern (the patient’s concern about the potential negative impact of treatment) and perceived treatment necessity (the patient’s concern about the negative consequences of disease progression) influenced patient choice regarding treatment escalation. This qualitative study further found that treatment concern and perceived treatment necessity together influenced willingness to engage in decisional trade-offs. Among patients who meet objective criteria to escalate treatment, moderate levels of both treatment concern and perceived treatment necessity corresponded with willingness to weigh the pros and cons associated with escalating treatment. On the other hand, very high or very low perceived treatment necessity corresponded with unwillingness to engage in decisional trade-offs: patients with very high levels of perceived treatment necessity described strongly preferring to escalate treatment, while patients with very low levels of perceived treatment necessity described strongly preferring the status quo (deferring treatment escalation). Moreover, further, perceived treatment necessity appeared to interact with treatment concern: most patients with high perceived treatment necessity strongly preferred to escalate treatment; however, those who also had high treatment concern preferred not to escalate treatment.
These findings were identified in a single qualitative study among people with rheumatoid arthritis and must be evaluated empirically. Furthermore, individual differences among patients could impact decision-making regarding treatment escalation. In particular, age and numeracy have demonstrated strong relationships with patient decision-making regarding medical treatment options in the existing literature. Higher age is associated with poorer efficiency in decision-making tasks, but improved experience-based reasoning, both of which are relevant in medical decision-making (De et al., 2012; Peters et al., 2008). Low numeracy is associated with distortion of risk–benefit analysis and a higher effect of competing, irrelevant information on decision-making; people with low numeracy are less likely to follow medical recommendations, access treatments, and may even have poorer medical outcomes, compared to people with high numeracy (Peters et al., 2006; Reyna et al., 2009).
In summary, little is known about how patients make decisions regarding treatment escalation. The Necessity-Concerns Framework provides a starting point for evaluating treatment escalation but a qualitative evaluation of treatment escalation in patients with rheumatoid arthritis suggests that (1) many patients are not willing to engage in decisional trade-offs concerning treatment escalation and that (2) patient willingness to engage in decisional trade-offs regarding treatment escalation and decisions about treatment escalation are influenced by perceived treatment necessity and treatment concern. Empirical evidence is needed to provide “proof-of-concept” that the key component identified in the qualitative research (willingness to engage in decisional trade-offs) is indeed involved in decision-making processes regarding treatment escalation. This study was designed to manipulate perceived treatment necessity and treatment concern to evaluate whether Necessity-Concerns variables are empirically associated with willingness to engage in decisional trade-offs in a treatment escalation situation. In clinical populations, perceived treatment necessity and treatment concern are necessarily confounded by treatment experience; therefore, we set out to evaluate these relationships in a non-clinical population using a vignette disease that (1) had a clear decision point for treatment escalation, (2) was relatively unfamiliar to a non-clinical sample, and (3) in which we were able to achieve manipulation of perceived treatment necessity and treatment concern. Psoriasis, an itchy or painful dermatologic condition characterized by treatment escalation from topical creams to injection, was selected after several rounds of pilot testing. This study aimed to (1) empirically evaluate the relative contributions of perceived treatment necessity, treatment concern, and their interaction on decisions regarding escalation of treatment and willingness to engage in decisional trade-offs and (2) evaluate individual differences, including age, numeracy, and education as moderators of these effects. Hypotheses were as follows:
The combination of high perceived treatment necessity and high treatment concern will be associated with higher odds of deferring treatment compared to high perceived treatment necessity and moderate treatment concern.
The combination of high perceived treatment necessity and moderate treatment concern will be associated with higher odds of choosing to treat compared to moderate perceived treatment necessity and treatment concern.
High perceived treatment necessity will be associated with lower willingness to engage in decisional trade-offs; high treatment concern will strengthen the relationship.
High treatment concern will be associated with lower willingness to engage in decisional trade-offs.
Methods
Study development and pilot studies
Population
We chose to sample a non-clinical population, rather than a specific clinical population, because we hoped to establish proof of concept from a previous qualitative study using manipulation of Necessity-Concerns Framework variables in the context of treatment escalation; manipulation of perceived treatment necessity and treatment concern in an existing patient population is not feasible due to the influence of personal experiences and expectations. Participants were recruited on the Amazon Mechanical Turk web-based portal. This portal is increasingly being used in psychological research where individuals can participate in surveys for compensation. The Mechanical Turk population is well-characterized: Mechanical Turk samples tend to be more demographically diverse than standard Internet samples and substantially more diverse than college samples typically used in psychology samples (Buhrmester et al., 2011). Therefore, we considered the Mechanical Turk population superior to a college student population for this proof-of-concept study. Studies have demonstrated that Mechanical Turk samples perform better than college samples on attention checks and have larger responses to manipulations (Hauser and Schwarz, 2016), such as those used in this study. Empirical evaluation of Mechanical Turk sample characterization data suggests that individuals who choose to participate in studies using the Mechanical Turk platform are internally motivated and produce psychometrically sound data (Buhrmester et al., 2011). Furthermore, we restricted the study to individuals with a “master” designation, a subgroup of participants who have demonstrated a record of accurate and consistent performance on tasks completed within the Mechanical Turk portal; previous research has demonstrated that participants with a high reputation within the Mechanical Turk site produce higher quality data and fail attention checks at lower rates than participants with a low reputation (Peer et al., 2014). Finally, we restricted the study to individuals who completed the survey from an IP address located within the United States because (1) we are most interested in evaluating whether willingness to engage in decisional trade-offs appears to be a potential component within the Necessity-Concerns Framework in the country in which the qualitative research was conducted and (2) Mechanical Turk participants from the United States have demonstrated higher data quality than Mechanical Turk participants from other countries (Litman et al., 2015).
Vignette disease
Because we sampled a non-clinical population, we set out to choose a scenario that could be imagined as personally relevant and that would enable us to manipulate both disease and treatment concern. Therefore, we set out to choose a disease state for the vignette that had a clear treatment escalation decision point, was relatively uncommon, and could be experienced by people of varying ages and backgrounds. We did not want participants to have a great deal of information about the disease state prior to being presented with the vignette. This ruled out several disease states that had already been evaluated in clinical research in the Necessity-Concerns Framework literature (e.g. rheumatoid arthritis or type 2 diabetes mellitus). We iteratively piloted several versions of the vignettes to attempt to achieve this balance. The first formal pilot study (n = 20) attempted to manipulate disease and treatment concern in a vignette describing being diagnosed with an uncommon form of cancer; however, the disease evoked such strong dread that we were unable to obtain moderate scores on perceived treatment necessity. With an additional two iterative rounds of piloting (ns = 14–16), psoriasis was the eventual choice for the disease model for the vignette because it was unfamiliar to the majority of participants, did not evoke a strong emotional response, and we were able to manipulate both perceived treatment necessity and treatment concern. Psoriasis is a dermatologic condition in which skin cells reproduce too rapidly and cause extra cells to build up on the skin surface (Raychaudhuri et al., 2014). Common symptoms include scaling and/or red patches that are often itchy or painful. Psoriasis is a relatively uncommon disease (US population prevalence ranges from 0.51% to 1.23%) with a wide range of severity in disease presentation (Takeshita et al., 2015). In psoriasis, treatment escalation occurs when people transition from using topical creams to oral medications or injections used to treat the disease. In the final and largest pilot of the vignette (n = 50), psoriasis did not evoke uniformly strong negative reactions, allowing for manipulation of both perceived treatment necessity and treatment concern.
Manipulation
We revised the manipulation of perceived treatment necessity and treatment concern through piloting of both visual images and written manipulation, such that both perceived treatment necessity and treatment concern manipulations achieved similar levels of reported concern about disease (perceived treatment necessity) and medication (treatment concern) upon manipulation check.
Sample size
A priori power analyses conducted on a pilot sample of 50 participants from the MTurk site indicated a sample size of 94 for a power of .95 to detect interactions between perceived treatment necessity and treatment concern. A sample of 150 was indicated for a power of .80 to detect a medium effect for a continuous moderator; therefore, we set out to collect 150 participants.
Participants
Inclusion criteria were as follows: (1) aged 18 and above, (2) the ability to read English, (3) participating on the Mechanical Turk site with a “master” designation, and (4) from the United States. A total of 152 participants completed the study. Of these, 147 participants utilized IP addresses from within the United States and were therefore included in the analyses.
Design
This is an experimental study evaluating the impact of perceived treatment necessity and treatment concern on treatment choice and willingness to engage in decisional trade-offs in the context of a vignette regarding treatment escalation for psoriasis. Participants were randomized into a 2 (high perceived treatment necessity vs moderate perceived treatment necessity) × 2 (high treatment concern vs moderate treatment concern) factorial design (Figure 1). Perceived treatment necessity and treatment concern were manipulated in a vignette in which participants were asked to imagine that they were given a diagnosis of psoriasis by their doctor and asked to make a decision regarding whether to escalate treatment (Figure 2). Dependent variables of treatment choice (whether or not the participant decided to escalate treatment) and willingness to engage in decisional trade-offs (how willing would the participant be to reconsider his or her decision if the risks changed) were then assessed (Figure 1).
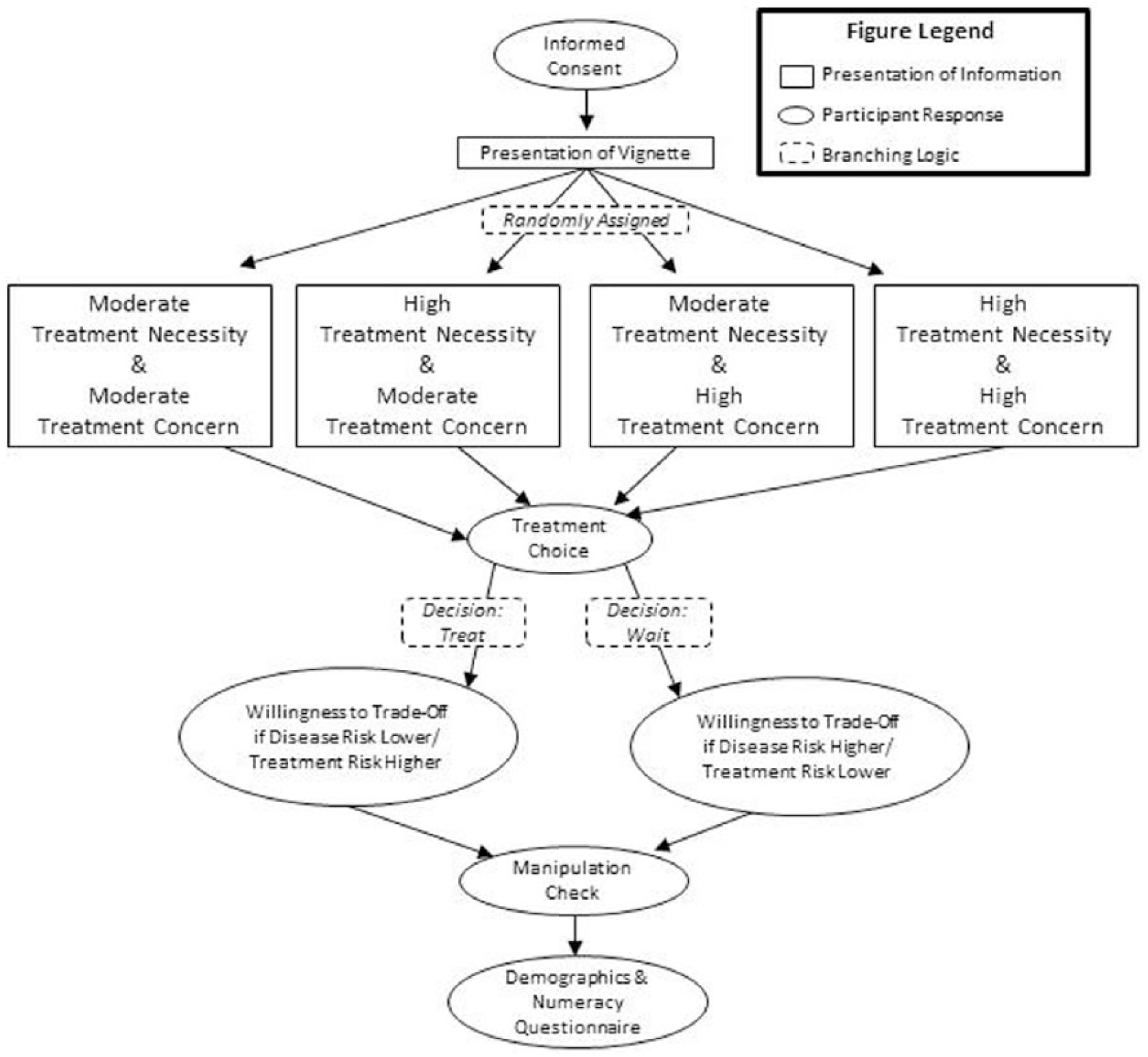
Study flow.
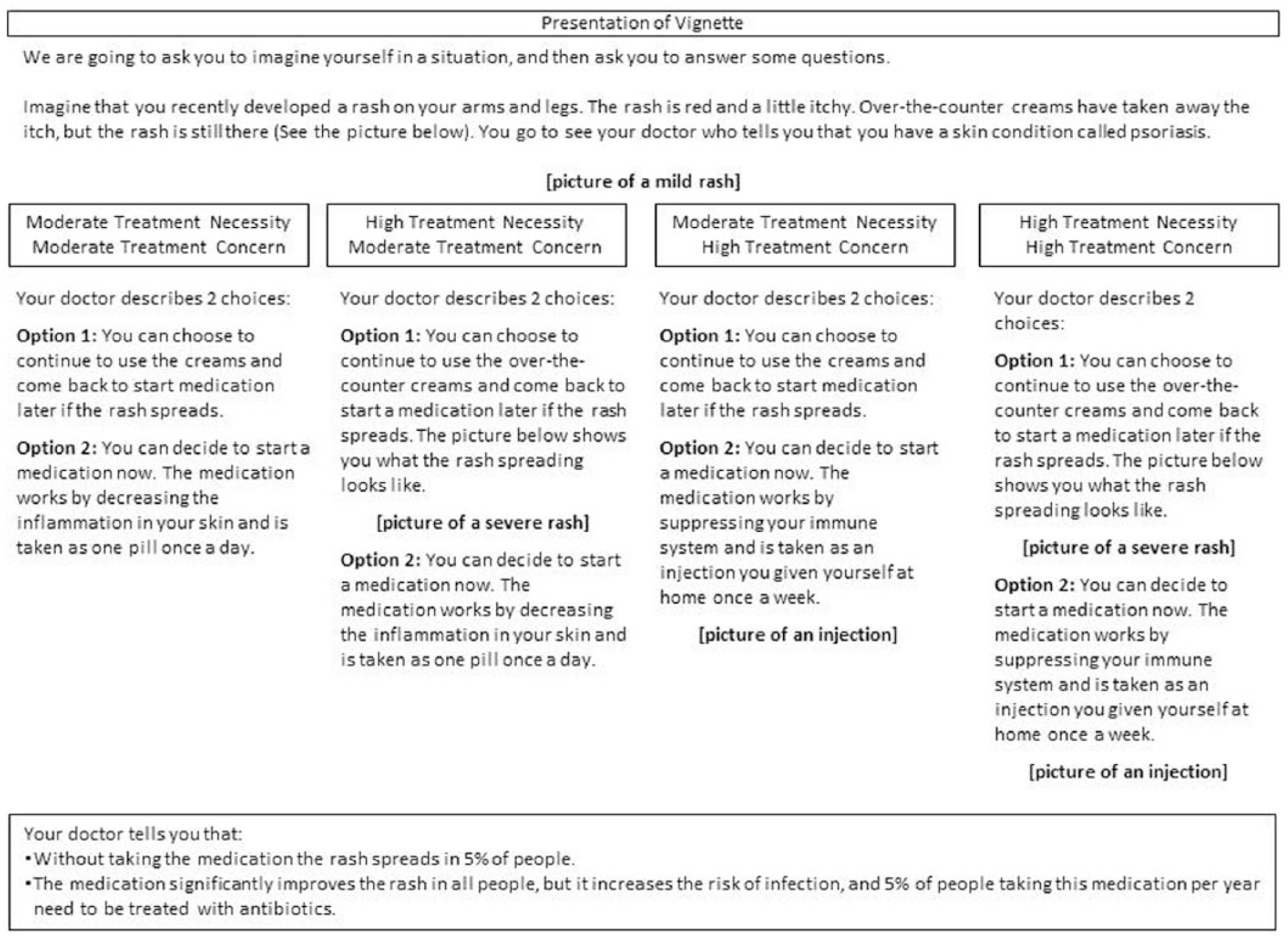
Description of the vignette, including the four randomized conditions.
Materials
Demographics
Participants answered demographic questions relating to their age, gender, race/ethnicity, marital status, and the highest grade level completed. For moderator analyses, education was coded as some college or less vs college degree or higher. Perceived overall health status was assessed with the item, “In general, I would say my health is”: with response options on a 5-point scale ranging from excellent to poor, which is similar to other single-item self-rated health items, such as those used in the International Quality of Life Assessment Project (Ware and Gandek, 1998) and the World Health Survey (Subramanian et al., 2010). A single-item measure of experience with the treatment escalation option was developed alongside the vignette, as this was specific to the disease and treatment options presented. Thus, history of self-injecting medication was assessed with the item, “Have you ever given yourself an injection?” and response options of “I am CURRENTLY giving myself an injection,” “I have given myself an injection IN THE PAST YEAR,” and “I have NEVER given myself an injection.”
Treatment choice
Items assessing treatment choice were developed alongside the vignette, as the response options for the treatment choice were dependent on the disease and treatment options chosen. Participants responded to the question, “What do you choose to do?” with one of two tick-box response options: “Start medication now” (indicating the choice to treat) or “Decide not to take the medication at this time, but to wait and see how things go only using over-the-counter creams” (indicating the choice to defer treatment escalation).
Willingness to engage in decisional trade-offs
Items assessing willingness to engage in decisional trade-offs were initially developed using qualitative data from the literature (Fraenkel et al., 2015b) and refined in the pilot testing as they were specific to the vignette disease state and treatment escalation options. To assess willingness to engage in decisional trade-offs if disease risk changed, participants were asked one of two questions: “If the chance of the rash spreading was slightly lower, would you be willing to consider continuing with creams for now?” (if the participant chose to treat) or “If the chance of the rash spreading was slightly higher, would you be willing to consider starting the medication now?” (if the participant chose to defer treatment escalation). Response options were tick boxes indicating “yes” or “no.” To assess willingness to engage in decisional trade-offs if treatment risk changed, participants were asked one of two questions: “If the chance of having an infection was slightly higher, would you be willing to consider continuing with creams for now?” (if the participant chose to treat) or “If the chance of having an infection was slightly lower, would you be willing to consider starting the medication now?” (if the participant chose to defer treatment escalation). Response options were tick boxes indicating “yes” or “no.”
Manipulation check
Manipulation check items were initially developed from the “specific” section of the Beliefs about Medicines Questionnaire (Horne et al., 1999) and refined through pilot testing as they were specific to the disease state and treatment escalation options. As a manipulation check, all participants rated “How concerned are you about the rash?” and “How concerned are you about the medication?” using a 5-point Likert-type scale (1 = not at all concerned and 5 = very concerned).
Numeracy Questionnaire
Participants completed an 8-item scale assessing objective numeracy (Weller et al., 2011). Example questions include, “If the chance of getting a disease is 10%, how many people would be expected to get the disease out of 1000 people?” and “Imagine that we roll a fair, six-sided die 1,000 times. Out of 1,000 rolls, how many times do you think the die would come up as an even number?” This measure was developed using Rasch analysis. The measure has demonstrated adequate internal consistency (α = .71) and convergent validity with other measures of numeracy and expected relationships with demographics.
Procedures
The study occurred in a single setting; participants spent a median of 7.9 minutes completing the study (interquartile range (IQR) = 5.5–10.6 minutes), and all consented participants completed the study. Figure 1 describes participant flow through the study. Participants gave electronic informed consent and then read the vignette described in Figure 2. All participants were given the same introduction, which describes the early stages of psoriasis (developing a rash on arms and legs). Then, participants were randomized to read one of four sets of vignette treatment options in a 2 (high perceived treatment necessity vs moderate perceived treatment necessity) × 2 (high treatment concern vs moderate treatment concern) design (see Figure 2 for the manipulation). Participants were presented with two options: (1) continuing over-the-counter creams or (2) escalating treatment to a medication. When presenting option 1, high treatment necessity was manipulated by including a picture of a psoriasis rash spreading, whereas the moderate treatment necessity condition did not include a picture. When presenting option 2, high treatment concern was manipulated by informing the participant that the treatment involved injected medications that suppress the immune system and providing a picture of an injection, whereas moderate treatment concern was manipulated by informing the participant that the treatment involved an oral medication that decreases skin inflammation. Finally, all participants were given an identical vignette conclusion, which stated probabilities of the disease worsening without treatment and medication side effects.
Participants then completed a single item regarding treatment choice (treat or defer treatment escalation; Figure 1). All participants were then queried about whether they would be willing to engage in decisional trade-offs if the disease risk changed or if the treatment risk changed. Specific willingness to engage in decisional trade-offs questions differed based on treatment choice (Figure 1). Participants who chose to treat were asked whether they would be willing to defer treatment escalation if the risk of getting an infection (a serious side effect from the medication) was higher or if the risk of the disease worsening was lower. Participants who chose to defer treatment escalation were asked whether they would be willing to consider treating now if the risk of getting an infection was lower or if the risk of the disease worsening was higher.
All participants then completed a manipulation check, demographics, and objective numeracy questionnaires (Figure 1; measures described below). Participants in this study were compensated US$ 50 cents following completion of the study. This study was approved by the Einstein IRB (#2014-3401).
Analyses
Randomization check
Relationships between perceived treatment necessity and treatment concern, demographics, and numeracy were examined through t tests (age, perceived health status, numeracy) and χ2 tests (gender: male vs female), race/ethnicity (White vs all else), and education (some college or less vs college degree or higher).
Manipulation check
T tests evaluated the manipulation checks. We expected that average concern about disease would be higher in people randomized to the high perceived treatment necessity compared to people randomized to moderate perceived treatment necessity, but that randomization to the high or moderate treatment concern condition would not impact concern about disease. Alternately, we expected that average concern about medication would be higher in people randomized to the high treatment concern condition compared to people randomized to the moderate treatment concern condition, but that randomization to the high or moderate perceived treatment necessity condition would not impact concern about medication.
Primary outcomes
Logistic regression examined perceived treatment necessity, treatment concern, and their interaction as predictors of treatment choice (treat now vs defer treatment). If the interaction was not significant, it was removed from the model and only main effects interpreted. Two logistic regressions examined perceived treatment necessity, treatment concern, treatment choice, and their interactions as predictors of willingness to engage in decisional trade-offs in two circumstances: willingness to engage in decisional trade-offs if disease risk changed (yes vs no) and willingness to engage in decisional trade-offs if treatment risk changed (yes vs no). In each model, all predictors were entered into the model (perceived treatment necessity, treatment concern, treatment choice, and all two- and three-way interactions); higher order terms were removed if non-significant until all terms were significant or used in higher order interactions.
Moderator analyses
Logistic regression examined the influence of potential moderators (age, numeracy, and education) on significant results from the primary outcome analyses. In each analysis, the potential moderator, perceived treatment necessity, treatment concern (and when appropriate, treatment choice), and their interactions were entered into the model. Higher order terms were removed if non-significant until all terms were significant or used in higher order interactions. Moderation is indicated by a significant interaction including the potential moderator (age, numeracy, or education).
Results
Demographics
Demographics by condition are described in Table 1. The overall mean age was 36.16 (standard deviation (SD) = 11.23) with a range from 20 to 68. Participants were majority White, non-Hispanic (n = 113 (76.9%)) women (n = 78 (53.1%)) with some college (n = 65 (44.2%)) or an undergraduate degree (n = 46 (31.3%)). Approximately half were single (n = 74 (50.3%)) or married/partnered (n = 63 (42.9%)). On average, participants correctly answered 5.02 (SD = 1.45) out of 8 numeracy questions, which is comparable to the mean reported in the community-based and web-panel development populations (Weller et al., 2011), and perceived their health to be “good” or “very good” (M = 3.42, SD = 0.99). The majority of participants (134 (91.2%)) had never given themselves an injection; 10 participants (6.8%) had given themselves an injection in the past, and only 3(2.0%) were giving themselves injections currently.
Demographic characteristics.

GED: General Educational Development; SD: standard deviation.
Manipulation checks
A series of t tests evaluating the manipulation checks by randomization suggested that the manipulation was successful. People randomized to the high perceived treatment necessity group reported higher concern about disease (M = 1.8, SD = 0.8) than those randomized to the moderate perceived treatment necessity group (M = 2.4, SD = 1.0); however, treatment concern group membership was not associated with reported concern about disease (high treatment concern, M = 2.2, SD = 1.0; moderate treatment concern, M = 1.9, SD = 0.9; p = .114). Randomization to the high treatment concern group reported higher concern about treatment than people randomized to the moderate treatment concern group (t = 3.59, p < .001); however, randomization to perceived treatment necessity group was not associated with reported concern about treatment (high perceived treatment necessity, M = 1.8, SD = 0.8; moderate perceived treatment necessity, M = 2.9, SD = 1.2; p = .209). Demographic variables, numeracy, and perceived health were not related to the manipulation (p > .300).
Treatment choice
Effect of perceived treatment necessity and treatment concern
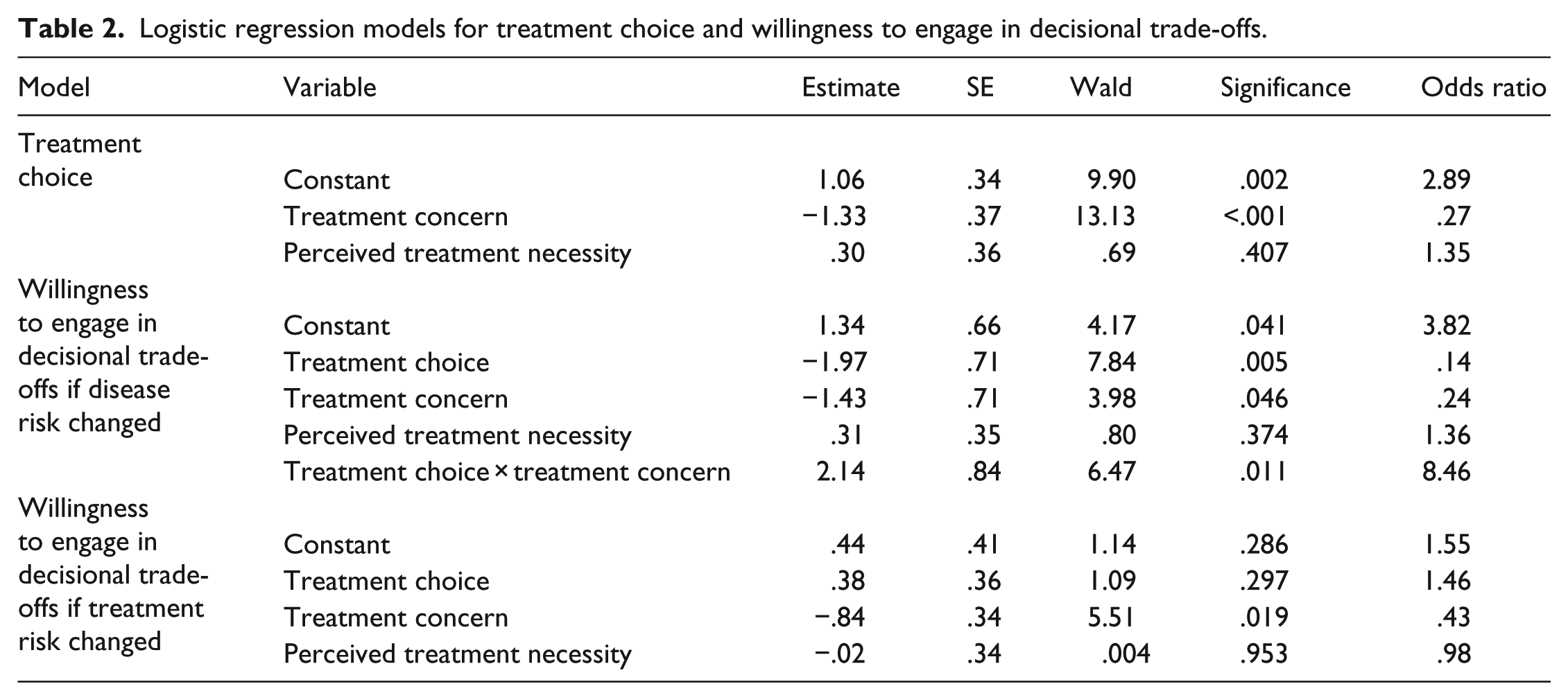
Overall, 90 (61.2%) participants chose to treat, whereas 57 (38.8%) chose to defer treatment escalation. Neither perceived treatment necessity nor the interaction between perceived treatment necessity and treatment concern were associated with treatment choice (ps > .050; Table 2). In contrast, treatment concern demonstrated a significant association with treatment choice: people randomized to the high treatment concern condition chose to defer treatment escalation more frequently than people randomized to the moderate treatment concern condition (OR = 2.89, p = .002; Table 2).
Logistic regression models for treatment choice and willingness to engage in decisional trade-offs.
Effect of age, education, and numeracy
Higher age was associated with choosing to defer treatment escalation (OR = .95, p = .003) but did not moderate the effect of treatment concern on treatment choice (p = .579). Education and numeracy were not significantly associated with treatment choice (ps > .400) and did not moderate the effect of treatment concern on treatment choice (ps > .600).
Willingness to engage in decisional trade-offs
When disease risk is changed
Treatment choice and willingness to trade-off
Treatment choice (OR = .14, p = .005), treatment concern (OR = .24, p = .046), and the interaction between these two variables (OR = 8.46, p = .011) were associated with willingness to engage in decisional trade-offs if disease risk changed. Overall, people randomized to the high treatment concern condition, and those who initially chose to defer treatment escalation, were less willing to engage in trade-off if disease risk changed compared to those randomized to the moderate treatment concern condition and who chose to treat, respectively (Table 2). The interaction between initial treatment choice and treatment concern is illustrated in Figure 3. Among people who chose to defer treatment escalation, a larger proportion of people randomized to the moderate treatment concern condition were willing to engage in decisional trade-offs (81.3%) than people randomized to the high treatment concern condition (51.2%), χ2(1) = 4.31, p = .038; on the other hand, among people who chose to treat, there was no significant difference in the proportion of people willing to engage in decisional trade-offs between people randomized to the high treatment concern condition (55.6%) and the moderate treatment concern condition (38.9%), χ2(1) = 2.42, p = .120 (Figure 3). Neither perceived treatment necessity nor interactions containing perceived treatment necessity were associated with treatment choice (ps > .05; Table 2).

Proportion of participants who were willing to engage in decisional trade-offs if disease risk changed by treatment choice (defer treatment escalation vs treat) and treatment concern (moderate vs high).
Effect of age, education, and numeracy
Higher education was associated with lower willingness to engage in decisional trade-offs if disease risk changed (OR = 0.32, p = .026); furthermore, education moderated the impact of treatment concern on willingness to engage in decisional trade-offs if disease risk changed (OR = 8.69, p = .002). Among people with some college or less, randomization to the high treatment concern condition was associated with lower willingness to engage in decisional trade-offs if disease risk changed; however, among people with a college degree or higher, randomization to the high treatment concern condition was associated with higher willingness to engage in decisional trade-offs if disease risk changed. Education and numeracy are related (t(150) = −3.99, p < .001); these results were unchanged when adjusting for numeracy.
Higher age was associated with lower willingness to engage in decisional trade-offs if disease risk changed (OR = .96, p = .009) but did not moderate the effects of treatment choice (p = .222), treatment concern (p = .135), or the interaction between these two variables (p = .646) on willingness to engage in decisional trade-offs if disease risk changed. Numeracy was not significantly associated with willingness to engage in decisional trade-offs if disease risk changed (p = .642) and did not moderate the effects of treatment concern (p = .895), treatment choice (p = .599), or the interaction between these two variables (p = .418) on willingness to engage in decisional trade-offs if disease risk changed.
When treatment risk is changed
Treatment choice and willingness to trade-off
Initial treatment choice and perceived treatment necessity were not associated with willingness to engage in decisional trade-offs if treatment risk changed (ps > .050; Table 2). People randomized to the high treatment concern condition had lower willingness to engage in decisional trade-offs if treatment risk changed (OR = .43, p = .019; Table 2). No interaction was significant (ps > .050).
Effect of age, education, and numeracy
Age moderated the relationship between treatment concern and willingness to engage in decisional trade-offs if treatment risk changed (OR = .93, p = .027; Figure 4; although age was analyzed as a continuous variable, age is presented with a median split (median = 34) in the figure for ease of interpretation). The negative effect of treatment concern on willingness to engage in decisional trade-offs if treatment risk changed was stronger in older people than in younger people. The main effect of age on willingness to engage in decisional trade-offs if treatment risk changed was not significant in the presence of treatment concern and the treatment concern × age interaction. Higher numeracy was associated with higher willingness to engage in decisional trade-offs if treatment risk changed (OR = 1.40, p = .013); this result was unchanged adjusting for education. However, numeracy did not moderate the effect of treatment concern on willingness to engage in decisional trade-offs if treatment risk changed (p = .388).

Proportion of participants who were willing to engage in decisional trade-offs if disease risk changed by treatment concern (moderate vs high) and age (≤34 vs >34).
Education was not associated with willingness to engage in decisional trade-offs if treatment risk changed and did not moderate the relationship between treatment concern and willingness to engage in decisional trade-offs if treatment risk changed (ps > .500).
Discussion
This study sought to empirically evaluate how perceived treatment necessity and treatment concern impact patient decisions about escalating treatment and willingness to engage in decisional trade-offs about escalating treatment. The results of this study partially supported findings from a previous qualitative study (Fraenkel et al., 2015b). People randomized to the high treatment concern condition were less likely to be willing to engage in decisional trade-offs than people randomized to the moderate treatment concern condition. People randomized to the high treatment concern condition were more likely to choose to defer treatment; however, if a person chose to treat even in the face of high treatment concern, he or she was likely to be willing to re-examine that decision and consider alternative treatment options if the risk of the disease worsening was lowered. On the other hand, if a person with high treatment concern chose to defer treatment (which was the most common choice among people with high treatment concern), he or she was likely to be unwilling to re-examine that decision and consider alternative treatment options if the risk of disease progression was more severe than originally described.
These results suggest that people with high treatment concern are more likely to refuse treatment changes and unlikely to reconsider their decision in light of new information about the risks associated with either the disease or the treatment. Thus, treatment concern effects people’s decisions about treatment escalation and their willingness to reconsider treatment options in the face of new information. These results should be evaluated in observational studies within patient populations to determine whether these experimental findings translate to real-world health settings. Particularly, relevant patient populations (those that include a specific decision point of treatment escalation) should be identified and a measure of willingness to engage in decisional trade-offs developed for these patient populations. Patient populations who are particularly relevant would include rheumatoid arthritis (the escalation to biologic medications) and type 2 diabetes mellitus (the escalation to insulin). If these results are corroborated, efforts to develop interventions to address treatment concern prior to engaging in shared decision-making in relevant patient populations could be warranted.
This study identified age as a significant predictor of both treatment choice and willingness to engage in decisional trade-offs. Results from the study indicate that as age increases, people are more likely to choose to defer treatment and are less willing to engage in decisional trade-offs about their treatment choices. Furthermore, older people with high treatment concern may be even less willing to engage in decisional trade-offs when information about treatment risks change than younger people. Older people use more health care services and take more prescription medications than younger people (National Center for Health Statistics, 2015). Thus, the negative ramifications of treatment concern (e.g. closing people off to engaging in a decisional trade-off about treatment options) may be most evident among older people.
This study found that higher numeracy was associated with higher willingness to engage in decisional trade-offs when information about treatment risk is changed. This result is in keeping with studies demonstrating that subjects with low numeracy tend to perceive more risk, choose less risky options, and prefer to remain with the status quo compared to people with higher numeracy (Fraenkel et al., 2015a; Reyna et al., 2009).
Although the qualitative study suggested that perceived treatment necessity was an important component of willingness to engage in decisional trade-offs, this factor was not a significant predictor of treatment choice or willingness to engage in decisional trade-offs in this study. There are several possible explanations. First, perceived treatment necessity may simply not be a salient predictor of treatment choice or willingness to engage in decisional trade-offs. However, results from the qualitative study found numerous consistent examples of perceived treatment necessity as a starting point for patient decisions regarding escalation of rheumatoid arthritis treatment (Fraenkel et al., 2015b). It is also possible that differences in levels of personal experience with medications versus skin conditions resulted in a more successful manipulation of treatment concern than perceived treatment necessity. Although many people have taken a medication or received an injection at some point in their lives, many people may not have personal experience with a skin condition. We specifically chose a disease condition (psoriasis) that is neither rare nor terribly common. This choice was successful in minimizing the immediate dread associated with other diagnoses piloted (e.g. cancer), allowing us to get a reasonable range of “concern about disease” across participants and a significant effect of the perceived treatment necessity manipulation on the manipulation check. Future studies should consider (1) examining the roles of disease familiarity, personal experience, and emotional arousal in perceived treatment necessity and treatment concern and (2) manipulating perceived treatment necessity in an experimental design using other diseases.
Limitations and future directions
The Mechanical Turk platform was chosen to collect the sample because it is less biased than other available samples (e.g. college students); however, our sample was still more highly educated and had higher rates of people who identify as White, non-Hispanic, and Asian, compared to the general US population (Humes et al., 2011; Ryan and Bauman, 2016). Furthermore, participants on the Mechanical Turk platform have demonstrated internal motivation (Buhrmester et al., 2011) but are also certainly motivated by compensation; however, we attempted to optimize our compensation by offering an amount high enough to encourage high-quality participation but low enough to attract participants who were also intrinsically motivated to participate in the research. Future studies should evaluate willingness to engage in decisional trade-offs in the context of treatment escalation for specific disease states in specific populations in order to develop clinically applicable models of decision-making in these populations.
The conceptual model was developed in a patient sample, whereas this study used a non-clinical, online convenience sample of people in the United States who were not selected for the presence (or absence) of any particular health experience or medical diagnosis. This sample was chosen to minimize the systemic intrusion of current patient experiences in the manipulation. However, there are several limitations associated with this approach. First, the patient role could influence associations between treatment concern and perceived treatment necessity and treatment choice and willingness to engage in decisional trade-offs, which we could not capture with this non-clinical sample. Second, the participants were taking questionnaires online rather than making decisions in a medical office with their provider. The treatment context and provider presence could influence associations between treatment concern and perceived treatment necessity and treatment choice and willingness to engage in decisional trade-offs (Frank and Frank, 1991).
The qualitative study in which the conceptual model was expanded occurred in rheumatoid arthritis patients. It is possible that factors specific to rheumatoid arthritis (disease symptoms, severity, course, and treatment options) influenced the conceptual model, decreasing generalizability to psoriasis or other conditions. Future studies should both qualitatively and quantitatively examine the conceptual model in a variety of diseases, to identify the potential role of disease in relationships between perceived treatment necessity, treatment concern, treatment choice, and willingness to engage in decisional trade-offs regarding treatment choice.
Conclusion
In summary, this article suggests that decisions regarding treatment escalation may be influenced by treatment concern. High treatment concern was associated with choosing not to escalate treatment and unwillingness to engage in decisional trade-offs even when the risk of disease progression was increased or the medication risk was decreased. Future studies should consider assessing willingness to trade-off in disease states with a clear treatment escalation decision point (such as rheumatoid arthritis and type 2 diabetes mellitus) when evaluating the treatment escalation decision-making process and developing interventions to improve patient decision-making regarding treatment escalation.
Footnotes
Acknowledgements
The authors would like to acknowledge the invaluable assistance of Ms Hannah Scholl in data collection for this project.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: E.K.S. has received research funding from the National Institute of Neurological Disorders and Stroke (K23N S096107), the International Headache Academy, and has served as a consultant for GlaxoSmithKline. L.F. has received a career development award from the National Institute of Arthritis and Musculoskeletal and Skin Diseases (AR060231). A.S.G. declares that she has no conflict of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.