
Abstract
Medication adherence (MA) to recommended treatment is a multi-faceted problem and an ongoing challenge for healthcare providers (HCPs) to monitor. This qualitative study with 10 HCPs in Cyprus aims to explore HCPs’ perceptions and strategies used on addressing medication non-adherence (MNA) in patients with chronic conditions. Two main themes emerged from the analysis reflecting the ways that HCPs described their reactions to MNA of their patients: (1) “Relying on information provision to improve MA” and (2) “Trying to understand patients’ perspective.” HCPs reported empathizing with patients and engaging in discussions to understand patients’ perspective and reasons for MNA, so as to explore alternative solutions. Simultaneously, some HCPs reflected that the techniques used to improve MA are solely centered around information on medication and side-effects. HCPs experienced an internal conflict between providing patient-centered care versus using directive approaches to improve MA. Findings suggest how HCPs could thoroughly address patients’ individual barriers.
Keywords
Introduction
Medication adherence (ΜΑ) is defined as the extent to which patients’ medication-taking behavior matches condition recommendations and agreed-upon prescription from their healthcare provider (HCP) (National Institute for Health and Clinical Excellence, 2009). Medication non-adherence (MNA) rates are comparable between patients receiving short- and long-term therapies, but it constitutes a more serious problem for patients with chronic conditions, as it leads to worse quality of life, health deterioration, and treatment failure (Monnette et al., 2018). Chronic conditions are defined as diseases of long duration and generally slow progression and those that are associated with the highest MNA rates include asthma, cancer, diabetes, epilepsy, HIV/AIDS, and hypertension (Sarabi et al., 2016). In Cyprus, more than one quarter of the general population has multimorbidity—the co-existence of two or more chronic conditions (Kyprianidou et al., 2020) and about two in five Cypriot adults (39%) reported having at least one chronic condition in 2019. In chronic conditions, ΜΑ is crucial in order to manage symptoms, enhance recovery, improve health outcomes and prevent further disability (Bodenheimer et al., 2002).
Barriers and facilitators to MA in chronic conditions have been extensively examined in the literature. For example, some key structural barriers to adherence are identified (i.e. long waiting times at clinics and shortage of GP appointments) (Kagee and Delport, 2010; Kvarnström et al., 2021). Also, a recent scoping review suggested that the most reported barriers are younger age, low education, low income, high medication cost, side effects, patient beliefs/perceptions, comorbidities, and poor patient–provider communication (Konstantinou et al., 2020). Medical distrust is considered as detrimental in patient health outcomes (Dale et al., 2016). Though many barriers are under the direct control of the patient, keys to address the MNA problem lie with improvements in shared decision-making and patient-centered care (Osterberg and Blaschke, 2005). Shared decision-making increases MA and health outcomes in patients with chronic conditions (Matthias et al., 2013). Patient-centered care places patients’ feelings and preferences centrally in consultation and during treatment decisions (Stewart, 2001).
Evidence suggests that HCPs mainly use and rely on education and information provision to enhance MA (Abdulhadi et al., 2013; Wermeling et al., 2014; Young et al., 2015). However, behavioral science research suggest that information-provision constitutes only a small facet of behavior change and whilst it can enhance knowledge, it is less likely to improve MA on its own (Raynor, 2020). For instance, most people already know that it is crucial to adhere to their prescribed medication, yet they do not adhere as recommended for many reasons (Heath et al., 2015; Reason, 2000). In such cases, providing more information will rarely lead to improvements in MA (Arlinghaus and Johnston, 2018). Τhe information–motivation–behavioral skills (IMB) model (Fisher and Fisher, 1992) highlights that when it comes to chronic conditions, it is important that the patients have the information and knowledge regarding the need for adhering, to be motivated to change behavior and to have the behavioral skills to adhere.
Although patient-focused approaches are well known to be effective on improving MA (Konstantinou et al., 2020), there remains a lack of understanding on how HCPs perceive and deal with patients’ MNA behavior. A few qualitative studies focus on the perspectives of HCPs on barriers for MA among patients with chronic conditions. Among the perceived barriers were; poor knowledge of the illness and medication, fear of the drugs, polypharmacy, healthcare professionals having an authoritative role (Kvarnström et al., 2018), lack of motivation and knowledge (Ab et al., 2009; Edward et al., 2021; Ouwens et al., 2005). Moreover, two systematic reviews of qualitative studies focusing on HCPs’ perspectives, suggested the following perceived barriers; forgetfulness, lack of family support (Krishnamoorthy et al., 2022), lack of information and knowledge about the disease, lack of motivation, intentional MNA due to financial constraints and poor cognitive ability (Brundisini et al., 2015).
However, previous qualitative studies mainly focused on particular diseases, especially in specific hospitals and health centers (Kvarnström et al., 2018). As MNA is a context-sensitive problem that varies depending on the situation and the setting (Naghavi et al., 2019), this study aimed to examine the perceptions of HCPs working with patients with chronic conditions associated with the highest MNA rates conditions that is, asthma, cancer, diabetes, hypertension; (World Health Organization, 2003) in Cyprus. To our knowledge, there has been no qualitative research in Cyprus exploring the perceptions of HCPs on MNA. Also, building upon the previous qualitative studies, we aimed to explore the perspectives of HCPs in depth, as HCPs is suggested to be an important population for further qualitative investigation (Brundisini et al., 2015). A qualitative investigation of perspectives and reactions of HCPs on addressing MNA will enable an in-depth exploration of their feelings, experiences and attitudes. The main objectives were to: (a) Investigate HCPs’ perceptions, attitudes, beliefs, and reactions on MNA, and (b) Examine the strategies, practices, and interventions used to address MNA and improve MA. Exploring HCPs’ perspectives can inform interventions and strategies that can ultimately effectively combat MA.
Methods
Design
This was a qualitative study drawing on one-to-one interviews. Ethical approval was received from the Cyprus National Bioethics Committee (ref: EEBK EII 2018.01.185). Informed consents were obtained from all participants, with their anonymity and confidentiality ensured throughout the study.
Participants
HCPs were selected from a registry of the medical association of Cyprus and they were referred to by the professional network of the authors of this study. All HCPs were contacted by phone. Convenience sampling was used based on the availability and willingness to participate, with their participation being completely voluntary. HCPs could participate if they were Greek-speaking, living in Cyprus, and working with patients (asthma, cancer, diabetes, epilepsy, HIV/AIDS, and hypertension) that present the highest MNA rates.
Data collection
Individual, face-to-face interviews were conducted in HCP’s offices. Interviews were semi-structured, including open-ended questions, lasting about 20–30 minutes (Appendix A). All interviews were audio-recorded and transcribed verbatim. Interviews covered a broad range of topics including assessment methods of MA, beliefs and perceptions of responsibility assignment regarding MNA, barriers and facilitators to MA, and strategies used to address MNA. An interview guide was developed, independently reviewed and validated by three experienced researchers (PK, OK, APK) and piloted with two HCPs to ensure comprehensiveness of the interviews. Trained researchers (PK, OK) in qualitative methods conducted the interviews.
Reflexivity
The researchers involved had a diverse background (e.g. medicine, psychology) but they hold positive views on the importance of medication adherence and on medical professionals’ patient-centered care provision. These views inevitably influenced their interpretations of the data.
Data analysis
Data were analyzed following the steps of thematic analysis (TA) (Braun and Clarke, 2006). TA focuses on researcher’s role in knowledge production and the significance of deep reflection on, and engagement with the data. Researchers aimed to invoke psychological terminology, whilst taking a critical realist epistemological position, enabling analysis to take the data for what it was, but also bearing in mind that people formulate their own interpretation of the world.
After familiarizing with the data, the data were coded independently by the two researchers (CK, PK) and divergences were discussed, to establish a degree of inter-rater reliability and credibility. Atlas software was used to code and organize the data. The codes are illustrated in Supplemental Materials. Whilst re-reading the transcripts, two researchers (CK, IK) clustered the codes together and transformed them into more analytical and higher-level sub-themes and themes. Appendix B illustrates which codes led to each theme. Whilst two researchers transformed the codes into themes and subthemes, the entire team were involved in discussions about themes, any development and refinement and iteratively developed the “thematic map.” The researchers also discussed which quotes were most illustrative for each theme and subtheme and they tried to include quotes from many participants, so as to demonstrate transparency (Yardley, 2000).
Results
Participants
Overall, 21 HCPs working with patients associated with high MNA rates were approached and contacted to participate in the present study. From these, 10 HCPs (47.6%) were interested and participated in the study (seven males and three females), by which point data saturation was reached (Baker and Edwards, 2012). The sample was comprised by general surgeons (n = 3), pulmonologists (n = 2), medical oncologist (n = 1), neurologist (n = 1), cardiologist (n = 1), endocrinologist (n = 1), and a general practitioner (n = 1). All of them reported having more than 15 years of working experience in practice, being currently working at a public hospital (n = 1), at a private hospital (n = 6), in private practice (n = 2), and at an Oncology Center (n = 1).
Findings from the TA
Following analysis, themes and subthemes were organized into a “thematic map” illustrating a visual representation of any inter-linkages between them (Figure 1). The themes and subthemes will now be described with the use of exemplar quotes, and for reasons of clarity, they will be discussed separately, however, the analysis is sensitive to the links between them. A description of the themes and subthemes is presented through a dynamic interaction between data, reflecting participants’ meaning making, and researchers’ interpretive framework.
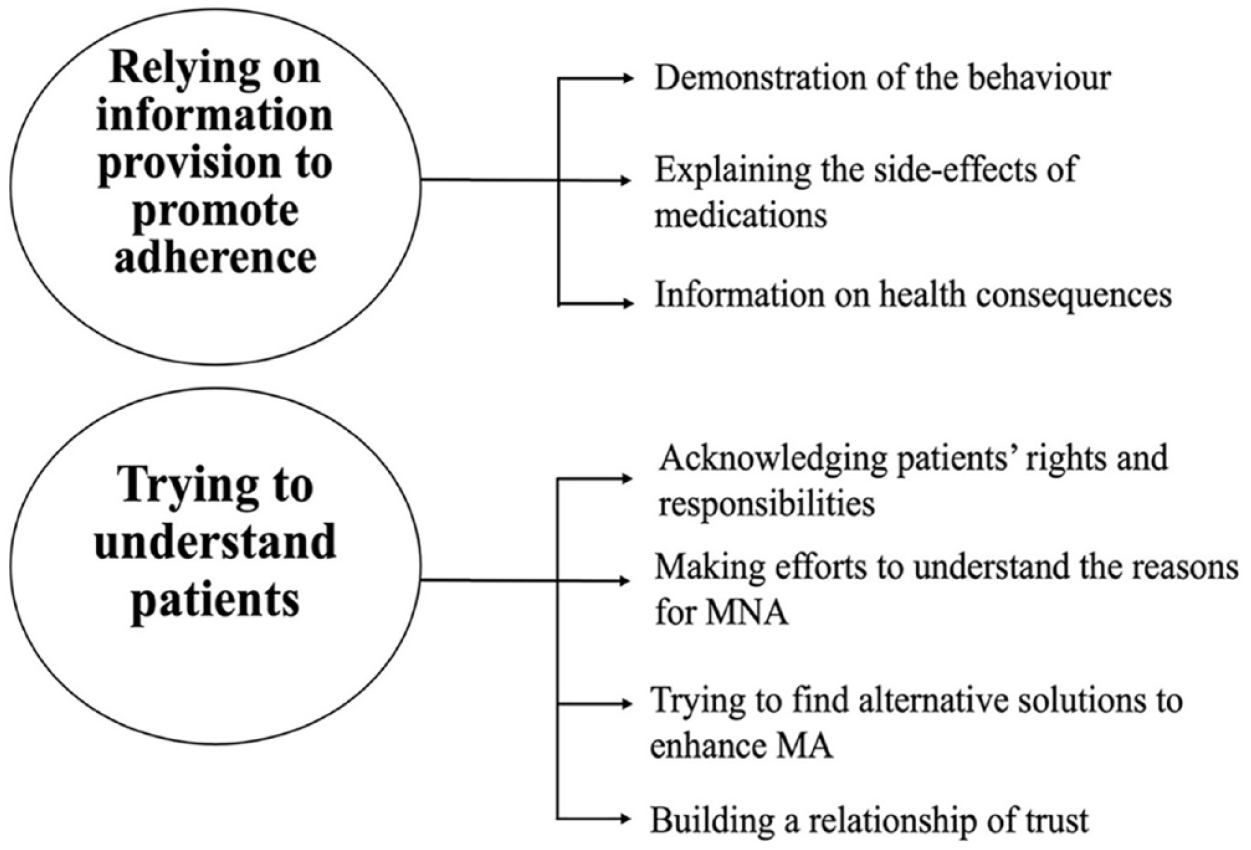
Thematic map of themes and subthemes generated through data analysis.
Two themes emerged from the analysis reflecting the ways that HCPs described their reactions to MNA of their patients.
Theme 1: Information provision to improve MA
In describing their reactions to their patients’ MNA, most HCPs stressed the importance of providing information to their patients on the importance of MA, using several strategies.
Demonstration of the behavior
HCPs provide information and then, if patients do not adhere to their medication, what follows is a practical education. HCP9 provides information because she believes there is a lack of understanding: They don’t understand the concept of prevention and they don’t understand the concept of chronic disease. Many times, I start by telling them that the chronic disease needs chronic treatment. [HCP9-endocrinologist]
For HCP1, education and information are prerequisites for MA: A patient well educated and well informed, does not give up his medication. [HCP1-pulmonologist]
The view of HCP1 appears one-sided and not patient-centered, as he assumes for the patient rather than asking the patient. If patients do not adhere, he may rely on the development of practical skills: I dedicate more time to train the patient and convince him that he needs to take his medication and secondly, I dedicate more time to his practical training on how to take the medication. I have devices with placebo, and I begin training again. [HCP1-pulmonologist]
For HCP1, MA seems to depend on “convincing” the patients about the value of medication. Convincing through the provision of information was mentioned by almost all HCPs (n = 8), reflecting a one-sided flow of direction of information from HCPs to the patient.
Explaining the side-effects of medications
This subtheme was identified in one case among the sample. HCP2 valued the provision of information regarding the side-effects and the value of the medication: I repeat the side-effects. If there really are any side effects, we are trying together with the patient to weigh the pros and cons of taking the medication. If I know that a side-effect will either go away, or it will not cause a significant change in the patient’s quality of life, I’ll try to convince him that the benefits of taking the medication are far more important than a mild side effect he may have to accept. [HCP2-neurologist]
In what follows, he replied to a question regarding to what extent he thinks that patients understand the reasons or the importance of taking their medication: I try as much as I can to explain to them the reasons, how the pill works, the possible side-effects and tell them that by weighing the two, I believe that this must be done. I give them percentages for the side-effects and I answer their questions. I think my patients leave my office well informed. Yes. [HCP2-neurologist]
According to HCP2, the provision of accurate information regarding the function of the medication and its side-effects, is of outmost importance. Also, despite that weighing pros and cons is suggested to be an effective behavior change strategy to get the patient motivated for behavior change (Black et al., 2020), the way it is used by HCP2, it is presented as information to the patient, without giving them the chance to weigh things for themselves.
Information on health consequences
Apart from using percentages to enhance MA, other HCPs similarly outlined specific strategies that they use, such as providing information to their patients on the possible negative consequences of MNA. HCP3 said: I mainly remind them how important it is to control the risk factors. What I do, is a bit of ‘controlled fear’. . .I sometimes show them articles. I have downloaded one a few days ago, which is a bit catchy, reporting what severe hypertension does and I show them that if you leave it, it may not have observable symptoms, but the time will come, when you’ll have 180 blood pressure, and then you may get a stroke. [HCP3-general practitioner]
When a patient appears to be non-adherent, what HCP4 reported doing: Just education, that it might be dangerous if you don’t take it. [HCP4-general surgeon]
The word “just” highlights that HCP4 perceives that education is all that is needed.
Theme 2: Trying to understand patients’ perspective
Some of the same HCPs that argued about the first theme, simultaneously showed evidence of collaborative decision-making. They expressed that they are trying to understand patients’ perspective and reasons for MNA and find alternative solutions to improve MA. For them, having a relationship of trust with their patients is important.
Acknowledging patients’ rights and responsibilities
Some (n = 3) HCPs reflected that they acknowledge the rights of patients to not take their medication. HCP7 highlighted: Once they are properly informed and have a complete picture of what it means to receive treatment and what it means not to receive treatment and have consciously decided not to receive treatment, then it’s their right not to receive treatment. If they don’t take it, they don’t take it knowing what the possible consequences may be. [HCP7-medical oncologist]
Similarly, HCP6 focuses on the explanation of side-effects, by allowing patients to make informed decisions: If they don’t want to adhere, I’ll not push them. I just explain the side-effects.[HCP6-cardiologist]
HCP6 and HCP7 stance toward MNA, differ from the previous HCPs, in the degree they acknowledge rights and responsibility. They both perceive that their role is to provide all the information, and by doing so, they fulfill their duties. From that point onward, if they fail to persuade the patients and patients do not adhere, it is their choice, and they accept it.
Making efforts to understand the reasons for MNA
Few HCPs presented efforts to understand the reasons behind their patients’ MNA. HCP2, when being asked what he does to help a patient who does not adhere to medication, stated: I can’t force you to get the medication. The choice is yours, the body is yours, the illness is yours, I am here with a consulting role. The responsibility is yours”. I just try to understand calmly the reasons. [HCP2-neurologist]
This quote gives the sense that his role is not to tell patients what to do, but instead, he constructs a relationship of respect and understanding. HCP8 similarly used to a great extent the word “try”: Of course, not with stringency, I think, but I want [them] to try and explain to me. I am trying to tell the patient “You should have taken it”. [HCP8-general surgeon]
This quote is characterized by ambivalence and feelings of a tension between having adequate understanding toward a patients’ perspective (i.e. “not with stringency,” “explain to me”) and a more authoritative approach (i.e. “you should have taken it”).
Both HCP8 and HCP2 are trying to understand why patients behave in a certain way and the intention is evident, however, the execution of this in practice does not support it.
Trying to find alternative solutions to improve MA
By understanding the reasons behind MNA, almost half (n = 4) of the HCPs highlighted how they actively try to find solutions and explanations. HCP5 stated: I try to understand why and see what I can do to increase the adherence. Maybe. . . the living conditions of the patient may be such that what I prescribed is not very convenient. [HCP5-pulmonologist]
HCP5 pays attention to contextual factors, however, she does not propose any other real solutions the barriers of MA.
Whilst HCP2 emphasized the importance of information provision, as indicated in Theme 1, he simultaneously evokes an understanding toward patients and their rights. He is trying to find ways to enhance MA: If they tell me that they have too many drugs and they don’t want to take them, we try to find ways with the pill boxes and reminders, in order to remember to take them. [HCP2-neurologist]
However, patients may say that they take too many drugs, and the doctor may perceive that they forget to take their medication. Therefore, the patient may mean one thing and the doctor may understand something else, thus helping them with the wrong thing.
Building a relationship of trust
Whilst HCPs make efforts to build a relationship of trust with the patients, they simultaneously express their disbelief toward patients’ perspectives. HCP6 stated: Most of them will lie to you. [HCP6-cardiologist]
Lying is attributed to fear toward the HCPs: They [the patients] tell you [the researchers] more than what they tell us, the HCPs. Often, I talk to the secretary or to the nurse, as they will tell them more things than what they tell me. They are afraid we will argue, until they get to know me. [HCP6-cardiologist]
HCP3 noted that lying depends also on the doctor’s approach: The best thing is when you directly ask them [about whether they took their medications]. When you are honest with them, and you have a relationship of trust, they’ll tell you. If you are distant and you are authoritarian, you create distance, and they’ll hide things from you. Therefore, I’m trying to have a relationship of trust with them. [HCP3-general practitioner]
However, simultaneously, HCP3 seems suspicious, reflecting that he remains vigilant about patients’ reports: They can bring their medication here. Of course, this action can also hide things from you. [HCP3-general practitioner]
Overall, HCPs are trying to understand patients’ perspective and why there is MNA. However, it is unclear in what ways and through which actions they show this effort. HCPs seem to have good intentions to help their patients, but they solely give information and use fear appeals. Therefore, they elicit an internal tension between providing patient-centered care versus using directive approaches to improve MA.
Discussion
HCPs seem to perceive MNA as patients’ fault. Therefore, they believe that providing information and practical education, will be sufficient. Our findings support the behavioral change wheel approach (Michie et al., 2011) which recommends that effective intervention functions should include training, persuasion, and education of patients. HCPs often use authoritative language in their efforts to provide education and “convince” the patients about the value of medication. This might be due to a power differential between the HCPs and the patients, as HCPs reflect that they possess the knowledge and from their perspective, it is crucial to “transfer” this knowledge to their patients (Nimmon and Stenfors-Hayes, 2016). Studies have suggested that institutional and hierarchical settings (e.g., hospitals) may perpetuate roles. HCPs’ role of being “experts,” can enhance their ability to make decisions for patients and abuse power, whilst the “sick” role of the patients can diminish patients’ power and ability to control their life (Prilleltensky and Prilleltensky, 2003; Zhai et al., 2020). Moreover, HCPs often consider lack of both education and understanding of the importance of medication as the most important barriers to adhering to medication (Kvarnström et al., 2018). This can be based on lay beliefs that people often lack knowledge and that by improving knowledge, their attitude can change (Speller, 2007). In Cyprus, there is a high proportion of the population with problematic health literacy—patients’ ability to obtain, process, communicate, and understand basic health information, to thus make appropriate health decisions (Andreou et al., 2019; Baker, 2006). However, whilst patients’ knowledge can be improved by providing education and information, interventions focusing on the provision of information and education appear to be ineffective to improve MA (Al-aqeel and Al-sabhan, 2011; Costa et al., 2015). There is a need to investigate HCPs perceptions, attitudes and strategies used so that multicomponent interventions, personalized to the patients’ needs and characteristics, and responding to the MA barriers they face are in use.
If the provision of information does not work, then fear appeals are used by HCPs because they seem to believe that once you impose fear, patients will conform to taking their medications. In a qualitative study conducted with patients with diabetes, it was found that when HCPs were using fear strategies to improve MA, feelings of anxiety and negativity toward their HCPs increased (Matthews et al., 2009). Conflicting evidence reflects that the use of fear may positively influence attitudes, intentions, and health behaviors (Tannenbaum et al., 2015). Our study suggests that HCPs do follow this strategy and the impact this can have to patients needs to be examined.
Some HCPs expressed their willingness to understand the patients’ views. However, their narratives do not truly reflect this. Whilst they acknowledge patients’ right to not adhere, they seemed to blame the patients. The way they go about it is authoritarian, which does not seem to allow for good communication and for patients to truly express their concerns. A recent systematic review found that even though patients are usually willing to discuss any concerns they have about medications they are prescribed, they emphasize the better communication and better information on medicines are critical factors from their perspective (Kvarnström et al., 2021). Whilst HCPs mentioned both internal (e.g. patients’ thoughts) as well as external (e.g. living conditions) barriers to MA (Konstantinou et al., 2020), they did not specify which ways of assessment they use to understand the nature of barriers and if they use any. Only one HCP seemed to propose techniques (e.g. pill boxes) to overcome a barrier (e.g. forgetfulness), though this was done without being sure whether this was indeed the barrier. So, their efforts and actions to deal with MNA, do not follow any assessment of the barriers to MA, thus they make disjointed efforts. This could further evoke that HCPs tend to think that techniques available are only for unintentional MNA. It remains unclear if HCPs ignore the fact that usually MNA can also be intentional and/or whether they use any techniques to address intentional MNA.
Finally, HCPs highlighted the importance of having good communication and connection with their patients. Effective communication constitutes a crucial aspect in the HCP-patient relationship and is suggested to be related with improved MA rates (Alfonso et al., 2009; Tavakoly Sany et al., 2020; Zolnierek and DiMatteo, 2009). A few HCPs mentioned that some patients lie to them, attributing it to their patients’ fear toward them or depending to their approach (e.g. authoritative or collaborative). One HCP mentioned that when he directly asks patients about whether they took their medications, they tend to tell him the truth. Patients can be very accurate in reporting whether they adhere to their medication if they are asked simply and directly (Duong et al., 2001) and are more likely to disclose MNA in response to being asked how often they miss a drug dose, compared to being directly asked if they take their medication as they should (Engel et al., 2017). Despite that, HCPs may distrust patients’ accounts of treatment failures, doubting their compliance with the treatment (Rogers, 2002). Consequently, being distrusted can be very disempowering. The power and authority of HCPs in medical decision-making, is suggested to create a power imbalance in the HCP-patient relationship (Cook et al., 2004). Patients already have less power than HCP in the context of healthcare provision, and being distrusted by HCPs, widens that power imbalance. As a result, a “no-blame” approach by HCPs, where they do not judge the patient, may be more likely to elicit an honest expression of MNA and concerns. Also, this approach could encourage patients to discuss about intentional MNA and any doubts or concerns they have about treatment. The HCPs in the study were making efforts to identify barriers to MA but it remains unclear whether they followed any assessment of reasoning for MNA. Addressing MNA is not about getting patients to take more medicines per se, but identifying a potential barrier to MA, assessing the reasoning for MNA, thus helping the patient to make informed decisions (d’Ancona and Weinman, 2021).
Limitations and future directions
Whilst the qualitative design of this study was beneficial to capture an in-depth understanding of the perspectives, psychological processes and reactions of HCPs toward MNA, there are several limitations. Firstly, the small number of participants is limiting the generalizability of the findings. Future research could use a greater number of HCPs and from different specialties, to enable a more representative sample. Secondly, the study included HCPs living in Cyprus. There may be important cultural differences between the cultural context of Cyprus and other European or Western contexts, limiting results’ applicability. For instance, the different health care systems and different cultural and societal effects, may influence HCPs’ beliefs. It would therefore be beneficial to replicate this study with HCPs from other countries. Moreover, even though data saturation was reached, it is unclear whether theoretical saturation was achieved (i.e. with a more heterogeneous sample of HCPs). By including more HCPs from various specialties, it is more likely that theoretical saturation would be achieved. Finally, this study uses interview methods that require participants to recall their experiences. There is a possibility that HCPs’ recall of their practice may be influences by trends happening during the interviews. Future studies may use naturalistic observational methods such as videotaped consultations (Asan and Montague, 2014) to observe interactions between HCPs and patients who do not adhere to their medication.
Practice implications
The findings reflect the strategies that HCPs use and believe that help, namely information provision and fear appeals. However, these are not the strategies that are empirically supported and in line with how to change MNA. HCPs can use more patient-centered approaches, such as motivational interviewing (Miller and Rollnick, 2012), that have demonstrated effectiveness and are useful to prepare the patients that are not ready to make behavior changes (Bischof et al., 2021). They could also focus on strategies aiming to enhance the patients’ motivation and combine education with other strategies instead of offering education alone. This could also be beneficial when addressing intentional MNA, as it is suggested to be largely associated with patient motivation (Molloy et al., 2014). Behavioral scientists could help with education and training HCPs on good communication skills, on MA and its barriers (i.e. personal barriers) and on behavior change techniques that can work to help combat this problem.
Literature shows that how people react to fear appeals, depends on their coping efficacy level—if efficacy is high, they are more likely to change their behavior in the suggested direction (Kok et al., 2018; Moussaoui et al., 2021). Therefore, HCPs could be careful on the extend of threat they use and perhaps, enhance patients’ self-efficacy instead since patients may be more likely to engage in MA when they believe they can execute those behaviors successfully (Okuboyejo et al., 2018).
Conclusion
To our knowledge, a few qualitative studies focus on the perspectives of HCPs on barriers for MA among patients with chronic conditions. Results reflected that HCPs mainly rely on information provision to address MNA rather than multicomponent approaches targeting the reasoning behind MNA. They do make efforts to understand patients’ perspectives but the execution of this in practice need to go beyond education and incorporate techniques of behavior change. Therefore, the results can have implications on how HCPs could use more patient-centered approaches, address patients’ personal barriers, and recognize and improve internal tensions.
Supplemental Material
sj-docx-1-hpq-10.1177_13591053241227003 – Supplemental material for Tensions in caring for chronic patients’ medication adherence: A qualitative study in Cyprus
Supplemental material, sj-docx-1-hpq-10.1177_13591053241227003 for Tensions in caring for chronic patients’ medication adherence: A qualitative study in Cyprus by Christiana Karashiali, Pinelopi Konstantinou, Orestis Kasinopoulos, Christos Michael, Alexia Papageorgiou, Irini Kadianaki, Maria Karekla and Angelos P Kassianos in Journal of Health Psychology
Footnotes
Appendix A
Appendix B
Table illustrating the codes which led to each theme.
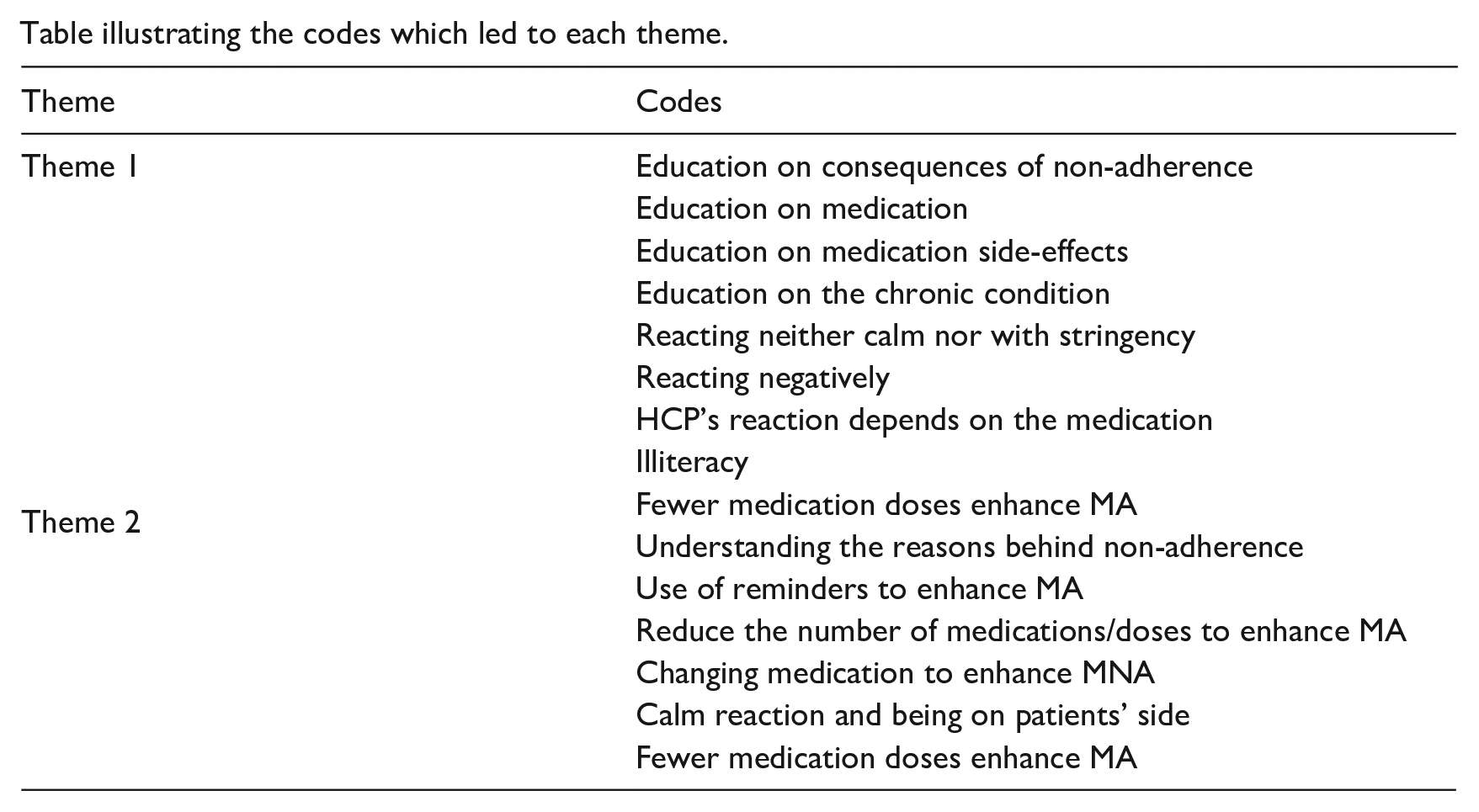
| Theme | Codes |
|---|---|
| Theme 1 | Education on consequences of non-adherence |
| Education on medication | |
| Education on medication side-effects | |
| Education on the chronic condition | |
| Reacting neither calm nor with stringency | |
| Reacting negatively | |
| HCP’s reaction depends on the medication | |
| Illiteracy | |
| Theme 2 | Fewer medication doses enhance MA |
| Understanding the reasons behind non-adherence | |
| Use of reminders to enhance MA | |
| Reduce the number of medications/doses to enhance MA | |
| Changing medication to enhance MNA | |
| Calm reaction and being on patients’ side | |
| Fewer medication doses enhance MA |
Acknowledgements
We thank all the HCPs who participated in this research project for their time.
Author contributions
Christiana Karashiali: Methodology, Investigation, Data Curation, Formal Analysis, Writing—Original Draft, Writing—Review & Editing. Pinelopi Konstantinou: Conceptualization, Methodology, Investigation, Validation, Writing—Review & Editing. Orestis Kasinopoulos: Conceptualization, Methodology, Investigation, Writing—review & editing. Christos Michael: Investigation, Writing—review & editing. Alexia Papageorgiou: Methodology, Investigation, Writing—review & editing. Irini Kadianaki: Methodology, Formal Analysis, Supervision, Writing—review & editing. Maria Karekla: Writing—Review & Editing, Supervision, Funding acquisition. Angelos P Kassianos: Conceptualization, Methodology, Writing—Review & Editing, Supervision, Project administration, Funding acquisition.
Data sharing statement
Any data from this work are available by contacting the corresponding author by reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was co-funded by the European Regional Development Fund and the Republic of Cyprus through the Research and Innovation Foundation (project: SOCIALINNO/0617/0014).
Ethics approval
The ethics committee of Cyprus National Bioethics Committee approved this study (REC number: ΕΕΒΚ/ΕΠ/2018.01.185).
Informed consent
All participants provided informed consent prior to their participation in this study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.