
Abstract
Background:
Sex-disaggregated data demonstrate that there are more female than male living kidney donors (LKDs), and this is widely thought to be a manifestation of gender inequities. A better understanding of how gender norms, roles, and relations influence the living kidney donation process is needed.
Objective:
We aimed to develop an analytical tool that can be used to conduct a systematic gender analysis of the living kidney donation process.
Design:
A participatory research approach was used.
Setting:
Canada.
Participants:
Canadian living kidney donors and health care professionals.
Methods:
Using a participatory research approach, we co-designed a gender analysis matrix (GAM) applicable to the context of living kidney donation. This tool is the first step into conducting a gender analysis of the living kidney donation process. Participants included 11 healthcare professionals, 6 LKDs, 1 patient partner, and a core methodology team (3 qualitative researchers and a gender analysis expert).
Results:
Following an iterative process, a final LKD-GAM with 4 columns and 4 rows was created. The gender-specific domains are access to resources, division of labor and everyday practices, social norms and beliefs, and decision-making power and autonomy. Context-specific domains are the decision to donate, physical and mental wellbeing, experiences with health services, and broader social and economic impacts of (non-)donation. Key insights for our future work include diversity in our sample (include LKD candidates, men, and different life stages) and unpacking the notions of consent, constrained consent, and subtle coercion.
Limitations:
The GAM’s scope is likely limited to the Canadian context. The study was also limited by the recruitment of LKDs from a past list of participants and by the lack of cultural and linguistic diversity in the sample.
Conclusion:
Using a participatory co-design approach, we have developed a robust tool that will inform a multinational qualitative study to better understand factors contributing to gender disparities in living kidney donation.
Introduction
Since the first successful living donor kidney transplant in 1954, living kidney donation has become a process championed by science and public education. 1 It is widely regarded as the best therapy among eligible patients with kidney failure and is cost-effective for healthcare systems; in some countries, it is the only available or accessible therapy.2-9 Thus, there has been a significant rise in the number of living kidney donors (LKDs) in the past 70 years, with the Global Observatory on Donation and Transplantation reporting almost 350,000 living donor kidney transplants being performed in the past decade alone (2014-2023). 10
Often equated with the actual surgery alone, we believe that living kidney donation is a process that includes learning, contemplation, decision, evaluation, nephrectomy, recovery, and a lifetime need for follow-up and monitoring. Analyzing kidney donation as a process rather than an event can help delineate how unintentionally discriminatory systems, practices, and structures can contribute to gender disparities in living kidney donation (e.g., how gender norms, roles, and relations create differences between and among women and men within the kidney donation process). 11 Indeed, gender disparity in living kidney donation is a recognized and persistent observation globally. Sex-disaggregated data have repeatedly demonstrated that in most countries, there are more female than male LKDs in most countries, and this is widely believed to represent a gender disparity.12-19 A better understanding of how gender norms, roles, and relations influence the living kidney donation process may help to address this gender disparity.
Tackling this disparity is an important priority in transplantation and kidney donation. Women are less likely than men to receive a kidney, while they are simultaneously more likely than men to donate a kidney.20,21 A gender analysis may highlight the factors that impact the living kidney donation processes and may impact donation rates among men, women and gender-diverse individuals. A gender analysis is “a systematic analytical process based on sex-disaggregated and gender information to identify, understand, and describe gender differences and the relevance of gender roles and power dynamics in a particular context.” 22 Currently, evidence regarding the underlying dynamics of gender disparity in donation is limited and mostly focused on women LKDs.18,23-26 Some scholars argue that gender disparity should be considered an under-representation of men, with men donating less due to masculine perceptions and social pressures or expectations of fulfilling the earner/provider role. 27 This may lead to them feeling less inclined to pursue kidney donation as they may be unable to take time off work or risk losing their provider role.
This article outlines the participatory process we have undertaken to develop a tool to conduct a gender analysis of the living kidney donation process. This tool was designed to apply to the experience of LKDs and candidates.28,29 Candidates are potential LKDs who expressed an interest, but were deemed ineligible to donate, dropped out of donation, or are currently in the process of being evaluated for kidney donation. LKD and candidates will be collectively referred to as LKDs from here on. This tool is the first step in conducting a gender analysis of the living kidney donation process to explore how gender power relations are constructed and negotiated in different settings and health systems, leading to gender disparities in living kidney donation. In this paper, we present our tool, the approach to designing this tool, and key insights gained from the participatory process.
Methods
Approach
We adopted a participatory approach, which is a form of systematic inquiry conducted in direct collaboration with relevant interest-holders affected by the issue under investigation.30-32 It fosters co-constructed research through partnerships between researchers and interest-holders, community members, and those with insider knowledge and lived expertise.31,32 We aimed to co-design a gender analysis matrix (GAM). First developed in the 1990s within the field of international development to incorporate a gender lens to the development and monitoring of projects,33,34 it has since been refined and adapted to many different contexts. In the health field, GAMs have been used to help researchers and policymakers conduct systematic gender analyses and explore the impact of gender power relations on specific topics.35,36
The GAM mobilizes a gender framework that explores the ways in which gender power relations manifest as inequities, and how these create different and/or inequitable experiences for LKDs. GAMs are constituted of columns and rows. The columns represent the gender analysis domains, while the rows are context-specific and need to be designed to respond to a particular context. We adopted the gender domains developed by Morgan et al. 28 They are: (1) Access to resources; (2) Division of labor and everyday practices; (3) Social norms and beliefs; and (4) Decision-making power and autonomy. While the gender domains remain stable, each context necessitates topic-specific domains (rows) which are relevant to the topic being studied. Our co-design process was therefore aimed at validating the use of a GAM and at developing our context-specific domains.
Co-design process
Our co-design process was grounded in the philosophy of Experience-Based Co-Design (EBCD), which builds on observations of service gaps and centers the experiences of people who use and deliver healthcare services. 37 EBCD includes multiple stages, from the project set-up to the celebration and review of the results. In this article, we report on the stages in which we gathered the professional and lived experiences of Health Care Providers (HCPs) and LKDs in order to co-design our GAM.
Our study design is outlined in Figure 1. Based on our systematic literature reviews,38-40 our prior qualitative work with Canadian LKDs and their family physicians,41-44 and our gender expert’s input on how to operationalize gender matrices within health and health systems research,29,35,45,46 we identified the need to study gender disparities in living kidney donation and created the initial iteration of the GAM (steps 1 and 2). We then undertook consultations with interest-holders in Canada. We started with the HCPs (step 3), then we refined the GAM (step 4) and proceeded with our focus group with LKDs (step 5), leading to our final iteration of the GAM (step 6). During these interviews and focus groups, we presented the LKD-GAM to the participants and asked them to discuss the relevance of the different domains, according to their own expertise and/or lived experience. These discussions were aimed at exploring the relevance of the tool in general and of the topic-specific domains in particular. The context-specific domains which are in the final version of the GAM emerged through these discussions. While this was not the goal at first, these discussions also generated many insights into the next steps of our study.
Data collection
To develop the context-specific domains, this research involved semi-structured interviews and focus groups with healthcare professionals (HCPs), LKDs, and a patient partner (HB). Focus groups and interviews are particularly appropriate because they actively engage participants in sharing their experiences, ideas, and preferences in a collaborative and open manner. 47 These methods facilitate a rich, interactive dialogue that is essential for co-design. The interviews and focus groups were conducted virtually, and the guide is attached as Supplement 1. The ones with HCPs were conducted by an experienced qualitative researcher with prior experience in participatory research (KL) from May to July 2024. The LKD focus group was conducted and moderated by two qualitative researchers (KL, MGB) in November 2024. The interviews and focus groups were structured around the GAM. Each row and column was presented, and their relevance was discussed with the participants. The participants were also invited to reflect on their lived experiences in relation to the context-specific domains that had been identified.
For the HCPs, a mix of focus groups and interviews was conducted due to challenges in merging the schedules of different interest-holders from different time zones. However, the integration of focus groups and individual interview data is reported to improve the trustworthiness of findings as it helps lead a productive iterative process, identify individual and contextual circumstances surrounding the phenomenon under investigation, and allows the convergence of the data using two distinct data collection methods. 48
We ended the data collection when we reached data saturation, i.e., when new interviews and focus groups did not provide new insights and perspectives. In this context, it meant that the interest-holders did not have new comments or suggestions on the GAM and that they understood it as capturing adequately their lived experiences.
Participants and recruitment
Participants included HCPs, LKDs, and a patient partner who is a living liver donor (HB). HB was involved both as a member of our research team and as a participant in the research. She has contributed to the study design and is an ongoing collaborator on the study. Our core methodology team included experts in qualitative research (MGB, KL, SS) and gender analysis (RM). The inclusion criteria for HCPs were involvement in LKD care, evaluation, or nephrectomy. The inclusion criteria for LKDs were any individual who has undergone kidney donation in Canada and could communicate in English or French. HCPs were recruited using purposive sampling. LKDs were recruited from those who participated in our prior work and consented to be invited to future studies. We aimed to obtain the perspectives of people of different genders, various roles among HCPs (nurse, transplant coordinator, social worker, nephrologist, surgeon), and diverse donor-recipient relationships (e.g., directed vs. non-directed).
Data analysis
Each interview and focus group lasted approximately an hour, was conducted via the Zoom™ platform, and was audio- or video-recorded. Audio files were transcribed verbatim. We analyzed our data qualitatively, using a conventional content analysis approach, 49 allowing categories about the relevance and refinement of the GAM domains to emerge inductively from the transcripts. We used an iterative process whereby the modifications suggested by participants were subsequently explored with other participants.50,51 This ongoing process allowed us to introduce different versions of our LKD-GAM until we reached saturation.
Ethics
This study was reviewed and approved by the Research Ethics Board of the McGill University Health Center Research Institute, Montreal, Canada (ID: 2024-9913).
Results
Participant characteristics
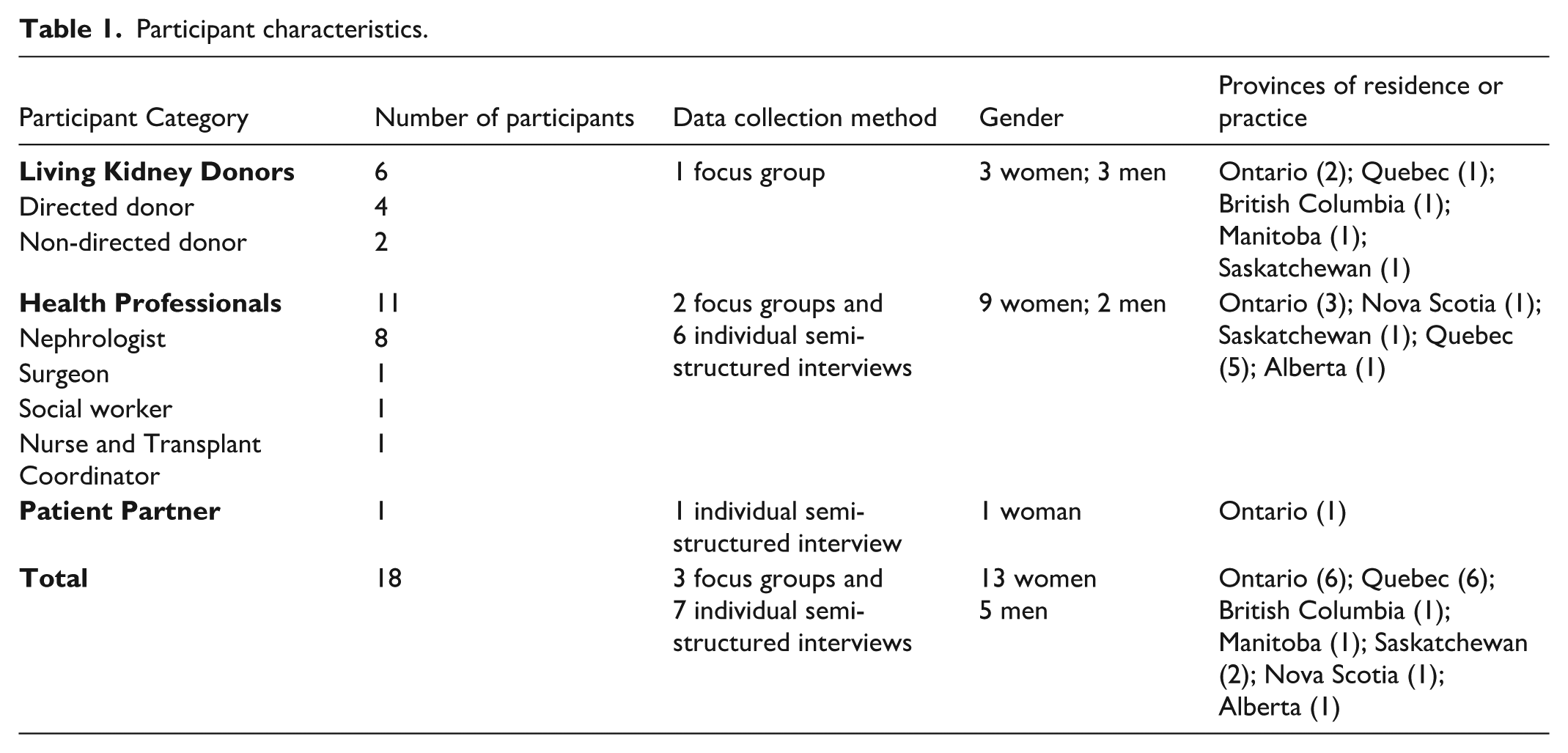
Our participants included 11 HCPs, 6 LKDs, and 1 patient partner, as elaborated in Table 1. HCPs represented major transplant centers in Canada and covered different roles (nephrologist, surgeon, social worker, nurse and transplant coordinator). Most of them also held academic positions. The LKDs came from 5 provinces and represented a diversity of experiences of donation: 2 were non-directed donors, 2 donated to family members, 1 donated to a friend, and 1 to a colleague. Moreover, 3 LKDs donated through the paired exchange program.
Participant characteristics.
The living kidney donation gender analysis matrix (LKD-GAM)
Through our participatory process, we confirmed with our participants the relevance of a GAM in the context of living kidney donation. The participatory approach used in this study resulted in the development of an LKD-GAM presented in Table 2 and discussed below.
Our final GAM includes 16 cells, each populated by lists of elements that will help us explore how these elements may collectively contribute to gender disparity in the living kidney donation process (Table 2).
A gender analysis matrix created using a participatory approach to conduct a gender analysis in living kidney donation.

The gender domains
Our final GAM uses the gender domain as developed by Morgan et al. 28 Applied to the context of living kidney donation, we describe them as follows: (1) Access to resources: This domain addresses a LKD’s access to resources such as income, employment, insurance, education, and information; (2) Division of labor and everyday practices: This domain focuses on how labor and daily responsibilities are distributed within and outside of the LKD’s household; (3) Social norms and beliefs: This domain addresses norms and beliefs held by the LKD, their family, social network, and HCPs, around themes such as gender roles, health, care, risk, and work; and (4) Decision-making power and autonomy: This domain addresses the decision-making power relayed to institutions and laws, as well as the distribution of decision-making power within the LKD’s network, including family, friends, social support network, HCPs.
Context-specific domains
Through our participatory approach, we developed 4 context-specific domains to address the unique context of living kidney donation. They represent the rows of our matrix: (1) Decision to donate: This domain relates to the decision-making process of LKDs from initial contemplation to the final decision; (2) Physical and mental wellbeing: This domain focuses on the physical and mental wellbeing of LKDs throughout their donation journey; (3) Experiences with health services: This domain relates to the experiences of LKDs with health services throughout the continuum of care; and (4) Broader social and economic impacts of (non-)donation: This domain relates to the short- and long-term impact of donating (or not) on the social and economic lives of LKDs.
Modifications and iterations of the LKD-GAM
Many modifications were made throughout the co-design process to arrive at those domains. To align with our understanding of organ donation as a process, we started with context-specific domains that followed the linear process of donation as presented in Supplementary Figure 1 (risk and vulnerability of becoming a donor, donor screening, surgery, immediate post-donation, and long-term care). The “decision to donate” row was very generative and appreciated by the participants, so we kept it. However, early on during our co-design process, we realized that the other rows did not create a GAM that captured many of the dynamics mentioned by our participants and prior literature. Instead, we developed, with the suggestion of participants, the transversal domains: the wellbeing of LKDs, their experiences with health services, and the social and economic impacts of donating. These domains did not hinder our understanding of donation as a process, but they foregrounded transversal domains, impacted by gender, which were deemed essential by the interest-holders consulted.
Other smaller modifications were made. Our first row, “decision to donate,” was initially referred to as “risk and vulnerability.” This label was meant to capture the likelihood of someone becoming an LKD and the health risks related to donation. Many HCPs challenged this wording, as they suggested that it emphasized the inherent risks of donation and gender inequality, potentially deterring others from donating. They recommended a more neutral term, “decision to donate,” reflecting the contemplation of kidney donation and the key factors during this phase. We subsequently had to ensure that the row “decision to donate” was clearly understood as conceptually distinct from our column “decision-making power and autonomy.” We thus emphasized that the latter relates to the distribution of power within the network of people surrounding the LKD, whereas the “decision to donate” relates to the decision-making process of LKD.
Populating the LKD-GAM
At the intersection of these columns and rows, the LKD-GAM highlights the key elements stemming from our systematic literature reviews, interviews, and focus groups. These elements have been identified as contributing positively or negatively to gender differences throughout the living kidney donation process. To confirm that the GAM was comprehensive, we ensured that every element found in our literature reviews, and everything put forward by our participants, fell somewhere within the matrix.
Key insights from the co-design process
While our participatory process was first aimed at co-designing the topic-specific domains of the GAM, the approach also allowed us to gain insights that will help design our subsequent qualitative study where we will operationalize the LKD-GAM. During our interviews and focus groups, the discussions led participants to talk about their own lived experiences and the ways in which the different domains of the GAM have shown up. These insights were extremely valuable in confirming the study design, data collection tools, and analysis. They are outlined in Figure 2 and presented below.

Study outline and the different steps we undertook as part of a participatory research approach to design a gender framework called a gender analysis matrix (GAM).

A summary of the key insights gained during this participatory research that helped inform the methods of a large multinational qualitative research study that we will undertake to unpack the contributors of gender disparity in living kidney donation in different societies and health systems.
Diversity in the study population
First, the need to incorporate the experiences of LKD candidates was highlighted. This was suggested by HCPs and LKDs in order to obtain a comprehensive understanding of how gender norms, roles, and relations influence the living kidney donation process. HCPs and LKDs suggested this will minimize the risk of selection bias by enhancing our understanding of the gendered experiences of individuals who do not pursue donation. In addition, participants also suggested capturing a wide range of experiences in our subsequent purposive sampling. These experiences include non-directed (LKDs with no intended recipient) vs. directed (LKDs with an intended recipient) donation and different life stages to account for variations in age, familial responsibilities, and income levels. Moreover, it was suggested that the views of representatives of the general public, particularly from communities with low living kidney donation rates, be incorporated further to enhance the applicability and scope of our gender analysis.
Inclusion of men
A key insight stemming from our focus group with LKDs relates to the way that gender disparity in living kidney donation is conceived of as an over-representation of women rather than an under-representation of men. A few of our participants highlighted the pressure of gendered social norms on men. One participant in our LKD focus group stated: I was discouraged from being a donor simply because . . . what if something happens in the surgery and you know you can no longer work and then how is your family going to be supported? So I think it’s systemic. I think that there’s actually people within the system that are discouraging people who identify as male from donating simply because of an outdated outlook that says that men have to be or are only the . . . the breadwinners. (Man, Donated in his 40s, non-directed donation)
This led us to consider that the dissuasion of men to donate may be an important avenue of research, alongside the factors contributing to higher donation rates in women. It also points to the potential gender biases within the healthcare system. These insights, stemming from our focus group with LKDs, will be explored in our qualitative study.
Issues around consent
Participants also discussed the notions of consent, constrained consent, and the subtle pressure to donate. They suggested that these nuances would be challenging to capture. Participants therefore suggested individual semi-structured interviews with LKDs as the next step of the study, rather than focus groups, as a more optimal data-gathering method to foster trust and discuss the notion of consent in more depth. It is, however, possible that we will be unable to fully unpack this issue during a 1-hour interview. Mitigation strategies to address this will be adopted, such as building rapport with the participants and using open-ended questions and suitable probes.
Discussion
Using a participatory co-design approach, we have developed a robust tool to conduct a multinational qualitative study to better unpack the contributors of gender disparity in living kidney donation in different societies and health systems. The tool will inform the development of semi-structured interview guides for our planned qualitative study and help ensure that we ask relevant questions that touch on the many elements identified within the matrix. The comprehensiveness of the matrix ensures that we address all possible sites of gender power dynamics. We also shared key insights that helped refine our research question, analysis, and sampling strategy.
GAMs have recently been mobilized in health research, notably in the infectious diseases outbreaks research, in order to conduct gender analyses and highlight how gender inequities affect health.35,36,45,52,53 We have adapted this tool to the context of living kidney donation, highlighting its flexibility and the importance of participatory approaches. Indeed, participatory approaches have been increasingly employed to ensure the relevance of the research to the communities it aims to serve. 31 By integrating the perspectives of LKDs and HCPs, we have ensured that our tool reflected the specific context of these different interest-holders and their many concerns. The comprehensiveness of the LKD-GAM will allow us to capture how gender dynamics transpire at various stages of the living kidney donation process and impact different aspects of the LKD’s life.
As is often noted, participatory approaches may be challenging as they are more complex and time-consuming than other research approaches. 30 Two of the challenges frequently cited in the literature are, first, the sharing of power between academic and non-academic partners and between HCPs and patients, and, second, the building of trust.54,30 Working with our long-standing patient partner and recruiting LKDs from the pool of past participants facilitated trust-building by capitalizing on solid relationships that had already been forged. In addition, we employed certain proven strategies to equalize the power, such as conducting interviews and focus groups with HCPs and LKDs separately. Despite the length of time (nine months) in developing the GAM and the complex evolving nature of the research, the depth of the resulting tool will render the rest of the process more efficient, as we have, in advance, confirmed the relevance of our matrix with a wide range of interest-holders.
We highlight the following limitations of our study. While the co-design of our LKD-GAM was informed by data from a systematic review of the literature from different countries, stakeholder consultations were confined to Canada. Our future work will entail examining the applicability of the LKD-GAM across different settings with variable gender inequality indices. Our sample of LKDs all identified as White and English speakers. We acknowledge that the perspectives of individuals from culturally and linguistically diverse backgrounds and from gender-diverse individuals may differ. However, the LKD-GAM was co-designed to be flexible and to capture a wide and diverse range of experiences within its domains. Our recruitment strategy for the next step of the study will take this into account. Furthermore, by expanding our recruitment to candidates who did not end up donating, we will be able to address the experiences of the communities that are underrepresented within LKDs. Our recruitment of LKDs who had participated in prior studies may also form a selection bias in which the group was very motivated and eager to share their opinions. The view of this group might differ from the rest of the population. However, they were recruited from studies that were different in nature and did not touch on topics of gender. The nature of this particular focus group, the validation and discussion of the LKD-GAM, was also uniquely different than individual interviews.
In summary, using a participatory research approach, we have co-designed a LKD-GAM that will now be operationalized in a qualitative study to better understand gender disparity in the living kidney donation process. The iterative and participatory process of refining the GAM will ensure that our research is both comprehensive and systematic, while the findings are meaningful and trustworthy. The LKD-GAM has significant potential for advancing research and practice in living donation. While this study focuses on LKDs, the matrix can be adapted to explore gendered experiences in other areas of nephrology and transplantation. Future applications of this tool may provide insights to inform policy and improve equity in healthcare access and outcomes.
Supplemental Material
sj-pdf-1-cjk-10.1177_20543581251385066 – Supplemental material for Developing an Analytic Tool Using a Participatory Research Approach to Examine Gender Differences in the Living Kidney Donation Process
Supplemental material, sj-pdf-1-cjk-10.1177_20543581251385066 for Developing an Analytic Tool Using a Participatory Research Approach to Examine Gender Differences in the Living Kidney Donation Process by Mathilde Gouin-Bonenfant, Katya Loban, Rosemary Morgan, Heather Badenoch, Ann Bugeja, Christine Dipchand, Rahul Mainra, Marie-Chantal Fortin, Ngan N. Lam, Ahsan Alam and Shaifali Sandal in Canadian Journal of Kidney Health and Disease
Footnotes
Acknowledgements
Drs. Sandal is supported by the Chercheur boursier clinicien—Junior 1 award from the Fonds de recherche du Québec—Santé and Dr. Gouin-Bonenfant by a Women in Transplantation research fellowship. The team would like to thank and acknowledge and thank the HCPs and LKDs who participated in developing this analytic tool.
Author Contributions
Research idea and conception: SS
Study design: KL, RM, SS, HB
Data acquisition: MGB, KL
Data extraction and analysis: MGB, KL
Data interpretation: MGB, KL, RM, HB, AB, CD, RM, MCF, NLL, AA, SS
Supervision or mentorship: RM, SS
Created the first draft of the manuscript: MGB, KL
Reviewed and revised the manuscript critically for important intellectual content: All remaining authors
All authors approve the final version to be published and agree to be accountable for all aspects of the work.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a Planning grant from the Canadian Institute of Health Research (PCS – 195106)
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Sandal has received an education grant from Amgen Canada and a speaking honorarium from AstraZeneca. The other authors have no relevant disclosures.
Data Availability Statement
All the data generated is presented in the manuscript.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.