
Abstract
Background:
It is unclear whether kidney donation leads to lifestyle changes in terms of cannabis and cigarette use.
Objective:
To describe cigarette and cannabis use before and after kidney donation and to determine their associations with lifestyle and clinical factors.
Design:
Retrospective cohort study.
Setting:
The Living Kidney Donor program in the Champlain Local Health Integration Network at The Ottawa Hospital in Ottawa, Canada.
Patients:
The study included 178 living kidney donors who donated between January 2009 and December 2018.
Measurements:
Donors were screened for cannabis and cigarette use by telephone interview. Their clinical characteristics and changes in kidney function before and after donation were recorded.
Methods:
Cannabis and cigarette use before and after kidney donation were compared using chi-square test. Risk factors associated with their use was examined by univariate and multivariate logistic regression. Wilcoxon rank sum test was used to examine the association of cannabis and Chronic Kidney Disease Epidemiology Collaboration equation (CKD-EPI) estimated glomerular filtration rate (eGFR) at donation and at last follow-up. T-test was used to examine the association of cigarette smoking and CKD-EPI eGFR at donation and at last follow-up.
Results:
Among 305 donors, 262 met inclusion criteria and 178 participated (mean of 4.7 ± 2.9 years from kidney donation). Cannabis and cigarette use were reported by 5% (9 of 178) and 13% (23 of 178) at donation. After donation, 8% (14 of 178) and 5% (9 of 178) started cannabis and cigarettes, respectively; 74% (17 of 23) of smokers remained smokers after donation and 88% (53 of 60) who quit smoking before donation did not restart after donation. In multivariate analysis, non-married/common-in-law status was associated with cannabis use (odds ratio, 2.73; 95% confidence interval, 1.05-7.11; P = .04). There was no difference in eGFR pre- or post-donation among cannabis or cigarette users.
Limitations:
The single-center study design limits generalizability. Social desirability bias may have affected survey responses and cigarette smoking was not quantified.
Conclusions:
Cannabis and cigarette use was uncommon in the studied population and was not associated with remaining kidney function. Cannabis use increased post-donation. Most smokers remained smokers after donation and most donors who quit smoking before donation did not restart after donation. This warrants education and support for potential donors who smoke, to quit smoking prior to donation to reduce risks of cardiovascular and end-stage kidney disease.
Trial Registration:
Not applicable as this is not a clinical trial.
What was known before
Data around cannabis use and cigarette smoking patterns before and after kidney donation are limited. Smoking at the time of kidney donation may be associated with an increased risk of end-stage kidney disease among living kidney donors.
What this adds
Cannabis use was more prevalent after kidney donation and was associated with non-married/common-in-law status. Most smokers remained smokers after donation and most donors who quit smoking before donation did not restart after donation. This warrants education and support for potential donors who smoke, to quit smoking prior to donation to reduce risks of cardiovascular and end-stage kidney disease.
Introduction
Candidates for living kidney donation undergo medical and psychosocial evaluation for fitness for surgery and long-term safety. Controversy exists around the acceptance of living kidney donor candidates who smoke cigarettes and is center-dependent. Smoking may be associated with an increased risk of end-stage kidney disease (ESKD) among living kidney donors, although overall risk is low.1,2 An analysis of linked US transplant registry and death records found that kidney donors who smoked had approximately 5 times the adjusted mortality over 12 years compared with non-smoking kidney donors. 3 A single-center study of 612 donors showed that estimated glomerular filtration rate (eGFR) 6 months after donation was significantly reduced among those who had smoked or formerly smoked at the time of donation compared with non-smokers. 4 A recent decision analysis study suggested that smoking at the time of donation reduces life expectancy and increases the lifetime risk of ESKD compared with non-smoking donors. 5 There is limited data on smoking status after donation. One retrospective study of 98 living kidney donors included 46 smokers at the time of donation and 60% continued smoking at 1 year after donation. 6
In addition, recent evidence suggests that 15% of Canadians use cannabis daily or almost daily. 7 Further increases have been noted since legalization in Canada in 2018. 7 Cannabis use has been associated with psychosocial, cognitive, and respiratory complications. 8 The relationship between cannabis use and kidney function has not been well characterized. Several case reports suggest a higher risk of acute kidney injury with synthetic cannabinoid use. 9 The impact of cannabis use on kidney function in donors is unclear with 1 available study, which suggested no difference in eGFR between 31 cannabis-using and 263 non-cannabis-using donors 12 months after donation. 10
To help advance our understanding of living kidney donor health behaviors and outcomes, we aimed to describe cannabis use and cigarette smoking in living kidney donors before and after kidney donation, and their associations with lifestyle and clinical factors. We hypothesized that kidney function after donation would be worse among those with a smoking history at the time of donation. Recreational cannabis use was considered unlikely to be associated with differences in kidney function after donation.
Materials and Methods
This is a retrospective cohort study of all consecutive donors in The Ottawa Hospital Living Kidney Donor program between January 1, 2009, and December 31, 2018. A screening questionnaire was developed and administered to contactable, English-speaking donors to prospectively capture current cigarette and cannabis use and related lifestyle factors and health behaviors after kidney donation. Questionnaire completion was the inclusion criterion for the study. The questionnaire was designed by the Living Kidney Donor team at the Ottawa Hospital after a comprehensive literature review, including adaptation of pertinent questions from the 2018 Canadian Community Health Survey administered to the general population; 2 questions were also adapted from the Patient-Reported Outcomes Measurement Information System (PROMIS) Global Health measures to evaluate mental and overall health.11,12 The questionnaire contained a total of 41 items, 14 of which allowed for open-ended responses. The questionnaire was reviewed by donor nephrologists and the Patient and Family Advisory Council of our regional nephrology program and was then pilot tested with 3 donors. Their feedback around the clarity, suitability, and readability of the items was obtained and incorporated into the final questionnaire. All English-speaking donors were contacted by telephone over 3 months (up to 4 contact attempts, May 2019-July 2019). The questionnaires were conducted by someone who was not part of their donor care team to try to reduce social desirability bias. 13
Personal identifiers were not associated with the gathered data. Demographic data and laboratory data around kidney function and urine albumin excretion before and after donation were obtained from the electronic health record for donors who completed the questionnaire. Data on smoking and cannabis use at the time of kidney donation were obtained from the donor nephrologist and social work consultation notes, both of which often take place within 3 months before kidney donation. Smoking and recreational cannabis use are considered in overall risk assessment but by themselves are not contraindications to donation in our center. All living donors meet with a social worker to discuss psychosocial issues related to donation and non-directed donors are assessed by a psychiatrist.
Exposure Definitions
A donor who smoked cigarettes at the time of donation was defined as smoking within 4 months prior to donation, based on consensus among the local donor nephrologists. A former smoker was defined as anyone who quit smoking cigarettes at least 4 months prior to donation. A non-smoker was defined as never having smoked cigarettes. Cannabis included marijuana, hashish, or any other cannabis in its dry form or when mixed into another product, including an edible, hashish, capsule, pill, or spray. Like smoking, 4 months prior to donation was used to define current versus former cannabis users.
Statistical Analyses
Continuous variables were expressed as mean ± SD. Categorical variables were expressed as numbers and percentages. Cannabis and cigarette use before and after kidney donation were compared using chi-square test. Risk factors associated with the use of cannabis and cigarette smoking were examined by univariate logistic regression. Based on univariate comparisons, all variables identified as significant (at P < .1) were then entered into a logistic regression to identify factors that were associated with smoking and cannabis use. A P value of <.05 was considered significant. Wilcoxon rank sum test was used to examine the association of cannabis and CKD-EPI (Chronic Kidney Disease Epidemiology Collaboration equation) eGFR at donation and at last follow-up. T-test was used to examine the association of cigarette smoking and kidney function at donation and at last follow-up. Statistical analyses were performed using SAS, version 9.4 (SAS Institute Inc). The study is reported according to the “Strengthening the Reporting of Observational studies in Epidemiology (STROBE) statement”.
Results
In all, 305 kidney donors were identified in The Ottawa Hospital Living Kidney Donor program. A total of 262 donors had a working telephone number and spoke English and 178 questionnaires were completed (Figure 1). The mean (SD) time from kidney donation to questionnaire completion was 4.7 ± 2.9 years. The mean (SD) time from kidney donation to last serum creatinine was 3.0 ± 2.6 years. The mean (SD) age of donors was 54 ± 13 years and 63% of donors were women (Table 1).
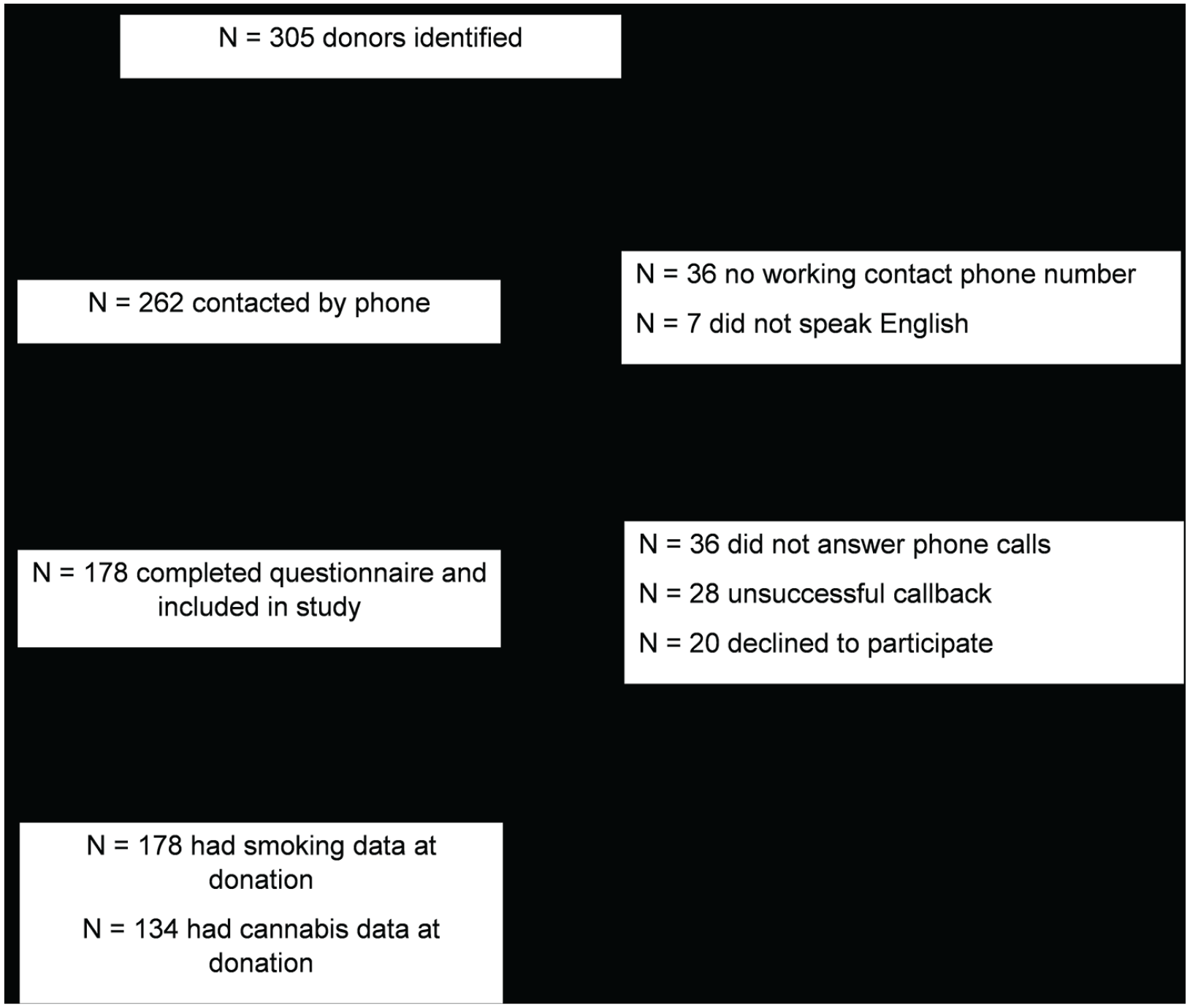
Study recruitment.
Characteristics of the Living Kidney Donor Population at Survey Completion, n = 178.

Missing data, n = 2.
Missing data, n = 1.
Cannabis use before and after kidney donation was available for 134 donors and is outlined in Figure 2. Among the 26 donors using cannabis after donation, 18 (69%) used cannabis less than once per month (but had used in the past 12 months) and 8 (31%) donors used cannabis at least monthly. The number of donors who used cannabis within the past 12 months (after donation) increased significantly from the time of donation (14.7% vs 6.7%; mean difference 8%; 95% confidence interval [CI], 0.9%-14.7%; P = .03). There was no statistically significant association between cannabis use in the past 12 months and donation era: for donation era before 2013 versus 2013-2016, odds ratio (OR), 0.67; 95% CI, 0.19-2.42; P = .55, and for donation era 2013-2016 versus 2017 or later, OR, 0.86; 95% CI, 0.31-2.43; P = .9.
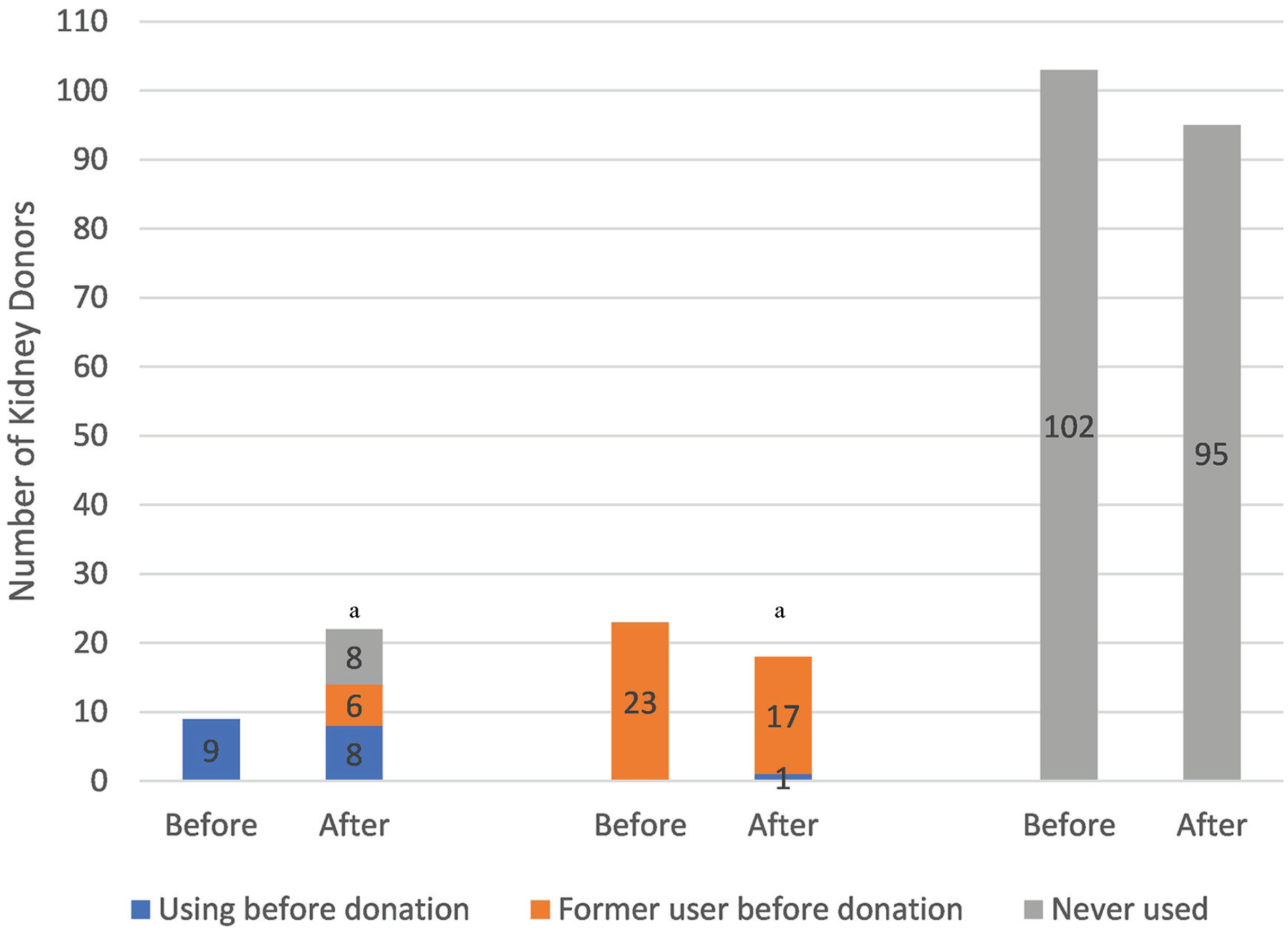
Cannabis use before and after kidney donation, n = 134.
Cannabis use in the past 12 months was statistically higher in non-married/common-in-law donors (OR, 3.40; 95% CI, 1.43-8.10; P < .01) and who had a higher household income (OR, 2.10; 95% CI, 0.90-4.91; P = .08), but only marital status was statistically significant on multivariate analysis (OR, 2.73; 95% CI, 1.05-7.11; P = .04; Supplementary Tables 1 and 2). Overall health and mental health assessment scores among cannabis users and non-users at survey completion were not significantly different. Cannabis users were not more likely to exceed the Canadian low-risk drinking guidelines or exercise below the Canadian physical activity.14,15 When asked about the impact of Canadian legalization of cannabis, 19 (11%) donors reported that they planned to use more cannabis.
Smoking status before and after donation is shown in Figure 3. A total of 74% (17 of 23) of smokers remained smokers after donation and 88% (53 of 60) who quit smoking before donation did not start smoking after donation. There was no statistical difference between number of smokers after kidney donation from before/at the time of donation (14.6% vs 12.9%; mean difference, 1.7%; 95% CI, –5.54% to 8.94%; P = .64). During the past 30 days prior to questionnaire completion, 16 (6%) donors reported smoking daily; 13 (6%) donors reported having tried to quit smoking in the past 12 months of survey completion.

Smoking before and after kidney donation, n = 178.
After donation, smoking was statistically higher among donors who were not married or not in a common-in-law relationship (OR, 3.00; 95% CI, 1.26-7.40; P = .02) and who had a higher household income (OR, 3.80; 95% CI, 1.50-9.80; P < .01) but was not statistically significant by age or gender univariate analysis (Supplementary Table 3). Overall health assessment scores among smokers were not significantly different (OR, 0.69; 95% CI, 0.25-1.89; P = .47) than non-smokers but mental health assessment scores were significantly worse among smokers (OR, 0.25; 95% CI, 0.08-0.75; P = .01). There was no association with smoking and exceeding the Canadian low-risk drinking guidelines but smokers were more likely to exercise an amount that met or exceeded the Canadian physical activity guidelines (OR, 2.58; 95% CI, 1.06-6.27; P = .04) compared with non-smokers. 15 However, none of these factors were statistically significant on multivariate analysis (Supplementary Table 4).
The mean (SD) CKD-EPI eGFR was 94.1 ± 17.3 mL/min/1.73 m2 at the time of kidney donation. The mean (SD) CKD-EPI eGFR was 66.5 ± 17.7 mL/min/1.73 m2 at last follow-up. There was no statistical difference in CKD-EPI eGFR at donation between non-smokers versus current and former smokers (mean difference, –0.36; 95% CI, –4.48 to 3.76; P = .86). There was also no statistical difference in CKD-EPI eGFR at last follow-up although numerically mean eGFR was lower in smokers (mean difference, 4.47; 95% CI, –0.75 to 9.69; P = .09). There was no statistical difference in CKD-EPI eGFR at donation (P = .91) and at last follow-up (P = .64) among current cannabis users versus former and non-cannabis users at the time of donation.
Discussion
In this retrospective cohort study of consecutive living kidney donors, we found a relatively low prevalence of cannabis use and cigarette smoking before and after donation. Cannabis use increased after donation. Cannabis use was associated with non-married/common-in-law donors, identifying a salient group for targeting screening and education around cannabis use.
Cannabis use in the Canadian general population had already been increasing with more than 190 000 newly registered medical cannabis users in Canada from June 2014 to June 2018, prior to its legalization in October 2018. 16 In our study, cannabis use among kidney donors within the past 12 months was 15% and was significantly higher after donation than at the time of donation; 10% of former and non-cannabis-using donors started using cannabis after donation. Donors in our study were also interested in increasing cannabis use. Similar to the study by Ruckle et al, 10 cannabis use did not affect kidney function at 3 years of donor follow-up.
Similar to our study findings, the overall smoking prevalence in the general Canadian population is reported to be 15% with 11% being daily smokers. 17 A retrospective, single-center study reported an overall reduction in smoking after donation at 1 year 6 and another study reported a nonsignificant reduction in smoking with 60% of their donors having less than 2-year follow-up after donation. 18 Close to half of our donors reported having tried to quit in the past year, as in the general population. 17 Post-donation cigarette smoking was statistically associated with non-married/common-in-law status, lower mental health scores, exercise, and household income only on univariate analysis. Multivariate analysis revealed no statistically significant association of these psychosocial factors to cigarette smoking. The lack of statistical association on multivariate analysis may be related to our small sample size. It is also possible that these psychosocial factors are inter-related. Of note, 5% of former and non-smokers at donation started smoking after donation. Unlike a larger study of kidney donors with shorter follow-up and different eGFR estimation, there was no statistical difference in CKD-EPI eGFR after donation among current and former smokers compared with non-smokers at the time of donation in our study. 4 This may be related to our smaller sample size and potentially underpowered study. Based on the SD of eGFR of 17.7 mL/min/1.73 m2 (from our data) and assuming a clinically significant difference of 3 mL/min/1.73 m2 between the 2 groups, we would require 548 patients in each group. Importantly, most smokers remained smokers after donation and most donors who quit smoking before donation did not restart after donation.
The strengths of our study include details around smoking and cannabis behaviors before and almost 5 years after kidney donation, the high survey response rate, and robust methodology. Recall bias was minimal given that smoking and cannabis use at the time of kidney donation was not dependent on recall. Our study also examined the associations of smoking and cannabis use to kidney function, psychosocial factors, and mental health—all of which have been identified as priorities to living kidney donors. 19 Limitations of our study include its retrospective nature and selection bias due to single-center study design. Given that we lacked consent to examine data for donors who did not complete the survey, it is possible that smokers were less likely to complete the survey. The number of cannabis users before donation was small. We cannot exclude social desirability bias. Most donors were evaluated prior to cannabis legalization in Canada in October 2018 and may have been less likely to report cannabis use due to fear of being declined for donation. Thus, these donors might have felt more comfortable reporting cannabis use during our survey administration in 2019. Missing cannabis data before donation may have been related to assessments done in earlier years when social work and nephrology consultation notes were not standardized in our donor program. Potential confounding variables, such the presence or absence of household members among non-married donors, were not assessed and may affect our results regarding the association of marital status and cannabis use. Smoking reports before donation may also have been subject to social desirability bias and stigmatization despite smoking not being an absolute contraindication to kidney donation at our center. Smoking is also defined as any amount of exposure without quantification in pack-years.
While data around kidney function among donors who smoke at the time of donation are mixed, kidney donor health maintenance behaviors are important for donor health and should be a prevention goal for the donor team. This is relevant as increasingly medically complex donor candidates come forward and are being accepted as donors. Current guidelines encourage smoking cessation prior to kidney donation, and there are no guidelines around cannabis use.20,21 Consequently, there is considerable variation around the acceptance of donor candidates who smoke and use cannabis.22,23 Smoking and cannabis use are not contraindications to kidney donation in our center and are considered on a case-by-case basis in the context of other medical and psychosocial factors. The donor team encourages smoking cessation prior to donation but no formal counseling or pharmacotherapy is provided. Given that most smokers continued to smoke after donation, donor candidates and donor programs must consider that this will remain a serious health risk after donation. This warrants education and support for donor candidates who smoke, to quit smoking prior to donation. Smoking is a modifiable risk factor so cessation may reduce cardiovascular and ESKD risks. Smoking cessation can also reduce future health-related risks regardless of kidney donation.
Regarding follow-up after donation, our center does not complete a focused assessment for health maintenance behavior review but this may be useful as smoking is associated with decreased health-related quality of life and donor death.3,24 Living kidney donation programs can support smoking cessation by counseling donors about the importance of cessation, directly connecting patients with local or regional smoking cessation programs, and consultation with their primary care physician for possible services offered by their primary care program. The efficacy of smoking cessation programs in the general population is established but studies are needed to determine whether smoking cessation strategies will affect long-term donor outcomes, including ESKD and mortality. 25 Given the small number of cannabis users in our study, its impact on kidney function remains unclear. Of concern, the prevalence of cannabis use increased after donation and donors were interested in increasing cannabis use but most donors were unable to quantify their current use. Thus, cannabis use should be determined before and after donation with education of the donor care team to address concerns and questions.
Conclusion
Cannabis use is more prevalent after kidney donation and may increase further with its recent legalization in Canada. Smoking rates among living kidney donors before and after kidney donation are similar to that of the general Canadian population. Most smokers remained smokers after donation and most donors who quit smoking before donation did not restart after donation. This warrants education and support for donor candidates who smoke, to quit smoking prior to donation. Smoking is a modifiable risk factor and donors should be provided with education and support to quit smoking to improve outcomes after kidney donation. Future multicentre, prospective studies can best identify the scope of smoking and cannabis use and whether interventions mitigate ESKD and mortality risk.
Supplemental Material
sj-pdf-1-cjk-10.1177_2054358121997243 – Supplemental material for Cannabis and Cigarette Use Before and After Living Kidney Donation
Supplemental material, sj-pdf-1-cjk-10.1177_2054358121997243 for Cannabis and Cigarette Use Before and After Living Kidney Donation by Ann Bugeja, Ieta Shams, Sophie Harris, Edward G. Clark, Kevin D. Burns, Manish M. Sood and Ayub Akbari in Canadian Journal of Kidney Health and Disease
Supplemental Material
sj-pdf-2-cjk-10.1177_2054358121997243 – Supplemental material for Cannabis and Cigarette Use Before and After Living Kidney Donation
Supplemental material, sj-pdf-2-cjk-10.1177_2054358121997243 for Cannabis and Cigarette Use Before and After Living Kidney Donation by Ann Bugeja, Ieta Shams, Sophie Harris, Edward G. Clark, Kevin D. Burns, Manish M. Sood and Ayub Akbari in Canadian Journal of Kidney Health and Disease
Supplemental Material
sj-pdf-3-cjk-10.1177_2054358121997243 – Supplemental material for Cannabis and Cigarette Use Before and After Living Kidney Donation
Supplemental material, sj-pdf-3-cjk-10.1177_2054358121997243 for Cannabis and Cigarette Use Before and After Living Kidney Donation by Ann Bugeja, Ieta Shams, Sophie Harris, Edward G. Clark, Kevin D. Burns, Manish M. Sood and Ayub Akbari in Canadian Journal of Kidney Health and Disease
Supplemental Material
sj-pdf-4-cjk-10.1177_2054358121997243 – Supplemental material for Cannabis and Cigarette Use Before and After Living Kidney Donation
Supplemental material, sj-pdf-4-cjk-10.1177_2054358121997243 for Cannabis and Cigarette Use Before and After Living Kidney Donation by Ann Bugeja, Ieta Shams, Sophie Harris, Edward G. Clark, Kevin D. Burns, Manish M. Sood and Ayub Akbari in Canadian Journal of Kidney Health and Disease
Footnotes
Acknowledgements
We thank the living kidney donors who participated in the study. We thank Diana DiPelino for ensuring accurate donor contact information.
List of Abbreviations
ESKD, end-stage kidney disease; eGFR, estimated glomerular filtration rate; CKD-EPI, Chronic Kidney Disease Epidemiology Collaboration equation; CI, confidence interval; OR, odds ratio; PROMIS, Patient-Reported Outcomes Measurement Information System.
Ethics Approval and Consent to Participate
The study protocol was approved by The Ottawa Hospital Health Science Network Research Ethics Board (Protocol ID 20190008-01H). A signed consent from participants was not required because of minimal risk to participants and survey completion was accepted by the Ethics Board as consent to participate.
Consent for Publication
We have the authors’ consent for publication.
Availability of Data and Materials
All data generated are included in this article.
Author Contributions
A.B. conceived and designed the study and wrote the initial manuscript. I.S. and S.H. acquired the data and performed initial data analysis. E.G.C., K.D.B., and M.M.S. provided critical feedback and helped shape the manuscript. A.A. performed data analysis and helped shape the manuscript. All authors approved the final manuscript and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. Data and materials are available for sharing by contacting
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Ann Bugeja received a research grant from LeoPharma. Manish Sood received a speaker fee from Astra Zeneca. Ayub Akbari received research support from Astra Zeneca and Otsuka.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.