
Abstract
Background:
Antibody-mediated rejection (AMR) is an important cause of kidney transplant loss. A new strategy requiring application of precision medicine tools in transplantation considers molecular compatibility between donors and recipients and holds the promise of improved immunologic risk, preventing rejection and premature graft loss.
Objective:
The objective of this study was to gather patients’ and caregivers’ perspectives on molecular compatibility in kidney transplantation.
Design:
Individual semi-structured interviews.
Setting:
The Centre hospitalier de l’Université de Montréal (CHUM) and McGill University Health Centre (MUHC) kidney transplant programs.
Participants:
Kidney transplant candidates, kidney transplant recipients, and caregivers.
Methods:
Twenty-seven participants took part in semi-structured interviews between July 2020 and November 2021. The interviews were digitally recorded, transcribed, and analyzed using the qualitative description approach.
Results:
Participants had different levels of knowledge about the kidney allocation process. They expressed trust in the system and healthcare professionals. They indicated that a fair organ allocation system should strive to maximize graft survival as it would decrease the demand for deceased donor kidneys and allow more patients to access transplantation. Molecular matching and precision medicine were seen as important improvements in the kidney transplant allocation process given their potential to improve graft survival and decrease the need for retransplantation. However, participants were concerned about increased waiting times that may negatively impact some patients upon implementation of molecular matching. To address these concerns, participants suggested integrating safeguards in the form of maximum waiting time for molecularly matched kidneys.
Limitations:
This study was conducted in the province of Quebec most of the participants were white and highly educated. Consequently, the results could not be generalizable to other populations, including ethnic minorities.
Conclusions:
Molecular matching and precision medicine are viewed as promising technologies for decreasing the incidence of AMR and improving graft survival. However, further studies are needed to determine how to ethically integrate this technology into the kidney allocation scheme.
Trial registration:
Not registered.
Introduction
Kidney transplantation is the best medical treatment for patients with end-stage kidney failure. 1 Kidney transplantation significantly improves patients’ quality of life and health status.2-4 Unfortunately, transplants do not last for the entire patients’ lifetime and result in eventual graft loss. For instance, in Canada, the 10-year graft survival rate is 58% for deceased donor kidney transplantation and 77% for living donor kidney transplantation. 5 One major cause of graft loss is antibody-mediated rejection (AMR) for which there are no well-proven effective therapies. Antibody-mediated rejection could occur early or late during the transplantation course.6-9 Antibody-mediated rejection is associated with the development and/or the presence of donor-specific antibodies (DSA) which occur when there is an immune recognition by the transplant recipient of non-self epitopes on human leukocyte antigens (HLA). 10
Worldwide, deceased donor kidney allocation algorithms strive to balance equity and medical utility. 11 In Canada, kidneys are allocated on a provincial basis. The allocation scheme differs from one province to another, but time spent on dialysis, pediatric priority, HLA compatibility and medical urgency are criteria considered by the different organ donation organizations.12-16 In addition, deceased donor kidneys are shared between provinces for highly sensitized patients (calculated Panel Reactive Antibocy (cPRA) > 95%) through a national registry managed by Canadian Blood Services. 17
In recent years, molecular-based matching was proposed for kidney allocation.18,19 This is a more precise method of HLA compatibility assessment, which consists of breaking down each HLA at the molecular level and considering the combination of amino acid polymorphisms informing antibody development. 20 Molecular compatibility could decrease the development of DSA by the recipient and, therefore, the incidence of AMR. 21 The Genome Canada Transplant Consortium set an objective for itself to develop a national molecular-compatibility-based kidney allocation program to decrease the incidence of acute rejection. 19 While molecular compatibility may improve long-term outcomes for kidney transplant recipients (KTRs), it could also result in decreased access to transplantation in patients who have a distinct molecular profile in comparison with the donor pool, raising concerns around fairness. 11
Patients and caregivers share important perspectives on the issue of how one should distribute a scarce resource such as a deceased donor kidney fairly. First, any new policies affecting organ allocation may affect their chances of being transplanted. Also, patients’ preferences on organ allocation are shaped by their medical concerns and their experiential knowledge when awaiting an organ and/or living with the consequences of AMR. Different studies have shown that patient preferences in terms of organ allocation, such as deservingness, are not necessarily aligned with existing allocation criteria.22,23
This study is part of a larger research project, CanPREVENT AMR, the objective of which is to use genetic technologies to improve donor-recipient compatibility and reduce the risks of AMR. 19 The CanPREVENT AMR project also aims to document various stakeholders’ perspectives on the ethical issues related to molecular matching in deceased kidney allocation. We have previously reported the Canadian transplant professionals’ perspectives on precision medicine and molecular matching. 24 The objective of this study was to gather Canadian KTRs’, kidney transplant candidates’ (KTCs’), and caregivers’ perspectives on precision medicine and molecular matching in kidney transplantation, with the vision of informing future allocation rules when incorporating molecular compatibility into deceased donor kidney transplantation in Canada.
Methods
This study was exploratory in nature. We used the consolidated criteria for reporting qualitative research checklist. 25 We conducted individual semi-structured interviews to gather KTRs,’ KTCs’, and caregivers’ perspectives on precision medicine and molecular compatibility in kidney transplantation. The Centre hospitalier de l’Université de Montréal (CHUM) and the McGill University Health Centre (MUHC) research ethics boards approved the study and all participants provided their informed consent (CHUM CE20.054, MP-02-2021-9021; MUHC MEO-02-20221-6938).
The recruitment and interviews were carried out between July 2020 and November 2021. Convenience and purposive sampling 26 were used to recruit KTRs, KTCs, and caregivers. Participants were recruited among the KTCs and KTRs followed at the CHUM and at the MUHC, 2 transplant programs located in the Canadian province of Quebec. Figure 1 summarizes the recruitment process. To be included in the study, participants had to be adults and speak English or French. Invitation letters were sent to KTRs and KTCs. Flyers about the study were also distributed at the CHUM and the MUHC transplant clinic, and a research coordinator approached patients during the transplant clinic. Caregivers were invited to participate through KTRs and KTCs. Moreover, we used social media to recruit patients through the Facebook pages of the Canadian Donation and Transplantation Research Program, the Kidney Foundation of Canada and the CHUM.

Recruiting flow chart.
Forty KTRs, 9 KTCs, and 3 caregivers were interested in having more information about the study and were contacted by the research team. Of these 52 individuals, 8 KTRs declined to participate due to time constraints and personal reasons; 5 KTRs could not be reached; and 9 KTRs, 2 KTCs, and 1 caregiver did not send back a signed informed consent form. Two KTRs and 1 KTC requested to participate with their caregiver (spouse). Of the 30 participants who consented to participate, 2 KTRs and 1 KTC could not be reached to schedule an interview, meaning 27 patients and caregivers participated in this study: 16 KTRs, 6 KTCs, and 5 caregivers (Figure 1).
Twenty-one participants took part in an individual interview: 14 KTRs, 5 KTCs, and 2 caregivers. Two KTRs and 1 KTC took part in an interview with their respective caregivers. Six interviews were conducted by phone and 18 by videoconference, 17 in French and 7 in English, by a male member of the research team (F.B.) who had no clinical relationship with the participants. French interview excerpts were translated by a professional agency. The interviews lasted around 38 (28-61) minutes and were digitally recorded and transcribed. Each participant received CAN$30 as a financial compensation for their time. The interview transcripts were sent to all participants for review and approval.
Interviews began with a brief PowerPoint presentation about molecular matching and the objectives of the study (see Supplementary Material). The objective of the PowerPoint presentation was to provide background information on molecular matching and to facilitate participation in discussion. Participants had the opportunity to ask questions about the study before the interviews started. The issues covered during the interviews were outlined in an interview guide with open-ended questions that was developed by the research team and pre-tested by 2 patients for question length and clarity, in both English and French. The questions addressed the following themes: (1) knowledge and perspectives on the current organ allocation system, (2) the role of molecular matching in deceased organ and living kidney donation, (3) informed consent and molecular compatibility, and (4) sociodemographic data (see Supplementary Material). Consistent with qualitative methodology, the interview guide was modified during the study as new topics emerged from the interviews. 26
We used a qualitative description approach to describe the perspectives of patients and caregivers on molecular matching in kidney transplantation.27,28 The goal of this pragmatic approach was to stay close to the data and provide a comprehensive summary of the topic studied, 28 using thematic analysis.26,29 The latest version of NVivo (Lumivero) software was used to facilitate the analysis. Prior to coding the verbatim, the research team created the initial coding frame based on the interview guide and a review of the literature. New codes were added to the coding frame based on the interview content. The research team met frequently to discuss the coding frame and data analysis. F.B., a male researcher with more than 10 years of experience conducting qualitative research in the field of organ transplantation ethics, coded the interviews and no new codes were created after the 20th interview. The number of participants allowed for data saturation.30,31 A female independent researcher (A.A.) who is completing her PhD in bioethics and has worked in our research team in ethics and organ transplantation for more than 5 years and has experience in qualitative methods coded 37% of the raw data with the rate of coding agreement assessed at 96% and disagreements were discussed. Coded quotes were then organized by themes and subthemes.
Results
Participants’ Characteristics
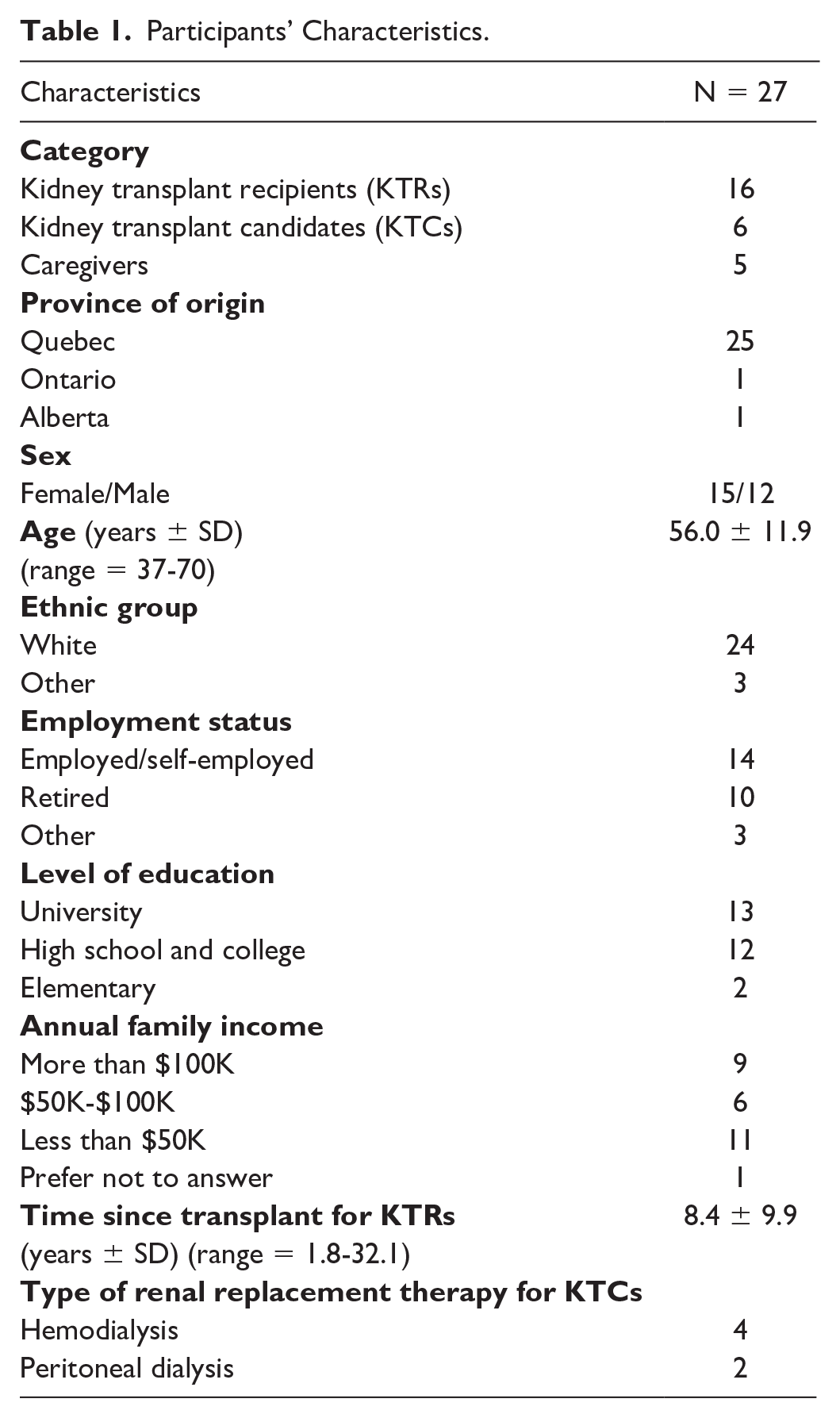
Sixteen KTRs, 6 KTCs and 5 caregivers participated in the study. Fifteen participants were women and most of them were white (89%). Participants were in their fifties and half of them had a university degree. Notably, more than half of the participants (52%) were currently employed and 56% had an annual family income of more than $50,000. Table 1 summarizes participants’ characteristics.
Participants’ Characteristics.
Perspectives and Knowledge of the Current Allocation System (Table 2)
Perspectives and Knowledge of the Current Allocation System.

Participants had some limited knowledge about the current organ allocation system. They were aware of some criteria about the current organ allocation system, such as the HLA and blood group compatibility. Some of them mentioned needing more information and transparency. One caregiver mentioned the need to know the patient’s queue place and average waiting time.
Participants trusted health professionals and organ donation organizations in their ability to develop a fair allocation system for deceased kidney donor. When questioned specifically on kidney allocation criteria, most participants viewed compatibility between the donor and the recipient as the most important criterion. For KTCs, time spent on dialysis as well as any factors that could affect graft survival, such as non-adherence, were viewed as important criteria. For KTRs and caregivers, transplant recipients’ lifestyle habits were also viewed as a factor to take into account when allocating deceased donor kidney. Participants also believed that a fair allocation system should strive to maximize graft survival as it would decrease the demand for deceased donor kidney and would allow more patients to have access to transplantation.
Perspectives on Precision Medicine and Molecular Matching in Kidney Transplantation (Table 3)
Perspectives on Precision Medicine and Molecular Matching in Kidney Transplantation.

Many participants viewed precision medicine and molecular matching as an interesting avenue to explore as it could improve graft survival, prevent graft rejection, and make the healthcare system more cost-effective. That being said, they also expressed concerns regarding this new technology. Indeed, some participants questioned whether molecular matching could prevent some patients from having access to kidney transplantation or increase waiting time for other patients. They feared that precision medicine could discriminate and disadvantage some patients.
Use of Precision Medicine and Molecular Matching in Living Kidney Donation (Table 4)
Use of Molecular Matching in Living Kidney Donation.

Precision medicine and molecular matching could also be used in living kidney donation to choose the better-matched living donor or to invite compatible pairs to enter into kidney paired donation to have a molecular-matched kidney. Most participants were open-minded about including molecular matching in living kidney donation and inviting compatible pairs in kidney paired donation. However, they believed that participation of compatible pairs in kidney paired donation should be voluntary and not mandatory. That being said, some of them believed that certain participants would be reluctant to participate in kidney paired donation to have a better-matched kidney, preferring to donate or receive a kidney from their loved ones. They also questioned whether molecular matching in kidney paired donation could increase the waiting time for a kidney transplant.
Mitigation Strategies and Recommendations for Implementing Precision Medicine and Molecular Matching in Kidney Transplantation (Table 5)
Mitigation Strategies and Recommendations for Implementing Precision Medicine and Molecular Matching in Kidney Transplantation.

As mentioned above, the possibility that molecular matching and precision medicine could increase waiting time for a kidney transplantation for some patients was a major concern. To mitigate the increased waiting time for a molecular-matched deceased donor kidney, some participants recommended setting a maximal waiting time. The maximum acceptable additional waiting time for a molecular-matched kidney would be 4 years or 1 or 2 years over the average waiting time. After this delay, if the KTC did not receive a molecular-matched deceased donor kidney, they would be prioritized to receive a deceased donor kidney based on the former allocation criteria. Other participants would, however, prefer to receive a non-molecularly matched kidney to be transplanted more rapidly and stop dialysis.
Some participants addressed the difficult situation of highly sensitized patients who are hard to match in the current allocation system. These patients suffer from high anxiety waiting for the perfect match, worrying they will never be able to get a transplant. Some participants suggested that highly sensitized patients should not be considered for precision medicine, as it might further complicate finding suitable matches. Other participants suggested that these hard-to-match patients should still have access to current programs, such as national sharing of kidneys, while being considered for molecular-matched deceased donor kidneys simultaneously.
One important recommendation was about informed consent and education about precision medicine and molecular matching in kidney transplantation. Patients wanted to be informed on how molecular matching will increase their graft survival and decrease the risk of rejection. Patients also want to be informed about the chances of finding a molecular-matched kidney in an acceptable timeframe. Percentages were described as a good way to communicate risk. Participants also believed that the information provided should be adapted to every patient’s situation and preferences.
Lastly, although participants found that molecular matching and precision medicine are interesting avenues, they also stressed the need to pursue research to develop renal replacement therapy that would improve patients’ health and quality of life. Even if molecular matching and precision medicine could improve graft survival, participants also highlighted the need to support patients and caregivers throughout their transplant journey.
Discussion
This is the first study to describe KTRs,’ KTCs’, and caregivers’ perspectives on the integration of molecular matching and precision medicine in deceased donor kidney allocation and in living kidney donation. Most participants had a positive view on the integration of molecular compatibility into organ allocation schemes as it has the potential to improve graft survival, prevent retransplantation, and, therefore, decrease the shortage of organs available for transplantation. They were, however, concerned by the possibility of decreasing access to transplantation for certain groups of patients and increasing waiting time when seeking molecularly compatible kidneys.
The balance between medical utility and fairness is a cause for ongoing tension in the field of organ allocation. Most allocation systems try to balance both utility and fairness.11,32 Our study has shown that participants truly value graft survival. For most participants, a fair deceased kidney allocation system should take into account compatibility between the donor and the recipient as well as other factors that could affect future graft survival, including lifestyle behaviors. These results are aligned with other studies, which have shown that for patients life gained after transplantation, and rejection prevention, are important determinants in the design of deceased donor allocation schemes.22,33,34 For some patients who participated in a qualitative study, medical compatibility between the donor and the recipient was an essential prerequisite. 33 The high value given by patients to medical utility and graft survival differs from the results of our previous study looking at transplant professionals’ views on molecular matching, prioritizing fairness over utility in organ allocation. 24 A recent worst-off scaling survey conducted with community members in Australia showed that the most valued principle was related to equity and fairness. In this study, participants prioritized deceased kidney transplantation to patients who had waited the longest, were hard to match, and those deemed the sickest. 35
Participants in our study were open-minded about including molecular compatibility in kidney paired donation. Wide-scale buy-in prioritizing the enrollment of molecularly compatible pairs into the kidney paired donation program is expected to further decrease immunological risk. Recently, Jackson et al invited the transplant community to revisit the existing paradigm on compatibility in living donation. For these authors, compatibility should be viewed more broadly than ABO/HLA compatibility and include molecular matching. 36 However, participants in our study found that participation of compatible pairs in the kidney paired donation program should be considered voluntary rather than mandatory. This is aligned with our previous study, which showed that the prospect of receiving a better kidney was a factor that increased the willingness of compatible pairs to participate in kidney paired donation; however, participants also expressed a strong desire to donate or receive from their intended donor or recipient. 37
Our study participants also made interesting recommendations around safeguards when incorporating precision medicine or molecular matching in deceased organ allocation. First, they proposed that a maximal waiting time be set when awaiting a molecularly compatible kidney. Should this maximal waiting time be exceeded, the recipient should be prioritized for transplantation according to allocation rules excluding molecular compatibility. They also recommended the development of educational tools informing candidates on their likelihood of accessing molecularly compatible kidney within a given timeframe. Given the complexity of molecular HLA compatibility, transplant professionals may experience challenges in communicating the opportunities and challenges expected when incorporating them into organ allocation. 32 Future studies are needed to explore the most appropriate educational tools on this topic.
A recent Canadian public deliberation process was conducted to define the guiding principles for incorporating molecular compatibility into kidney allocation schemes. Participants in this public deliberation agreed with the inclusion of molecular-based matching into deceased donor kidney allocation. However, they believed that there should also be safeguards and flexibility must be exercised to ensure fairness in organ allocation. They also recommended that patients with declining health have access to a non-molecularly matched kidney for quicker access to kidney transplantation. It is also important to develop a comprehensive educational program and to reassess the outcomes of precision medicine in organ allocation in 5 years. 38 These recommendations are aligned with our participants’ perspectives.
Limitations of our study include a small sample size, albeit it is important to recall that data saturation was achieved. Also, most study participants were from the province of Quebec, white and highly educated. Moreover, it was often proposed to include precision medicine in kidney transplantation for pediatric patients first to prevent the development of DSA, which would make future kidney transplantation harder to realize for increased immune sensitization. 39 Accordingly, another limitation of this study is the lack of parents’ perspectives on molecular compatibility implementation for pediatric patients. It is also possible that the PowerPoint presentation used to inform patients about molecular matching could have biased participants’ answers. Finally, it is possible that the results of this study are not generalizable (limiting external validity) and not representative to all Canadian KTRs’, KTCs’, and caregivers’ views on molecular matching. Importantly, however, our findings are congruent with perspectives of the Canadian public arising from prior public deliberation efforts. 38 Finally, while questions regarding the ethical issues related to molecular matching and kidney allocation are universal, as kidney allocation and clinical practices vary by country, our results may not be applicable to other parts of the world.
Conclusion
This is the first study to report KTRs’, KTCs’, and caregivers’ perspectives on the integration of precision medicine in deceased and living donor kidney transplantation. While participants viewed precision medicine as a promising avenue that could decrease rejection and the need for subsequent retransplantation, they were concerned about the possibility of discriminating against some groups of patients and decreasing access to transplantation for certain patients. To address these concerns, participants suggested the implementation of a maximum waiting time to receive a molecularly compatible kidney and the development of comprehensive educational tools for providing information about this type of allocation as well as the chances of receiving a molecularly compatible kidney within a specified timeframe. Our findings also indicate a need to develop tools for transplant professionals that can enable them to explain the intricacies and nuances of molecular matching to patients. We believe our findings pave the road for future patient-centered integration of molecular compatibility in the Canadian kidney allocation criteria.
Supplemental Material
sj-docx-1-cjk-10.1177_20543581251342440 – Supplemental material for Canadian Kidney Transplant Recipients’, Transplant Candidates’, and Caregivers’ Perspectives on Precision Medicine and Molecular Matching in Kidney Allocation: A Qualitative Analysis
Supplemental material, sj-docx-1-cjk-10.1177_20543581251342440 for Canadian Kidney Transplant Recipients’, Transplant Candidates’, and Caregivers’ Perspectives on Precision Medicine and Molecular Matching in Kidney Allocation: A Qualitative Analysis by Fabian Ballesteros, Aliya Affdal, Mohamad Issa, Marie-Françoise Malo, Savannah-Lou Cochran-Mavrikakis, Carina Sancho, Stirling Bryan, Paul Keown, Ruth Sapir-Pichhadze and Marie-Chantal Fortin in Canadian Journal of Kidney Health and Disease
Footnotes
List of Abbreviations
AMR, antibody-mediated rejection; cPRA, calculated panel reactive antibody; CHUM, Centre hospitalier de l’Université de Montréal; MUHC, McGill University Health Centre; DSA, donor-specific antibody; HLA, human leukocyte antigen; KTC, kidney transplant candidate; KTR, kidney transplant recipient.
Author Contributions
F.B. participated in the conduct of the research and the data analysis, and in the writing of the manuscript. A.A. participated in the conduct of the research and the data analysis, and in the writing of the manuscript. M.I. participated in the writing of the manuscript. M.-F.M. participated in the conduct of the research and the data analysis, and in the writing of the manuscript. S.-L.C.-M. participated in the data analysis and in the writing of the manuscript. C.S. participated in the data analysis and in the writing of the manuscript. S.B. participated in the research design and in the writing of the manuscript. P.K. obtained the research funding, participated in the research design and in the writing of the manuscript. R.S.-P. obtained research funding, participated in the research design, conduct of research, and in the writing of the manuscript. M.-C.F. participated in the research design, in the conduct of the research and the data analysis, and in the writing of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research project was funded by the Genome Canada Large Scale Applied Research Program Award “Precision Medicine CanPREVENT AMR,” funded by Génome Québec, Genome British Columbia, Genome Alberta, and Canadian Institutes of Health Research. R.S.-P. and M.-C.F. are Fonds de recherche du Québec—Santé research scholars. They are also Canadian Donation and Transplantation Research Program investigators. We want to thank all those who took the time to participate in this study.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.