
Abstract
Purpose of program:
The ongoing shortage of organs for transplant combined with the highest prevalence of end-stage kidney disease (ESKD) in Canada has resulted in long wait times for a deceased donor transplant in Manitoba. Therefore, the Transplant Manitoba Adult Kidney Program has ongoing quality improvement initiatives to expand the deceased donor pool. This clinical transplant protocol describes an age-targeted program intended to increase the use of transplants with a kidney donor profile index (KDPI) >85 by allocating them to suitable pre-consented recipients age ≥65 with low wait times. The goal is to improve survival and quality of life for older recipients by maximizing a previously under-utilized donor pool.
Sources of information:
Scoping literature review; Transplant Manitoba deceased donor audit; and key stakeholder engagement with patient partners, inter-disciplinary health care providers, and health system leaders.
Methods:
The alternative donor pool criteria include deceased donor kidneys with KDPI 86-100 or another concern for graft longevity but are otherwise suitable for transplantation. Patients with no living donor, age ≥65, low wait times and otherwise eligible for transplant listing will be educated, and if suitable, pre-consented for the age-targeted program. All patients remain eligible for a standard criteria donor according to the local allocation criteria. The age-targeted program waitlist follows the same provincial allocation rules using wait time, panel reactive antibody (PRA), and human leukocyte antigen (HLA) match points for determining rank order. If an age-targeted recipient experiences early graft loss from a KDPI 86-100 kidney within 12 months from transplant, their cumulative wait time, including time with the transplant, will be reinstated upon relisting.
Key findings:
Transplant Manitoba’s provincial allocation rules do not permit bypassing top of the list recipients for kidney offers; therefore, transplant providers were previously reluctant to utilize KDPI 86-100 donor kidneys to top of the list recipients eligible for higher quality kidneys. This age-targeted program facilitates allocation of KDPI 86-100 kidneys to suitable older pre-consented recipients with low wait times, who may obtain a survival and quality of life benefit from these transplants. This approach expands the utilized deceased donor pool to benefit all Manitobans awaiting a deceased donor kidney transplant.
Limitations:
This program was launched in January 2023, and there are no data reported on outcomes given the small numbers and abbreviated follow-up.
Implications:
The goal of this quality improvement project is to improve access to deceased donor kidney transplantation for Manitobans with ESKD. This program was developed with patient and provider feedback, including multimedia patient education materials which may be helpful for other programs. We anticipate this program is a safe and effective way to expand access to deceased donor kidney transplantation using a previously under-utilized donor pool.
Introduction
Avoiding the discard or non-utilization of potentially transplantable deceased donor kidneys is critical to reducing the chronic organ shortage for kidney transplant. 1 Concern over donor quality is a common reason for discard or non-utilization. The kidney donor profile index (KDPI) is a measure of kidney quality and increasing KDPI is associated with risk of discard, with some studies reporting a 50% discard rate for KDPI >85 kidneys. 2 Prior to this clinical transplant protocol, KDPI >85 kidneys were not used from donation after circulatory death (DCD) donors by Transplant Manitoba and those from neurological determination of death (NDD) donors were allocated only rarely through routine allocation to recipients over the age of 60 without a formal pre-consent process.
There is mounting evidence that for many patients with end-stage kidney disease (ESKD) accepting a KDPI >85 transplant is associated with improved long-term survival compared with remaining on dialysis indefinitely or remaining on dialysis to wait for a subsequent KDPI <85 transplant.3-5 The benefit of accepting a high KDPI transplant is more pronounced for patients who are older, have long anticipated wait time, or have comorbidities such as diabetes that increase their risk of dying or being removed from the wait list prior to receiving a transplant.3-5 The maximum benefit of a high KDPI transplant appears to be associated with preemptive transplant5,6; the survival advantage is likely driven by a reduction in wait time and avoiding the morbidity and mortality associated with accumulating dialysis vintage. A recent economic evaluation of high KDPI transplants using the Manitoba context suggests that increasing the use of such transplants will offer cost savings, improved quality of life, and greater overall survival for patients aged 60 and older. 7 For context, in the last 5 years, approximately 50% of our deceased donor transplant recipients were over the age of 60 and 25% were over the age of 65. Among the candidates active on our current waitlist, approximately 25% are over the age of 60 and 10% over the age of 65.
Transplant Manitoba’s provincial allocation rules were designed to balance justice (prioritizing those with the longest waiting time) and utility (to improve kidney transplant outcomes, with HLA and age matching), and to be transparent and accountable for this scarce resource. Prior to this clinical transplant protocol, it was not possible to direct KDPI >85 kidneys to older recipients with lower waiting times who were most likely to benefit, which led to significant under-utilization of this deceased donor pool. In this program report, we describe a new “age-targeted kidney transplant program” designed to increase the use of high KDPI transplants and to allocate them safely and efficiently to the patients most likely to benefit.
Sources of Information
Transplant Manitoba Deceased Donor Audit
Winnipeg is the largest urban center in Manitoba, capital city of the province, and location of the province’s multiple tertiary care centers. Transplant Manitoba—Gift of Life operates under a mandatory referral policy whereby the organ donor coordinator must be notified of any patient in a Winnipeg intensive care unit or emergency department who is ventilated and for whom an end of life discussion is planned.
Annual deceased donor audit data are available to track the number of referrals and the outcome of the referrals, including whether or not the potential donor ultimately proceeds to donation. If the referral does not lead to donation, the reason is coded in the audit data. For purposes of this project, we identified how many referrals were declined due to KDPI in the 3-year period of 2018 to 2020 as an estimate of potential donor pool expansion with routine use of high KDPI kidneys.
We determined that approximately 35 of every 1000 referrals were declined by the transplant nephrologist due to high KDPI before the donor underwent full medical assessment and family or next of kin were approached for consent. Given that, by definition, the high KDPI donor tends to be older with more comorbidities, we assumed that had these donors been considered approximately 50% of them would also be medically suitable to donate. The donor audit data suggest that approximately 35% to 40% of suitable referred donors do not donate due to family decline and another 25% to 30% due to other barriers such as DCD donor non-progression to asystole, donor instability, or other medical issues discovered after referral. Therefore, we estimated that 35% of the medically suitable high KDPI donors would successfully donate 2 single kidneys for transplantation providing an additional 12 single kidney transplants per 1000 referrals. This would represent an 11% increase in the deceased donor pool compared with the actual transplant rate of 108 single kidney transplants per 1000 referrals measured in that same time period. These calculations were used to support the value of a high KDPI program in Manitoba and justify the resources used to design and implement the clinical protocol described in this report.
Provider Engagement
Two provider advisory committees were created to inform this protocol. Committee members were recruited through convenience sampling by sending them an electronic invitation letter describing the goal of creating a new kidney transplant program to expand the donor pool and identifying them as a health care provider who works with patients who may benefit from such a program. One committee was considered a “chronic kidney disease (CKD) provider” committee and was made up of 1 general nephrologist from each of the 3 Winnipeg hospitals with dialysis programs and 1 registered nurse practicing in a renal health clinic. The second committee was considered a “kidney transplant provider” committee and was made up of 1 transplant nephrologist, 1 registered nurse practicing in a post-kidney transplant clinic, 1 transplant coordinator practicing as a deceased donor coordinator and a pre-transplant recipient coordinator, as well as a social worker with experience working with patients pre-kidney and post-kidney transplant.
Four virtual meetings were held over Zoom with each provider committee between September 2021 and April 2022. The CKD and transplant provider committees met separately due to scheduling conflicts. The primary author (AT) led all the meetings. Committee meetings followed an unstructured conversational format. Topics discussed included, but were not limited to, the background literature supporting high KDPI transplants, the perceived need for such a program locally, patients who may be most interested and/or most likely to benefit, language and terminology to be used, inclusion and exclusion criteria, and the development of patient and provider educational material. All provider committee members endorsed the final version of the protocol reported in this article. One additional meeting was held with 2 transplant surgeons in April 2022 to obtain their endorsement of the program as well.
Patient Engagement
To ensure the patient perspective was incorporated into the design of this program, a patient advisory committee was also formed with Research Ethics Board approval (University of Manitoba, HS25240, H2021: 388). Patient committee members were recruited through convenience sampling. Each provider committee member was asked to submit the names of 2 or 3 patients who fit the following criteria:
55 years or older with other medical conditions (eg, diabetes) or 65 years or older and otherwise healthy, and
already have a kidney transplant, are on the waitlist for a kidney transplant, or may need to be on dialysis or get a transplant in the future.
Potential patient committee members were then mailed an invitation letter, followed by a phone call from a member of the program team. Eight individuals aged 55 to 74 years joined the patient advisory committee. There were 5 men and 3 women; 2 patients had a functioning kidney transplant, 1 patient had CKD G5ND, and 5 patients were receiving kidney replacement therapy (KRT; 3 in-center hemodialysis, 1 peritoneal dialysis, 1 home hemodialysis).
Five virtual meetings were held over Zoom between September 2021 and June 2022. Patient members were remunerated for their time. The primary author (AT) led all the meetings. Committee meetings followed an unstructured conversational format. Topics discussed included, but were not limited to, the background literature supporting high KDPI transplants, the acceptability of such a program to patients, language and terminology to be used, inclusion and exclusion criteria, and the development of patient educational material. All patient advisory committee members endorsed the final version of the protocol reported in this article.
Program Structure
Guiding Principles
The patient and provider committees identified several overarching themes to be incorporated into the design of a new age-targeted program including:
There are other transplant programs routinely using KDPI >85 transplants at higher rates than Manitoba with outcomes that are acceptable to patients and providers.
The benefits of high KDPI transplants are more established in older patients who receive a transplant with less dialysis vintage than would be required to receive a lower KDPI transplant.
A minimum age requirement is acceptable to patients and providers, primarily to facilitate ease of allocation and achieve lower wait times by maintaining a smaller pool of those recipients most likely to benefit.
Individual patient motivation and risk tolerance for transplant vary, from hoping for improved overall survival to accepting reduced survival for an opportunity to avoid dialysis. Therefore, strict recipient criteria (beyond age) to participate in a high KDPI transplant program were not acceptable. General guidance on which patients should be encouraged was welcomed.
Alternative Donor Pool Donors
Deceased donor kidneys considered viable for transplantation but with characteristics that may be associated with reduced graft longevity will be assigned to the alternative donor pool. Transplantation with such a kidney may be considered less than ideal for a candidate at the top of the standard waiting list, but does not in itself warrant discard or non-utilization, and may provide a survival and quality of life benefit to the right recipient. Therefore, the term “alternative donor pool” was agreed upon by the patient and provider committees as acknowledging the characteristics of the donors in this program are different than the current deceased donor pool in Manitoba, but was felt to have a neutral tone that was not dissuasive nor euphemistic.
Alternative donor pool inclusion criteria
KDPI >85 kidneys, regardless of neurologically determined death (NDD) or donation after cardiac death (DCD) status.
KDPI <85 kidneys, if there are other donor characteristics which raise concern for graft longevity. In such instances, assignment to the alternative donor pool is at the discretion of the transplant nephrologist, the reason for assignment must be clearly documented, and such assignments will be reviewed annually by the program to ensure appropriate use of the alternative donor pool.
Alternative donor pool exclusion criteria
Deceased donor kidneys with concerning features other than those related to “donor quality” or graft longevity, such as increased malignant or infectious risk deemed not suitable for use in the standard waiting list.
Alternative donor considerations
There is no definitive evidence to support a KDPI threshold at which donor kidneys should be discarded or not used. The transplant nephrologist should use additional caution/consideration for KDPI >97 offers, and especially when the KDPI is 100. This is due to the non-linear nature of the KDPI and risk of graft failure, especially with KDPI >97. In such circumstances, direct calculation of the kidney donor risk index (KDRI) 8 may be helpful. Consideration of other clinical features not captured by the KDRI may also be helpful in deciding to accept or decline the offer, but there is limited evidence to support specific features.
There is no definitive evidence to support a KDPI threshold at which deceased donor kidneys should only be offered as dual kidney transplant (both kidneys to 1 recipient). There are, however, numerous publications reporting excellent recipient outcomes for very high KDPI dual kidney transplants.9-11 Deceased donor kidneys deemed not appropriate for assignment to the alternative donor pool as single kidney transplants should be considered for assignment as dual kidney transplants prior to being discarded or declined.
There is limited evidence regarding the interaction between cold ischemic time (CIT) or warm ischemic time (WIT) and KDPI. As with any deceased donor transplant, minimizing CIT and WIT is important in preventing delayed graft function (DGF), but the relationship between ischemia time and long-term outcomes is less clear.12-15 Therefore, the Transplant Manitoba clinical protocol will be followed for management of DCD donors. For DCD donors with KDPI >85 and/or surgical barrier to retrieval (eg, multiple prior surgeries, abdominal obesity), the maximum time from withdrawal of life-sustaining therapy to death is 120 minutes. The DCD donation attempt will be stopped if the agonal time is >30 minutes, with agonal phase defined as a persistent systolic blood pressure ≤50 (sustained for at least 2 minutes) until the start of asystole. 16
Age-Targeted Program Candidates
Living kidney donor transplant is always recommended as a first-line option, and this program is only applicable for those who are suitable for transplant but do not have a living donor. The candidate who will benefit most from the age-targeted program and accepting of the relevant trade-offs in terms of graft longevity is an older recipient facing a long wait to the top of the standard deceased donor transplant list. The eligibility criteria were designed to be inclusive, but also acknowledge that the highest benefit will come from reducing wait time as much as possible. This means restricting access to the alternative donor pool may be necessary to prevent long wait times within the age-targeted program, which would reduce the net benefit and increase the risk to patients. The eligibility criteria will be reassessed periodically as the supply and demand for alternative donor pool kidney transplants change over time.
Other recipient factors considered by centers experienced in transplanting high KDPI kidneys include good functional status pre-transplant, adequate cardiovascular fitness to tolerate a prolonged episode of DGF, and ability to tolerate reduced nephron mass (ie, patients with very high body mass index [BMI] often excluded).17-19 Compared with receiving a lower KDPI transplant, the risks associated with receiving a high KDPI transplant may include reduced graft survival, higher rates of DGF, and potentially higher rates of primary non-function (PNF), assuming all other factors in the transplant are held similar.12,20 Through thoughtful recipient selection and purposefully allocating high KDPI transplants to patients with as little wait time as possible, these risks should be minimized or offset, but to what degree remains uncertain.
Owing to the possibility of pre-emptive transplantation through the age-targeted program, eligible patients who are not yet on dialysis but are aged ≥63 with a 2-year kidney failure risk equation (KFRE) >20% should start their transplant evaluation so they can be ready for potential pre-emptive age-targeted transplant by age 65. Similarly, patients ≥64 years will have their transplant work up expedited where possible if the nephrologist indicates they may be a good candidate for the age-targeted program.
Age-targeted program recipient inclusion criteria
A recurrent theme identified through engagement with the patient and provider partners was that individual patient goals for transplant and risk tolerance vary. Strict criteria, outside of age, were not recommended but rather general criteria to guide the shared decision-making were developed. The clinical criteria comprising groups 1, 2, and 3 below are meant to help direct the conversation and the strength of the recommendation by the transplant nephrologist to consider enrollment in the age-targeted program, but are not meant to be interpreted as strict criteria for inclusion or exclusion.
Inclusion criteria
Age ≥65 years; and
Transplant eligible; and
CKD G5ND with a 2-year KFRE ≥50% or treated with KRT; and
Clinical factors: Group 1 criteria; or Group 2 criteria; or Group 3 criteria when the anticipated wait time to transplant may be significantly reduced through the age-targeted program and is done in the context of shared decision-making with the patient.
BMI <30; and
An anticipated wait time for standard list greater than 3 to 4 years; and
Good functional status
BMI <40; and
No group 3 criteria (below).
BMI >40; or
Poor functional status / rehabilitation potential; or
Diabetic with previous coronary artery disease (CAD), *unless the anticipated wait time to transplant will be significantly reduced through this program; or
Approaching the top of the standard list.
*This recommendation is based on 1 observational study showing increased mortality in diabetic recipients with CAD who received a high KDPI transplant compared with a low KDPI transplant, and similar mortality in the high KDPI group compared with a reference group who remained on dialysis. 21 This study raises a safety signal for diabetic patients with CAD receiving high KDPI transplants but is not definitive enough to rule out a benefit if total time on dialysis can be reduced through accepting such a transplant.
Patient Education and Pre-consent
All candidates expected to be aged ≥65 at transplant will be offered education about the age-targeted program. The timing of education is at the discretion of the transplant nephrologist, but there is a dedicated information session booked after the patient is cleared as “ready” on the waitlist to discuss the age-targeted program. The decision to enroll is achieved through a shared decision-making process with their transplant nephrologist and informed consent documented.
Multimedia patient information tools were developed to help guide shared decision-making discussions about the age-targeted program. The video, infographics, and frequently asked questions document are available on the Transplant Manitoba web site (https://www.transplantmanitoba.ca/transplant-program/adult-kidney-transplant-program) (https://www.youtube.com/watch?v=PkyHEVamjC4) and (Figures 1 and 2 and Appendix).
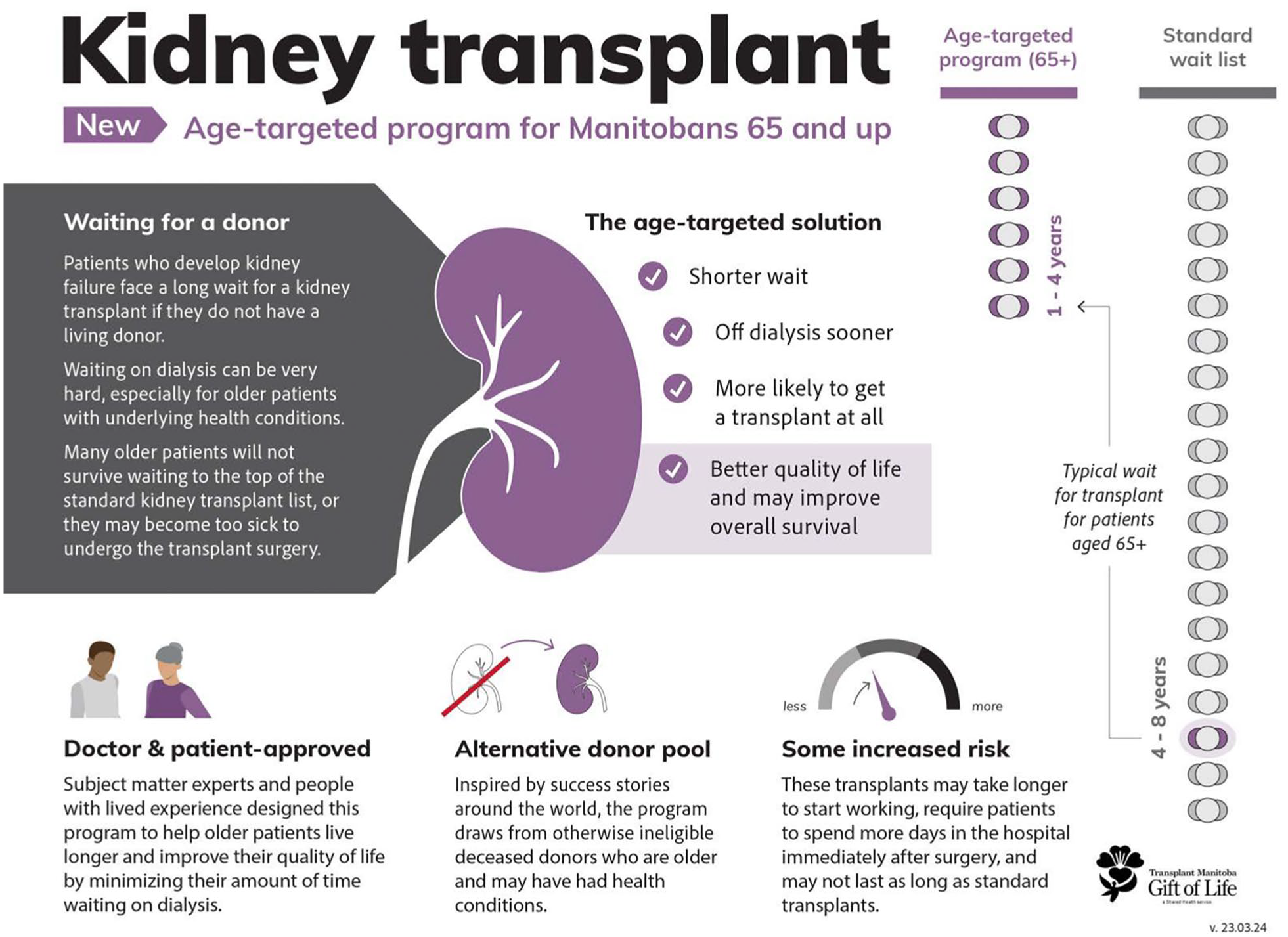
An infographic explaining the new age-targeted kidney transplant program in Manitoba.

A patient decision aid to help eligible transplant candidates understand the risks and benefits of enrolling in the age-targeted program.
Waitlist Management and Organ Allocation
All patients enrolled in the age-targeted program remain eligible for a standard deceased donor transplant as they simultaneously accumulate wait time toward the alternative and standard donor pools. The Transplant Manitoba allocation policy was first developed in 2008, and the criteria are publicly available at https://www.transplantmanitoba.ca/transplant-program/kidney-allocation.
Confirmation of consent/enrollment in the age-targeted program will be obtained annually for patients ready on the list via their transplant coordinator or nephrologist. As a patient approaches the top of the standard deceased donor transplant list, the benefit of a transplant from the alternative donor pool decreases. Once a patient has accumulated 4 years of dialysis time, they should be booked for a pre-transplant clinic visit for a more detailed discussion around the risks and benefits of remaining enrolled in the age-targeted program.
Organ allocation from the alternative donor pool to recipients enrolled in the age-targeted program follows the same scoring system as the standard deceased donor transplant list with wait time calculated from the date of dialysis initiation. A list for all age ≥65 waitlist ready patients is coded as “accept,” “decline,” or “to be determined” for the age-targeted program. Patients who are “to be determined” have been cleared to the wait list and may be waiting for an appointment to discuss the age-targeted program in detail or have had a discussion with their transplant nephrologist and are still deciding whether they want to enroll.
When an alternative KDPI >85 donor becomes available, kidneys are allocated to those who have “accepted” or are “to be determined,” with the rank order determined using the standard scoring system. The transplant nephrologist on call will contact patients allocated an alternative donor pool kidney to discuss the risks/benefits of the offer, with a more detailed discussion for those who are not yet formally enrolled in the program.
Medically urgent and highly sensitized patients
Organs from the alternative donor pool may be allocated to patients who are highly sensitized (panel reactive antibody ≥95%) or listed with medically urgent priority (eg, failing vascular access and not a peritoneal dialysis candidate). The decision to accept the organ offer should be achieved through detailed discussion and shared decision-making between the patient and transplant nephrologist.
Pre-emptive transplant
Pre-emptive transplantation with an alternative donor pool organ will only be considered when there is no suitable recipient ready on dialysis. This is an equity-based decision and is meant to avoid preferential access to transplant for patients with better access to the health care system overall (ie, patients with good primary care, early nephrology care, and the opportunity to get listed for transplant prior to requiring dialysis). To facilitate preemptive allocation, any eligible patient with CKD G4-5ND will have their KFRE calculated every 3 months. Pre-emptive waitlisting for the age-targeted program occurs when the 2-year KFRE is ≥50% on ≥2 occasions.
If there are multiple preemptive age-targeted program candidates, the rank order is determined with the standard scoring system, with the exception that wait time is calculated from the date at which the 2-year KFRE is confirmed to be ≥50%. Patients who have been listed for pre-emptive transplant, but start dialysis prior to transplant will have their wait time recalculated from the date of dialysis initiation and automatically be prioritized above preemptive wait list candidates according to the standard allocation rules.
Allocation to the standard wait list
If there are no suitable pre-consented candidates aged 65 or older to allocate an alternative donor pool kidney through the age-targeted program, the kidneys will be offered through standard allocation to candidates aged 60 and older using the routine allocation priority score and shared decision-making between the transplant nephrologist and potential recipients. If there are no suitable recipients aged 60 and older, the donor kidneys will be offered to other programs outside of Manitoba.
Early graft loss
As the alternative donor kidneys may have a higher risk of PNF or early graft failure, a safety mechanism was built into the allocation system such that if an age-targeted program recipient experiences graft loss within 12 months from transplant, they will have their cumulative wait time—including the time with the graft—reinstated.
Continuous Quality Improvement—Measuring Success
Outcomes
This is a quality improvement project to expand access to deceased donor kidney transplant to improve survival and quality of life for eligible older Manitobans with ESKD. The safety and outcomes of this program will be monitored to inform ongoing updates as needed in plan-do-study-act cycle.
Key performance indicators
1. Program outcomes
a. Primary—Number of additional kidney transplants performed due to the age-targeted program per year.
2. Patient outcomes
a. Primary—Rates of death, PNF, and early graft loss within the first-year post-transplant.
b. Key Secondary—Rate of pre-emptive transplant or time from dialysis to transplant vs age ≥65 years eligible patients not enrolled in the age-targeted program.
c. Secondary—Rate of DGF; length of hospitalization with transplant; estimated glomerular filtration rate (eGFR) at 1, 3 and 5 years; and quality of life measured by EQ-5D-5L, which is routinely collected pre-transplant and post-transplant.
Data collection and analysis
As a clinical quality improvement program, all data are collected as standard-of-care within the Accuro electronic medical record. Data will be extracted from Accuro for the outcomes and safety analysis. Patients will be followed until death-censored graft loss or death with a functioning graft or moved outside of Manitoba.
JMP software version 16.0 (SAS Institute Inc., Cary, North Carolina) will be used for statistical analysis. For categorical data, Fisher’s exact test or Pearson’s chi-square test will be used to determine counts and percentages. Parametric continuous data will be analyzed by Student’s t-tests. Non-parametric continuous data will be summarized as median (interquartile range, IQR) unless stated otherwise and analyzed by the Wilcoxon rank-sum or Kruskal-Wallis rank-sum tests. A 2-tailed P < .05 will be considered statistically significant.
Key Findings
In the interests of transparency and public accountability for a scarce resource, Transplant Manitoba’s provincial allocation rules do not permit bypassing top of the list recipients for routine offers, but instead kidneys must be offered in rank order as allocated by a point system which is predominantly driven by wait time. Transplant providers were previously reluctant to utilize KDPI 86-100 donor kidneys which were allocated to recipients with the longest wait times. This age-targeted program facilitates allocation of KDPI 86-100 kidneys to suitable older pre-consented recipients with low wait times, who are the most likely to achieve a survival and quality of life benefit from these transplants. This approach expands the overall deceased donor pool to benefit all Manitobans awaiting a deceased donor kidney transplant.
Development of this protocol was an iterative process which required multidisciplinary stakeholder engagement with patient partners, transplant and general nephrology providers, transplant surgery, donation physicians, donor coordinators, HLA laboratory, and health care leadership. This information may be useful to other transplant programs seeking to establish a structured approach to the use of high KDPI kidneys.
Limitations
The use of the KDPI to allocate deceased donor transplants has limitations and any discrete cut-off for decision-making is inherently arbitrary, especially in programs outside of the United States where the score was originally validated 8 and undergoes periodic updates. Changes in the donor population of the United States and/or changes in the calculation of the KDPI score determined by The Organ Procurement and Transplantation Network (OPTN) have the potential to impact the distribution of KDPI among our smaller population of donors in Manitoba, thus affecting the number of donors that may be considered for the alternative donor pool. For example, proposed changes by the OPTN to remove race and hepatitis C from the KDPI equation 22 will lead to a change in the characteristics of donors with a KDPI >85. Given that the KDPI is a scaled score, lower KDPI scores for African American and hepatitis C positive donors may increase the proportion of non-African American and hepatitis C negative donors in the KDPI >85 group. In Manitoba, where we have very few African American or hepatitis C positive donors to begin with, application of this new KDPI equation may increase the number of donors in our population who are deemed high KDPI and assigned to the alternative donor pool.
Transplant Manitoba has a single procurement team and a single transplant center for the entire province. This makes implementation of a new program such as this more straight forward than in larger multicenter transplant programs. Obtaining buy-in from providers on the donation and transplantation side, standardizing patient counseling and enrollment, and practicing in a relatively uniform manner are more practical than in larger programs. There may be unintended consequences of the age-targeted program roll-out, eg. despite a process of pre-consent, it is still likely that allocation of alternative donor pool kidneys will be a more lengthy process and involve longer discussions with recipients and potentially more candidate bypasses, extending the overall allocation time. Although the general concepts of this program should be applicable to other transplant centers across Canada, the logistics of implementation will vary according to local practice and system factors.
Finally, the age-targeted program officially launched in January 2023 and outcome data are pending so we cannot comment on the success of the program at this time.
Implications
The overarching objective of this quality improvement project is to improve access to deceased donor kidney transplant for Manitobans with kidney failure. We hope this clinical protocol will be useful to other transplant groups to optimize the use of high KDPI kidneys, such as donor and recipient eligibility criteria, a structured organ allocation approach, and patient educational materials including a video and infographics. Finally, we anticipate this will be a safe and effective way to expand access to kidney transplant from a previously unutilized deceased donor pool.
Footnotes
Appendix – Patient information handout
Acknowledgements
The authors are very grateful for the assistance and input from our patient and provider committees. Developing and implementing this protocol were a significant multidisciplinary team effort, and we are very grateful for the support from all of Transplant Manitoba’s and Manitoba Renal Program staff who contributed.
Ethics Approval and Consent to Participate
The University of Manitoba Health and Research Ethics Board has approved this study [HS25240 (H2021: 388)].
Consent for Publication
Consent for publication was obtained from all authors.
Availability of Data and Materials
The information and patient materials presented in this manuscript are freely available on the Transplant Manitoba Website Adult Kidney Transplant Program | Transplant Manitoba https://www.transplantmanitoba.ca/transplant-program/adult-kidney-transplant-program and ![]() . They are not for commercial use.
. They are not for commercial use.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the George and Faye Yee Centre for Healthcare Innovation Preparing for Research by Engaging Public and Patient Partners (PREPPP) Award (AT), the Dr John M Rh Bowman Memorial Winnipeg Rh Institute Foundation Award (PN), and the Canadian Nephrology Trials Network Financial Assistance Award (AT).