
Abstract
Purpose of program:
Access to exercise and rehabilitation is often lower in rural or remote areas and hemodialysis (HD) dependence imposes additional barriers. Intradialytic cycling (IDC) can improve HD-related symptoms, such as leg cramping, restless legs, and symptoms of depression, as well as physical function and fitness, but access to exercise professionals with this expertise is limited. To promote access to IDC in rural and remote HD units, we describe the implementation and initial evaluation of a novel IDC program using virtual assessment to safely prescribe and individualize IDC.
Sources of information:
We developed and piloted a protocol for virtual IDC assessment and prospectively collected metrics informed by the Reach, Effectiveness, Adoption, Implementation, and Maintenance (RE-AIM) framework to support future quality improvement activities.
Methods:
Rural HD units were defined as per Alberta Kidney Care North (AKC-N)’s operations. The virtual IDC program components were: HD unit education sessions, support and interest from local unit staff and those receiving HD, a bike, a supervising kinesiologist, a stable Internet connection, a nurse present during the 25-minute initial virtual assessment, and virtual follow-up every 3 to 4 weeks with the kinesiologist. The initial assessment consists of a virtual bike test where the participant performs a graded, symptom-limited cycling trial with documentation of vital signs and rating of self-perceived exertion (relative intensity). The data are used to prescribe IDC (frequency, intensity, time). The HD unit staff learn participant and bike set-up, confirm safe exercise parameters for that day, adjust the bike intensity, and take vital signs. Outcomes for evaluating the impact of the IDC program using the RE-AIM health framework were selected.
Key findings:
Out of the 24 HD units in AKC-N, 18 units were defined as either remote or rural (75%). Four of the units (22%) adopted the program, which was less than our target of 30% of units. Individual-level participation (Reach) within those units ranged widely (1-67%) with only one unit reaching the target of at least 30% individual-level participation. Reasons for starting IDC were intradialytic cramping, restless legs, deconditioning, and boredom during HD. Reasons for non-participation were lack of interest and a desire to sleep. Routine exercise program questionnaires on health-related quality of life for program effectiveness were not consistently completed by participants. All virtual assessments were completed as per protocol with a nurse (100% fidelity); however, tests often needed to be re-scheduled due to technical issues with Wi-Fi, limited unit staffing, operational demands, and/or safety concerns. At 1 year, all 4 units continued to participate with 2 additional HD units starting the following year.
Limitations:
Reach could be improved by introducing intradialytic exercise to individuals at HD initiation, prior to moving to their local satellite HD unit. Existing measures of program effectiveness may not be relevant to program participants or feasible to implement without an on-site exercise professional. Technical issues and navigating the busy schedules of unit staff were limitations to completing tests as scheduled.
Implications:
Implementing a protocolized approach with virtual support can increase accessibility to an evidence-based treatment in HD units without exercise professionals. For people requiring HD, reach may be improved with early education and exposure at HD start and with orientation sessions for staff. Adding a virtual IDC assessment day for staff as part of their routine monthly task schedule may promote institutionalization. Formalized follow-up sessions for kinesiologists and nurses to discuss program concerns would benefit the program in the future. Completion of program effectiveness measures may be improved by selecting more individualized options, for example, person-reported measures related to the individual’s reason for referral.
Purpose of the Program
Due to Canada’s vast geography and low population density, access to health services is often limited, contributing to health inequities.1,2 This issue is particularly relevant to the management of chronic kidney disease (CKD) in Canada, where the prevalence of moderate to advanced CKD is higher in rural compared with urban settings.1,3 Rehabilitation services, such as exercise, are considered an essential component of universal health care and play an important role in ensuring well-being and maintaining independence. 4 However, the professionals and programs tailored to provide exercise training for people with multiple chronic conditions are typically co-located within specialty medical centers in urban areas. 5
Kidney failure requiring hemodialysis (HD) is associated with a high symptom burden and decrements in physical functioning and mental health. 6 Exercise, specifically when performed during HD treatment, can improve symptoms such as depression, restless leg syndrome, fatigue, and muscle cramping, as well as physical functioning, strength, and cardiorespiratory fitness.7,8 Intradialytic exercise (IDE) is most commonly implemented as intradialytic cycling (IDC), by placing a stationary bike at the foot of the dialysis chair or bed.
Despite the benefits of IDE, its implementation and maintenance in the setting of the HD unit are complex and require effective communication among nephrologists, exercise specialists (kinesiologists, physiotherapists), nurses, and managers. 9 The barriers and facilitators for HD unit staff (primarily nurses) and people requiring HD are well established.10-12 For unit staff, barriers are consistently related to the lack of time, exercise knowledge and expertise, and concerns regarding safety. People receiving HD have concerns regarding their ability to exercise and adding additional workload for unit staff. Common facilitators of IDE are the support from HD unit staff, specifically, a staff champion, and the expertise of an exercise professional.9,12 In our exercise program, the role of the exercise professional includes medical screening for participation, assessment and prescription of exercise, monitoring, and progression of the exercise program to help participants meet their goals, and education for other members of the health care team. 9 Educating participants on how to self-monitor their exertion, follow the exercise prescription, and recognize when to defer an exercise session optimizes participant safety during IDE.9,13 However, in rural or remote communities, there is often limited access to the expertise required to deliver IDE. 14 The limited exercise expertise among medical professionals, including HD unit staff, is a barrier to initiating such programs among those with multiple health conditions and deconditioning. 10 In this report, we describe the implementation and preliminary evaluation of a novel virtual IDC program aimed at increasing accessibility to IDC in rural and remote HD units in Alberta Kidney Care North (AKC-N).
Sources of Information
We obtained data from the Research Electronic Data Capture System (REDCap 8.8.2© 2018 Vanderbilt University), which is used to store data on exercise program metrics that is participants by clinic/unit and results of physical function testing and questionnaires from their assessments. These data are entered by the clinical kinesiologists. We obtained information regarding our virtual bike program and identified evaluative outcomes within the Reach, Effectiveness, Adoption, Implementation, and Maintenance (RE-AIM) framework from stakeholders (kinesiologists, nurses, managers, and nephrologists). 15
Methods
Setting and Exercise Program Structure
Alberta Kidney Care North catchment area encompasses a large geographic area over which care is delivered to 2500 people with non–dialysis-dependent kidney disease, 1200 people with HD-dependent kidney failure, and approximately 400 people receiving home dialysis. Kinesiologists have been a part of the multidisciplinary CKD team since 2015 in AKC-N. Kinesiologists are clinical exercise physiologists, who have completed a Bachelor of Kinesiology degree with an additional certification in clinical exercise for chronic disease management. Over the last 9 years, the kinesiology team has increased its capacity from 1.0 to 3.8 full-time equivalent (FTE) and expanded its services to provide exercise counseling to people across all stages of CKD. The resources offered include virtual group exercise classes, home exercise programs, and IDE. For those receiving in-center HD, IDE can include resistance exercise (bands, dumbbells, or ankle weights), cycling (IDC), or a combination of both. The role of the kinesiologists in IDE is to conduct a health history and physical assessment, to prescribe, monitor, and progress exercise, and to re-assess the participant’s progress. However, due to the lack of travel funding and feasibility, IDE was primarily only available in 6 HD units in Edmonton, Alberta. Operationally, any sites outside of Edmonton and Red Deer are defined as rural. As Red Deer is >150 km distance by road from Edmonton, this was defined as remote. The HD unit staff (registered nurse [RN] and licensed practical nurse) to patient ratio in our program is typically 1:3. Uniformly, these rural and remote sites did not have on-site professional support for exercise during HD (kinesiologists or physiotherapists). As per our program’s best practices, all potential IDE participants must undergo an assessment with the kinesiologist prior to starting IDE. Potential participants are screened for any of the following contraindications: cardiac event within the past 6 months, severe aortic stenosis, pericarditis, myocarditis, unstable angina, third-degree atrioventricular block, unstable angina, uncontrolled diabetes and/or chronic obstructive pulmonary disease, hemodynamic instability, or severe bone disease with multiple fractures. Hemodialysis unit staff assist with equipment set-up, encourage and document participation, and liaise with the kinesiologist.
Virtual IDC Program
The purpose of the virtual IDC program was to increase accessibility to IDC for remote and rural-dwelling HD-dependent individuals. We aimed to follow the same standards with respect to safety and effectiveness (improving physical function, ameliorating HD-related symptoms) while fostering interest and capability among participants, HD unit staff, and managers to support IDC without an on-site kinesiologist. We therefore developed a protocol for the virtual assessment of people receiving HD, including a virtual bike test (VBT), to assess hemodynamic stability with IDC and to inform the participant’s exercise prescription.
The virtual IDC program processes were developed with stakeholders (HD unit staff, managers, nephrologist, and people receiving HD). Consistent with the known barrier of time, in our early engagement with HD unit staff at rural sites the importance of streamlining the process and minimizing disruption to the HD session and other scheduled tasks was emphasized. With feedback from HD unit managers, we developed a high-level overview for HD unit staff and managers on what the virtual bike program would entail (Figure 1) and more detailed description of the role of the HD unit staff (Figure 2). On days where program-wide activities were already scheduled (ie, monthly blood work, physician rounding, foot checks), we avoided for virtual testing. The exercise program manager formulated a business proposal for Information Technology Services to request authorization for the procurement of iPads to rural units to facilitate the initiation of this program. Managers of AKC-N rural HD units were subsequently notified about the IDC program via operational meetings and e-mails. We then followed up with the larger rural units and engaged with the unit managers to determine if unit staffing was stable and if they were interested in hearing about the program. Interested units contacted the kinesiology team to schedule the virtual education session explaining IDC benefits, as well as unit and individual eligibility. This was a 20-minute Zoom presentation given by an AKC-N kinesiologist with 20 minutes for questions. Unit eligibility is based on addressing key individual- and setting-level determinants of successful IDE implementation: having an exercise champion in the local HD unit, space for bike storage, and individual interest.11,16 Alberta Kidney Care North provides funding for bikes (Monark 881E cycle [Healthcare International, Langley, Washington] or the TherapyTrainer [Interactive Motivation, Greeley, Colorado]). Unit staff are asked to promote the IDC program within the unit and recruit potential participants. Prior to conducting the initial virtual assessment, the kinesiologist uses the electronic medical record (EMR) and phones the potential participant to review their medical history, obtain consent, and delineate the potential participant’s goals and motivation for exercising. Contraindications to IDE are consistent with the American College of Sports Medicine Guidelines for Exercise Testing and Prescription with the addition of the following program criteria specific to IDE: pre-dialysis blood pressure greater than 90/40 mmHg and less than 180/100 mmHg, blood glucose 5.5 to 16.7 mmol/L, and ultrafiltration rate ≤15 mL/h/kg. 17 If no contraindications are identified, the kinesiologist explains the virtual assessment and arranges the initial virtual assessment with the HD unit.

An overview of the virtual IDC program initiation in remote and rural hemodialysis units.

Components and processes for remote and rural HD units wanting to participate in the IDC program.
Initial Virtual Assessment and VBT
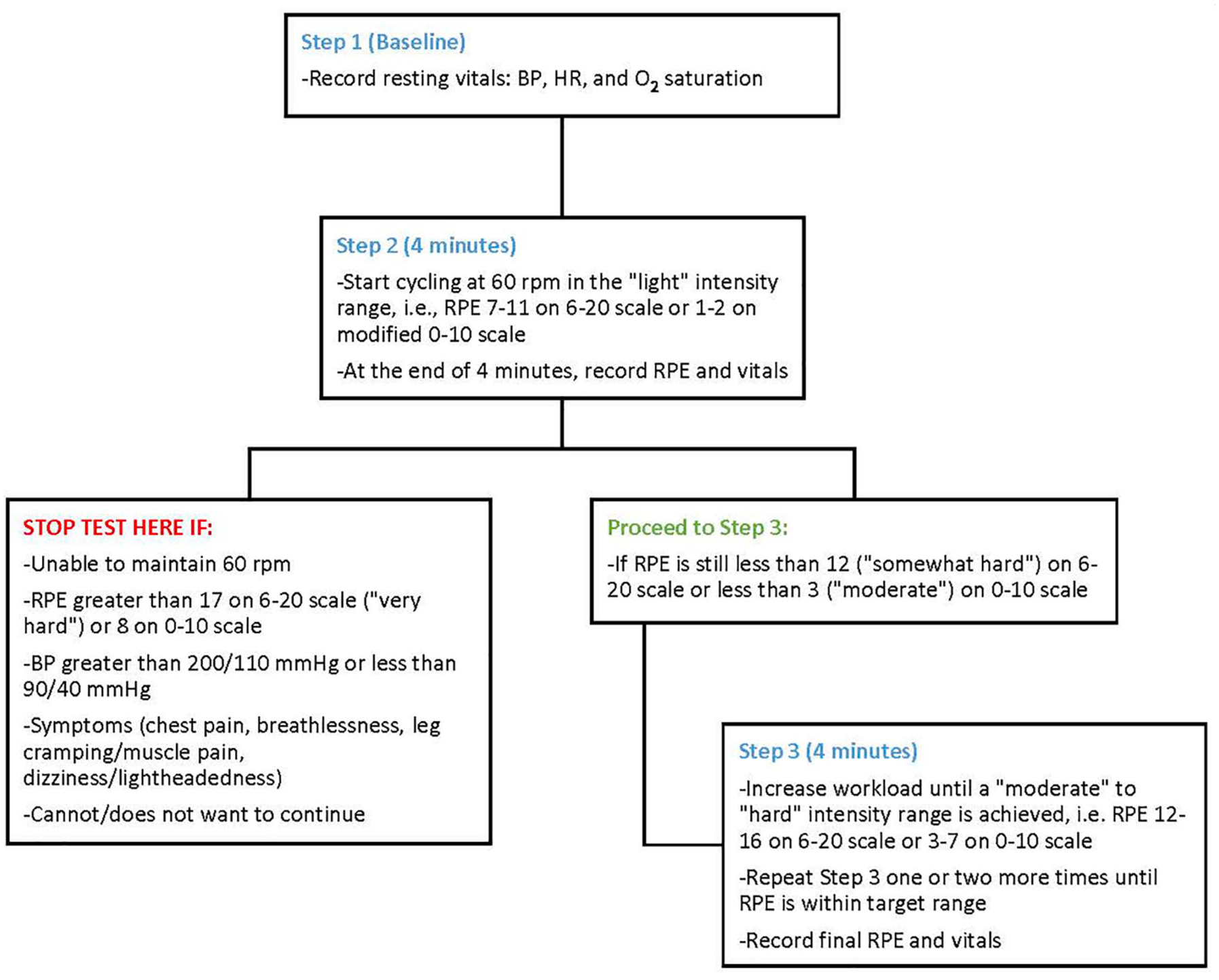
Following equipment set-up (Figure 2), the participant’s blood pressure, blood glucose, and programmed ultrafiltration rate are obtained by the unit nurse at the start of the assessment with the kinesiologist prior to proceeding. If within the specified parameters, the VBT is initiated (Box 1). The VBT is a modification of a submaximal exercise for IDC. 18 The nurse is present at the bedside to monitor the participant and check vitals throughout the assessment. At the completion of the VBT, the results are discussed. For example, if the participant completes two 4-minute stages and reaches a rate of perceived exertion (RPE) of 12 at the end of the second stage, that is, “somewhat hard” exertion level on the 6 to 20 scale, the prescribed workload would target this RPE cycling continuously for 15 to 20 minutes (as tolerated) in a session. 19 The initial VBT assessment is approximately 25 minutes in length.

The VBT. The VBT is completed during the initial virtual assessment to determine the initial IDC prescription and to confirm hemodynamic stability during IDC.
Follow-up
Program participants are contacted virtually as per their preference via phone, e-mail, or Zoom every 3 weeks to assess adherence and motivation, and to determine if the IDC prescription needs to be progressed. Intradialytic vital signs and dialysis prescription parameters are routinely uploaded directly to the EMR. The kinesiologist reviews the EMR remotely for blood pressure and ultrafiltration rate parameters, recent hospitalizations, and documented adherence in the EMR. The kinesiologist will also discuss the participant with the unit staff on an ad hoc basis.
Evaluative Framework
We used the RE-AIM model to inform future quality improvement initiatives for the rural IDC program. 15 Reach was defined as the absolute number and proportion of HD-dependent individuals within the unit who completed the initial assessment with VBT (individual level). Based on our Edmonton-based HD units, approximately 30% of people dialyzing in the unit will participate in an initial kinesiologist assessment and this was used as a benchmark to assess Reach. Physical function testing (eg, 6-minute walk test, timed-up and go) and a health-related quality of life (HRQoL) questionnaire are our program’s routine measures of effectiveness at baseline and every 6 months; however, due to the lack of availability of personnel to collect these locally, we used HRQoL questionnaire data only. Adoption was defined as the proportion of rural units that had participants complete the initial assessment with VBT (unit level). We aimed to have the virtual IDE program adopted by 30% of rural or remote HD units. Implementation was measured as the proportion of initial assessments completed as per protocol with the nurse present. We specified that an RN should be present for all assessments. Maintenance was defined as the proportion of HD units still doing IDC 1 year after its introduction.
Key Findings
The virtual IDC program started in March of 2021. Individual-level data on Reach is shown in Table 1. Reasons for starting IDC among participants were intradialytic cramping, restless legs, deconditioning, and boredom during HD. Reasons for non-participation among participant units were lack of interest and wanting to sleep during HD. Questionnaire data on HRQoL was incomplete at baseline. Four of the 18 rural or remote units (22%) adopted the program (Figure 3). These units represented both the smallest and the largest rural units in our program as well as the most proximal and higher distances from the main site in Edmonton. All assessments were completed as per protocol with nurses; however, common reasons for having to re-schedule planned testing were technical issues with the tablet, limited staff or staff being too busy, and participants being unwell or not attending HD. At 1 year, all 4 units continued to participate with a total of N = 21 participants and 2 units starting in the last year (N = 7). There were no adverse events (intradialytic hypotension, chest pain, loss of consciousness) during IDC and no sessions were stopped prematurely.
Reach: Proportion of Individuals Within Alberta Kidney Care North’s Rural and Remote Units That Participated in an Initial Intradialytic Cycling Program Assessment With a VBT.

Note. HD = hemodialysis; VBT = virtual bike test.
Map of Alberta with the location of hemodialysis units participating in the virtual cycling program and distance from the main site in Edmonton.
Limitations
Several factors may have limited the adoption and reach of the virtual IDC program. For example, participation entailed support and interest from staff and people receiving HD, and it is unclear which may have been the limiting factor. In our experience from implementing IDC in urban centers, staff engagement is enhanced through hearing about the benefits directly from the people dialyzing in their unit (eg, fewer cramps during dialysis, greater strength), rather than education sessions on the same topics; however, this opportunity was not available with the virtual program. 16 In addition, at the smaller sites, factors that are challenging to modify, such as limited space for bike storage, may have precluded adoption. Measures of program effectiveness were also limited by the lack of accessibility to personnel to do physical function testing before starting IDC and at follow-up and questionnaires were not completed. A process for providing feedback on the IDC program between the kinesiology team and the unit staff on a regularly scheduled basis could promote program maintenance.
Implications
Our aim was to improve accessibility to IDC by providing HD-dependent individuals access to specialty services through virtual assessment and follow-up. In AKC-N, the process for individuals to participate in any type of IDE entails medical screening by a certified clinical kinesiologist and monitoring of the hemodynamic response to exercise during HD. Using this approach, we can develop an individualized exercise prescription that is both safe and effective. Consistent with our experience and supported by the literature, HD unit staff commonly report that they do not believe they have the necessary skills and training to oversee and maintain IDE and tend to consider only younger and more functionally independent individuals as candidates.11,16 Despite this rationale for exercise professional supervision, we recognized this was a limitation to adoption of IDE at sites without on-site expertise and developed this protocol that can be used to safely tailor the IDC prescription to the participant’s abilities.
To improve the reach of our IDE program, we have added an in-person meeting with a kinesiologist and teaching on its benefits during the participants’ initial HD sessions at several of our Edmonton sites. Early exposure to IDE and seeing other people cycle on HD may increase self-efficacy and promote participation when they move to their local HD unit. Unit adoption was not related to unit size or proximity to the main center. Consistent with literature on exercise barriers and facilitators to IDE, adoption was likely influenced by the presence of an exercise champion among the HD staff, which may also be influenced by personal perspectives on the importance of exercise.11,16 We have found that targeted educational “blitzes” incorporating individual stories relaying the positive impact of exercise as well as physical activity initiatives for staff improved adoption among units in Edmonton and have successfully used this approach in rural units. To improve implementation, e-mailing the Zoom link for the initial virtual assessment to all unit staff, rather than just the exercise champion, helped improve scheduling. A designated, scheduled “VBT” day per month for the unit, similar to that of other unit staff tasks, could further promote institutionalization of IDC and prioritize its scheduling. Using measures of program effectiveness that are more directly related to the participants’ indication for referral (eg, severity of cramping/restless legs) may lead to higher completion rates than a generic HRQoL questionnaire. Ongoing follow-up is also required for program maintenance and individual-level adherence. We found that the participant and the unit staff need regular communication to promote maintenance at both the unit level and the individual level.
In conclusion, a protocolized approach with virtual support can increase accessibility to an evidence-based treatment and ensure that exercise is prescribed safely and effectively. Effective communication and collaboration among all stakeholders are crucial for maximizing the benefits participants can derive from such virtual programs. Continuous feedback and monitoring of both person-level outcomes and program efficacy are essential for enhancing the quality of current virtual exercise programs.
Footnotes
Acknowledgements
The authors thank the participants, staff members, and administration in Alberta Kidney Care North for their support.
Ethics Approval and Consent to Participate
Not applicable.
Consent for Publication
All authors consent to the publication of this study.
Availability of Data and Materials
Materials for this report are available on request from the corresponding author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.