
Abstract
Rationale:
Pyoderma gangrenosum is a rare neutrophilic dermatosis. Misdiagnosis of pyoderma gangrenosum as an infection is not uncommon. Pyoderma gangrenosum can be associated with Koebner phenomenon and rarely results in systemic inflammatory response syndrome and shock.
Presenting concerns of the patient:
A 61-year-old woman had recently started maintenance hemodialysis, using a tunneled catheter. She was admitted with fever and signs of inflammation at the catheter exit site and along the tunnel.
Diagnoses:
The initial diagnosis was catheter-related tunnel infection. The exit site broke down into a 5 cm × 5 cm lesion typical of pyoderma, and a new similar lesion developed at a subcutaneous injection site in her abdomen. Clinical diagnosis of pyoderma gangrenosum was made. She remained febrile despite broad antibiotic coverage and catheter removal and developed systemic inflammatory response syndrome (SIRS) that necessitated transfer to intensive care unit.
Interventions:
She responded well to fluids and intravenous steroids. Viral and bacterial cultures were negative throughout; echocardiography and computed tomography were unrevealing. Insertion of a new hemodialysis catheter was deferred as long as clinically possible, was undertaken while the patient was taking steroids, and was uncomplicated.
Outcomes:
She remained hemodynamically stable and was discharged after rehabilitation. Her wounds slowly granulated and healed. Steroids were tapered.
Teaching points:
To our knowledge, this is the first case report of a patient with pyoderma gangrenosum developing at the site of tunneled hemodialysis catheter. Our patient developed SIRS with no evidence of infection. We summarize 11 previous case reports of pyoderma leading to SIRS and responsive to steroids.
Introduction
Pyoderma gangrenosum is a rare neutrophilic dermatosis, first described in 1916. 1 Pyoderma can be idiopathic or, more commonly, associated with other systemic diseases such as arthritis, inflammatory bowel disease, monoclonal gammopathy, and malignancies. 2 In its classic form, it is characterized by painful nodules and pustules that rapidly expand and ulcerate. Variants are pustular, bullous, vegetative, and peristomal. 3 Skin biopsies are characterized by dermolysis, sterile neutrophilic infiltrate and lymphocytic perivascular, and mural infiltrates. 2
The pathogenesis of pyoderma involves variable defects in neutrophilic functions and inflammatory mediators in genetically predisposed persons. 4 It more commonly affects women and has a predilection to involve the lower limbs; the incidence is 5 to 6 patients per million population per year.5,6 The diagnosis is challenging, but mostly clinical, supported by histopathology and exclusion of alternative etiologies. Pyoderma is commonly misdiagnosed and unrecognized.7,8
We report a patient who developed pyoderma at the site of tunneled dialysis catheter insertion, who subsequently developed systemic inflammatory response syndrome (SIRS) and evidence of end-organ dysfunction. To our knowledge, this is the first description of pyoderma at the site of a tunneled dialysis catheter.
Presenting Concerns
A 61-year-old African-Canadian woman was admitted to the hospital with fever, dyspnea, and a diagnosis of pneumonia. Medical history included chronic kidney disease, previous pyoderma gangrenosum resulting in left above-knee amputation, diabetes mellitus, hypertension, osteoarthritis, and sarcoidosis. Her kidney function deteriorated, a permanent hemodialysis catheter was inserted, and hemodialysis started. She was discharged, with the expectation that dialysis would be long-term.
One week later, she presented with diarrhea and vomiting.
Clinical Findings
Her blood pressure (BP) was 157/79 mm Hg, heart rate 97 beats per minute, respiratory rate 20 breaths per minute, and temperature 38.3°C, with oxygen saturation of 98% on room air. Purulent discharge and redness were noticed around the catheter exit site, and there was induration, redness, and tenderness along the tunnel. Apart from the above-knee amputation, the rest of the examination was unremarkable.
The patient was admitted with a diagnosis of dialysis catheter tunnel infection. Central and peripheral blood samples and a swab from purulent discharge around catheter exit site were sent for cultures; she received intravenous cloxacillin 2 g every 6 hours, and vancomycin 15 mg/kg bolus and subsequent doses, targeting 15 to 20 mg/L trough levels. The catheter was promptly removed and its tip sent for culture. Transthoracic echocardiogram did not show valvular vegetations.
During the first week of hospitalization, the patient continued to have high-grade fever and leukocytosis (Figure 1). The swelling at the catheter tunnel exit site expanded and ulcerated with multiple points of purulent discharge over an area of 5 cm × 5 cm (Figure 2A). At the clavicle, a small collection was lanced and 1 to 2 mL of pus was expressed. A new painful nodular lesion developed on the abdominal wall at the site of subcutaneous low-molecular-weight heparin injections, which later ulcerated (Figure 2B). Blood cultures were repeated multiple times and were negative, as were the catheter tip, swab from the exit site, pus from the clavicular collection, and swabs from the abdominal ulcer. Stool enteric cultures, clostridium difficile toxin, and urine culture were also negative. We requested surgical review for consideration of incision and drainage, but all the lesions were deemed too small. The antibiotic coverage was broadened on the third day of hospitalization to intravenous piperacillin/tazobactam 2.25 g every 8 hours; vancomycin was continued.

Top panel, highest daily temperature by day of admission; bottom panel, leukocyte count, × 109/L.
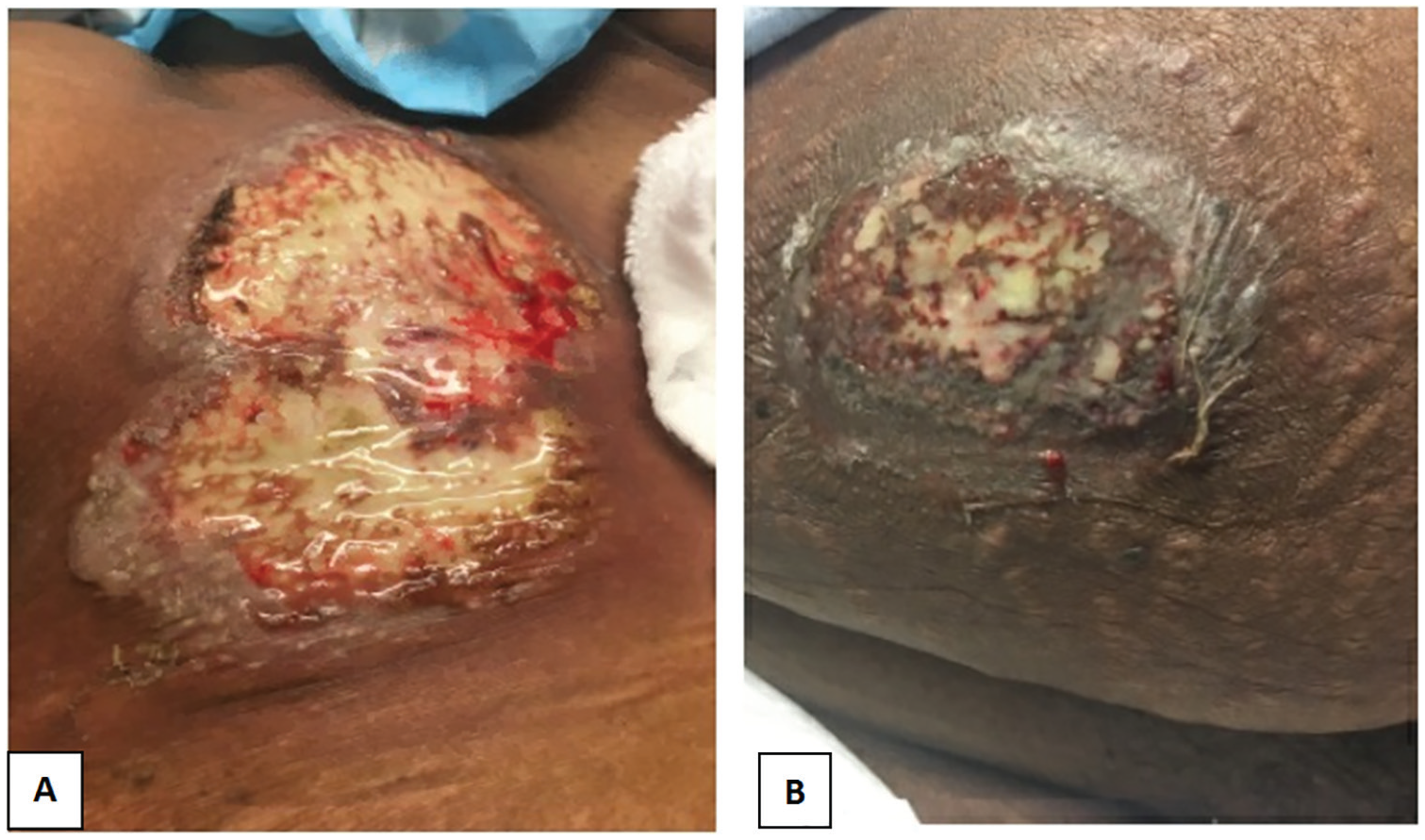
(A) Chest wall lesion at the tunneled catheter exit site on day 7 of admission; (B) abdominal wall lesion at the site of low-molecular-weight heparin injection on day 7 of admission.
Diagnostic Focus and Assessment
Given the development of classic-appearing lesions at 2 sites, and a prior history of pyoderma and sarcoidosis, a clinical diagnosis of pyoderma gangrenosum was entertained on the seventh day of hospitalization. After consultation with rheumatology, the decision was made to avoid biopsy to prevent precipitating further lesions. In addition, the insertion of a new dialysis line was deferred. The patient’s diuretics were maximized, and she was stable without dialysis for 11 days. Initiation of steroids for pyoderma was delayed because of concerns that ongoing fever and leukocytosis represented infection. She was not taking maintenance steroids for sarcoid.
On the eighth day, the patient developed hemodynamic instability, BP of 94/39 mm Hg, and acute alteration of mental status. Laboratory investigation showed C-reactive protein of 335 mg/L, leukocyte count of 28.7 × 109/L, and normal serum lactate. She was resuscitated with intravenous fluids and transferred to the intensive care unit. Computed tomography of the chest, abdomen, and pelvis with the administration of intravenous contrast revealed left lower lobe consolidation, in keeping with her prior admission with left lower lobe pneumonia, and mediastinal lymphadenopathy, in keeping with her known sarcoidosis, but no other pathology.
Therapeutic Focus and Assessment
Following transfer to the intensive care unit, the patient was treated with intravenous hydrocortisone 50 mg every 6 hours, and antibiotics were continued unchanged. She did not require hemodynamic or ventilatory support. Within 2 days of steroid initiation, fever resolved, and the pain at the site of the lesions markedly improved. A new tunneled dialysis line was then inserted, and hemodialysis was resumed. Intravenous hydrocortisone was changed to oral prednisone 50 mg/day, and piperacillin/tazobactam was stopped. Intravenous vancomycin was continued for a total of 4 weeks.
Follow-up and Outcomes
The patient was discharged after 4 weeks of hospitalization. Discharge medications included oral prednisone 50 mg daily and hydroxychloroquine 200 mg twice a day. Skin ulceration continued to improve, and 2 months after the initial hospitalization, the ulcers were almost completely healed (Figure 3A, B).

(A) Chest wall lesion at the tunneled catheter exit site after 2 months; (B) abdominal wall lesion at the site of low-molecular-weight heparin injection after 2 months.
Patient Perspective
The patient reported, I came with pneumonia. Blood tests showed my kidneys are shutting down. They put line in for dialysis, and I was in the hospital for a week. I went home and come back on Monday for my dialysis. Between Saturdays to Monday, it seems to got infected. I had to go through an emergency. When I ended up in ICU, my fever was 104°F, and I passed out. I did not know what happened after that. I stayed in the hospital for a month, lots of high temperatures, diarrhea, and antibiotics. I am still shaky with my current prednisone dose. I know it has cut down to 40, and I hope it will come down further. I had previous bad experience with pyoderma.
Discussion
Pyoderma is associated with increasing age,9,10 with inflammatory bowel disease, inflammatory arthritis, solid organ malignancies, hematologic malignancies, and other hematologic disorders, but not to our knowledge with sarcoid. 10 An association with diabetes, with metabolic syndrome, and with elevated creatinine levels has also been reported. 11 It is twice as common in women as in men; the prevalence is similar in white and African American patients. 9
Our patient was admitted with what appeared to be tunneled dialysis catheter infection. She was treated with antibiotics and prompt catheter removal. Her course was recognized to be atypical from the third hospital day, but despite the patient’s history of pyoderma severe enough to necessitate amputation, it was not until a new lesion developed in an injection site that a diagnosis of pyoderma was considered. From her perspective, it was one problem after another: pneumonia that precipitated a need for dialysis, pus at her exit site, multiple skin lesions that were puzzling her doctors, becoming critically ill, and finally suffering adverse effects from the moderate doses of steroids used in her treatment.
Pyoderma is known to develop sometimes at the site of skin trauma, namely, the Koebner phenomenon 12 or pathergy 13 ; pyoderma at surgical sites14,15 and with instrumentation16,17 has been reported. To our knowledge, this is the first case reported of pyoderma developed at the site of dialysis tunneled catheter (search strategy, Supplementary Table 1). However, pyoderma at a venous access device 18 and at a peritoneal dialysis catheter exit site has been previously reported. 19
To learn what was known about whether pyoderma can cause systemic inflammatory response syndrome and hypotension, we also conducted a formal literature search of this question (Appendix). Presumably, the pathogenesis of SIRS is mediated by inflammation and cytokines as in sepsis caused by bacterial organisms, but we did not find any data directly on this issue.
We identified 11 case reports of 11 patients (Table 1). Common initial diagnoses were necrotizing fasciitis and surgical site infection. Three patients had underlying diseases commonly associated with pyoderma. Deterioration of their clinical condition despite broad-spectrum antibiotics, sterile cultures, and histologic findings compatible with pyoderma prompted the correct diagnosis. All patients had a favorable outcome and rapidly improved after systemic steroids were started. The improvement of our patient’s clinical condition with steroids but without change in antibiotics suggests that severe pyoderma was the cause of her hypotension. We did not find any information on whether the patient’s chronic kidney disease may have contributed to the development of a sepsis syndrome; none of the other case reports mentioned advanced chronic kidney disease.
Summary of Previous Reports of Pyoderma Gangrenosum and Shock or Severe Sepsis-Like Clinical Presentation.

A limitation of our study is that no skin biopsy was done. We chose not to perform it because the diagnostic yield is low 31 due to the typical appearance of the lesions, her known history of pyoderma, and the risk of worsening of the lesions. We acknowledge that our patient did not meet criteria for the diagnosis of pyoderma, according to the consensus diagnostic criteria, which are histology plus 4 minor criteria. 13 Of the minor criteria, 6 out of 8 were met: exclusion of infection, pathergy, a papule that rapidly ulcerated, peripheral erythema and an undermining border with tenderness, multiple ulcerations, and response to immunosuppression. (Criteria not met were: inflammatory bowel disease or inflammatory arthritis and wrinkled paper appearance at healed lesions.) Our patient had a history of previous amputation for pyoderma, perhaps signifying an inherent susceptibility to more severe outcomes. We acknowledge that more details of her prior history of pyoderma and of sarcoid would have been interesting and would have enhanced this report. The literature does not permit us to predict whether she is likely to have further episodes in future. The risks and benefits of future interventions for access or other future procedures should include the possibility of future reactivation of pyoderma in surgical sites. Successful kidney transplantation, without ulceration at the surgical site, has been described in a patient with severe pyoderma and a history of developing intractable ulcers at surgical sites; probably, the immunosuppression necessary for the transplant reduced the risk of pyoderma in this case. 32
Conclusions
We report the first case of pyoderma gangrenosum as a complication of a tunneled dialysis catheter and summarize the previous reports of patients with SIRS that was eventually attributed to pyoderma. Clinicians should consider pyoderma in the evaluation of sterile abscesses or abscesses not responding to appropriate antibiotics, particularly at surgical sites and exit sites, and consider skin biopsy for definitive diagnosis.
Supplemental Material
sj-docx-1-cjk-10.1177_20543581221120618 – Supplemental material for Pyoderma Gangrenosum After Insertion of a Hemodialysis Catheter: Koebner Phenomenon, Systemic Inflammatory Response Syndrome, and a Delay in Diagnosis
Supplemental material, sj-docx-1-cjk-10.1177_20543581221120618 for Pyoderma Gangrenosum After Insertion of a Hemodialysis Catheter: Koebner Phenomenon, Systemic Inflammatory Response Syndrome, and a Delay in Diagnosis by Majed M. Alosaimi, Fatemah Sebzali, Ali Iqbal, Christian G. Rabbat and Catherine M. Clase in Canadian Journal of Kidney Health and Disease
Footnotes
Appendix
Search strategy: we searched MEDLINE and Embase databases from inception to February 29, 2020 (search strategy, Supplementary Table 2). We reviewed the reference lists of relevant articles and conducted “fuzzy” searches in Google Scholar. We refined the formal search strategy to include terms that identified articles that we had found using other methods. We identified 367 articles and screened titles and abstracts in duplicate (M.M.A. and F.S.). Eligibility criteria were a report of one or more adult patients with a final diagnosis of pyoderma, who also had either admission to the intensive care unit or shock, or severe sepsis, without evidence of infection. We accepted the original report’s definition of severe sepsis and septic shock, provided it was aligned with the American College of Chest Physicians-Society of Critical Care Medicine consensus definition. 33 We included studies in all languages, translating using translators or, where a translator could not be found, Google translate. Cohen’s kappa between the 2 reviewers was 0.73 (95% confidence interval, 0.56-0.90), with disagreements resolved by a third author.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Alosaimi, Sebzali, Iqbal, Rabbat: none. Catherine Clase has received consultation, advisory board membership, or research funding from the Ontario Ministry of Health, Sanofi, Pfizer, Leo Pharma, Astellas, Janssen, Amgen, Boehringer-Ingelheim, and Baxter. In 2018, she co-chaired a KDIGO potassium controversies conference sponsored at arm’s length by Fresenius Medical Care, AstraZenec, Vifor Fresenius Medical Care, Relypsa, Bayer HealthCare, and Boehringer-Ingelheim. She serves as Editor-in-Chief for Canadian Journal of Kidney Health Diseases.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval and Consent to Participate
The patient gave written consent, including the publication of anonymized photographs.
Consent for Publication
The patient gave informed consent for anonymized publication of her experience.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.