
Abstract
Background:
Depression and anxiety affect approximately 50% of patients with kidney failure receiving hemodialysis and are associated with decreased quality of life and increased risk of hospitalization and mortality. A Brief Mindfulness Intervention (BMI) may be promising in treating depressive and anxiety symptoms in this population, but the long-term sustainability of the intervention’s effects is unknown.
Objective:
We previously conducted a randomized controlled trial (RCT; n = 55) comparing an 8-week BMI with an active control (Health Enhancement Program [HEP]) for patients receiving dialysis, with depression and/or anxiety. Here, we examine the 6-month follow-up data to determine the long-term sustainability of BMI versus HEP in reducing (1) depressive symptoms, (2) anxiety symptoms, and (3) the efficacy of BMI versus HEP in reducing the likelihood of hospitalization.
Design:
In this study, we analyzed 6-month follow-up data from an 8-week assessor-blinded parallel RCT, which evaluated the efficacy of a BMI against an active control, HEP, in patients receiving hemodialysis with symptoms of depression and/or anxiety.
Setting:
The study took place at hemodialysis centers in 4 tertiary-care hospitals in Montreal, Canada.
Participants:
Participants included adults aged ≥18 years who were receiving in-center hemodialysis 3 times per week and had symptoms of depression and/or anxiety as indicated by a score ≥6 on the Patient Health Questionnaire–9 (PHQ-9) and/or the General Anxiety Disorder–7 (GAD-7).
Methods:
Participants were randomized to the treatment arm (BMI) or the active control arm (HEP) and completed assessments at baseline, 8 weeks, and 6-month follow-up. Depression was assessed using the PHQ-9, and anxiety was assessed by the GAD-7. Hospitalization rates were assessed using medical chart information.
Results:
We observed significant decrease in depression scores over 6 months in both BMI and HEP groups, with no significant difference between groups. Anxiety scores significantly decreased over 6 months, but only in the BMI group. Brief Mindfulness Intervention and Health Enhancement Program were comparable in terms of hospitalization rates.
Limitations:
The limitations of our study include the modest sample size and lack of a third arm such as a waitlist control.
Conclusions:
Our results suggest that the beneficial effects of BMI and HEP for improving mood disorder symptoms in patients receiving dialysis persist at 6-month follow-up. Both interventions showed sustained effects for depressive symptoms, but BMI may be more useful in this population given its efficacy in reducing anxiety symptoms as well.
Trial registration:
Prior to recruitment, the trial had been registered (ClinicalTrials.gov Identifier: NCT03406845).
Introduction
Globally, there are over 2.5 million patients with kidney failure, and this number is estimated to increase to 5.4 million by 2030. 1 The most prevalent psychiatric symptoms in this population are depression and anxiety, which affect up to 50% of patients receiving hemodialysis. 2 Depression and anxiety are associated with decreased quality of life, increased dialysis non-adherence, suicidal behavior, and increased mortality.3,4 Furthermore, both anxiety and depressive symptoms are significantly associated with increased likelihood and length of hospitalizations in this population. 5 Despite their negative effects on patients receiving dialysis, depression and anxiety symptoms are rarely assessed, and the majority of this population are not receiving effective treatment. 4 Antidepressants are prescribed with reluctance, due to inadequate data on their effectiveness 6 and safety 7 in this population, in addition to safety concerns regarding possible drug-drug interactions due to polypharmacy and increased risk of toxicity due to reduced renal clearance. 4
Mindfulness-based interventions (MBIs), which teach the cultivation of non-judgmental present-centered awareness, have shown effectiveness in treating numerous psychiatric conditions, including depression and anxiety, as well as chronic physical problems. 4 However, there is a lack of research assessing the effectiveness of MBIs for depression and anxiety in patients undergoing dialysis. Therefore, we conducted an 8-week multicenter randomized controlled trial (RCT) comparing a Brief Mindfulness Intervention (BMI) with an active control (Health Enhancement Program [HEP]) in 55 patients receiving dialysis who had symptoms of depression and/or anxiety (BMI = 25, HEP = 30). 4 We previously reported the primary endpoint data, demonstrating that both BMI and HEP were associated with significant reductions in depressive symptoms at 8 weeks. 4 Furthermore, BMI showed significant reductions in symptoms of anxiety (while HEP did not). 4 The results suggested that for patients receiving dialysis, BMI and HEP may be helpful interventions for depressive symptoms, while BMI was superior to HEP in decreasing anxiety symptoms. 4 Here, we report 6-month follow-up data to assess the sustainability of these effects.
Although our primary endpoint data showed that BMI may be helpful in reducing depression and anxiety by the end of the intervention, it is important to note that depression and anxiety, which increase patients’ risk of hospitalization and mortality, are marked by high relapse rates. 8 Mindfulness-Based Therapies (MBTs) show promise for sustainability of reduction in depression and anxiety in the long term. Several applications of MBTs have been designed to prevent relapse in psychiatric diagnoses such as depression and have demonstrated efficacy in sustaining positive effects on mental health outcomes in the long term.9,10 For example, a large meta-analysis examining 209 MBT trials showed large and clinically significant effects in treating depression and anxiety, and these gains were maintained at long-term follow-up (mean follow-up = 28.92 weeks). 11
To our knowledge, there is no literature on the long-term efficacy of BMIs for anxiety and depressive symptoms in patients undergoing dialysis. Such long-term efficacy data are needed because depression and anxiety are the most common psychiatric diagnoses in this population, have high relapse rates, and are significantly associated with increased risk of hospitalization. The primary aim of this article is to compare the efficacy of BMI and HEP in reducing depressive and anxiety symptoms in patients receiving dialysis using the follow-up data from our previously reported clinical trial. Furthermore, we aimed to examine whether BMI was associated with reduced risk of hospitalization from baseline to 6-month follow-up, compared with HEP. Specifically, we hypothesized that BMI would be more effective than HEP over 6-month follow-up for reducing (1) symptoms of depression, (2) symptoms of anxiety, and (3) the likelihood of hospitalization.
Methods
Study Design
In this study, we analyzed 6-month follow-up data from an 8-week assessor-blinded parallel RCT, which evaluated the efficacy of a BMI against an active control, HEP, in patients receiving hemodialysis with symptoms of depression and/or anxiety. For more exhaustive details concerning the design and methodology of this RCT, please refer to our previous report. 4
Ethical Considerations
Prior to recruitment, the trial had been registered (ClinicalTrials.gov Identifier: NCT03406845). The study was approved by the Research Ethics Boards at all participating hospitals.
Setting and Participants
Participants included adults aged ≥18 years who were receiving in-center hemodialysis 3 times per week at 4 tertiary-care hospitals in Montreal, Canada (Jewish General Hospital [JGH], Centre Hospitalier de l’Université de Montréal [CHUM], Montreal General Hospital, and Lachine Hospital), and had symptoms of depression and/or anxiety as indicated by a score ≥6 on the Patient Health Questionnaire–9 (PHQ-9) and/or the General Anxiety Disorder–7 (GAD-7). 4 Exclusion criteria included significant cognitive impairment suggestive of dementia, suicidal ideation or intent, signs of acute psychosis, difficulty hearing, current psychotherapy, and inability to speak French or English. 4
Of the 400 potential participants at the 4 dialysis units, 112 participants were screened using the PHQ-9 and the GAD-7, and 64 met eligibility criteria. Of the eligible participants, 9 refused and 55 were randomized. Randomization was performed by an independent statistician through a computerized random number generator. The independent statistician transmitted participant group information directly to the interventionists, and the assessors were blinded to the participants’ group assignment. Of the 55 randomized participants, 21/25 (84.0%) participants in the treatment arm and 26/30 (86.6%) participants in the active control arm completed the intervention programs and 8-week follow-up assessments. Of the 47 participants who completed the intervention programs and the 8-week follow-up assessments, 19/21 (90.5%) participants in the treatment arm and 21/26 (80.7%) participants in the active control arm completed the 6-month follow-up assessment (40/47 in total). In this article, we report the 6-month follow-up data from these 40 participants.
Intervention—BMI
In the BMI group, participants received 20-minute chair-side sessions of the intervention twice a week for 8 weeks, while undergoing dialysis. Participants were guided through approximately 15 minutes of mindfulness meditation techniques drawn from Mindfulness-Based Cognitive Therapy (MBCT) in most of the BMI sessions. 4 These techniques included body scanning, mindful eating, guided breath meditation, loving kindness meditation, and mindful movements. 4 Furthermore, participants were taught how to apply mindfulness to daily life and were encouraged to maintain a personal daily mindfulness practice for 10 minutes at home. Participants were invited to ask questions for a few minutes at the end of each session (3-5 minutes). 4 The interventions were delivered through audio headsets in English and French, while a trained interventionist delivered instructions in front of up to 6 participants at a time. One of the interventionists was a psychologist with over 40 years of clinical mental health experience who is a certified MBCT facilitator and MBSR (Mindfulness-Based Stress Reduction) teacher. The other interventionist was a registered social worker with a certification in MBCT facilitation who had maintained a personal mindfulness practice of over 7 years. Each intervention was reviewed and delivered by the same interventionist at all sites to ensure consistency and to control for the effects of the characteristics of the interventionist. 4
Control—HEP
In the HEP group, an interventionist led educational and activity-based sessions, which included topics such as light exercise, sleep, stress and anxiety, nutrition, journaling, and music enjoyment with drawing. Home practice and the implementation of health-enhancing habits were encouraged. 4 Health Enhancement Program was previously designed specifically as an active control for MBI trials to control for several non-program-specific intervention factors such as facilitator attention, expectations of positive change, duration of treatment, intervention format (eg, individual vs group), and time spent on at-home practice.4,12,13 The structure of HEP was equivalent to BMI: HEP was comprised of two 20-minute sessions per week for 8 weeks while patients were undergoing dialysis, encouraged the same amount of home practice (implementing health-enhancing habits for 10 minutes per day), allowed 3 to 5 minutes for questions, and was delivered via audio headsets with the interventionist present. 4
Outcome Measures
Change in depressive symptoms (primary outcome) was measured using PHQ-9 scores at baseline, 8 weeks, and 6 months. The PHQ-9 is a widely used 9-item self-report questionnaire, which assesses depressive symptom severity. 14 Change in anxiety symptoms (secondary outcome) was measured using the GAD-7 scale at baseline, 8 weeks, and 6 months. The GAD-7 is a 7-item scale measuring symptoms of anxiety. 15 All questions on the PHQ-9 and GAD-7 self-report scales were scored from “0” (not at all) to “3” (nearly every day).11,15 The PHQ-9 and GAD-7 questionnaires are both widely used, reliable, and validated self-report scales.14,16 To determine participants’ likelihood of hospitalization (exploratory outcome), hospitalization data (date and site of hospitalization) were collected from participants who were hospitalized between the start of the intervention and 6-month follow-up.
Data Analysis
Baseline demographic and clinical characteristics were compared between the treatment and control groups using chi-square tests to assess adequacy of randomization among participants who completed the 6-month follow-up. To determine whether BMI is more efficacious than HEP at reducing PHQ-9 depression scores (primary outcome) and GAD-7 anxiety scores (secondary outcome) over the 6-month follow-up period, 2-way mixed analyses of variance17,18 (ANOVAs) were conducted on 6-month follow-up PHQ-9 and GAD-7 scores separately, with the treatment group (BMI and HEP) as the between-subject factor and time (baseline, 8 weeks, and 6 months) as the within-subject factor. Normality of PHQ-9 and GAD-7 scores was assessed using the Kolmogorov-Smirnov test.
19
Post hoc t tests were used to compare treatment groups at each of the 3 time points for any significant interaction effects between time and treatment group, using a Bonferroni correction.
20
Measures of effect size at 90% confidence intervals (CIs) were performed using
Results
Out of the 47 participants who completed the intervention programs and the 8-week follow-up assessments, 19/21 (90.5%) participants in the treatment arm and 21/26 (80.7%) participants in the active control arm completed the 6-month follow-up assessment and were analyzed (n = 40; Figure 1). Baseline demographic and clinical characteristics of participants who were analyzed at 8-week follow-up were previously reported. Available baseline demographic and clinical data for the 6-month follow-up sample are displayed in Table 1. In the 6-month follow-up BMI group, the mean age was 57.2 ± 11.6 and 26.3% of the group was female. Sex and gender coincided for all participants. In the HEP group, the mean age was 64.5 ± 11.4, and 47.6% of the group was female. There were no statistically significant differences between groups on any baseline demographic or clinical characteristics.

Participant flowchart.
Six-Month Follow-up Baseline Demographic and Clinical Information.
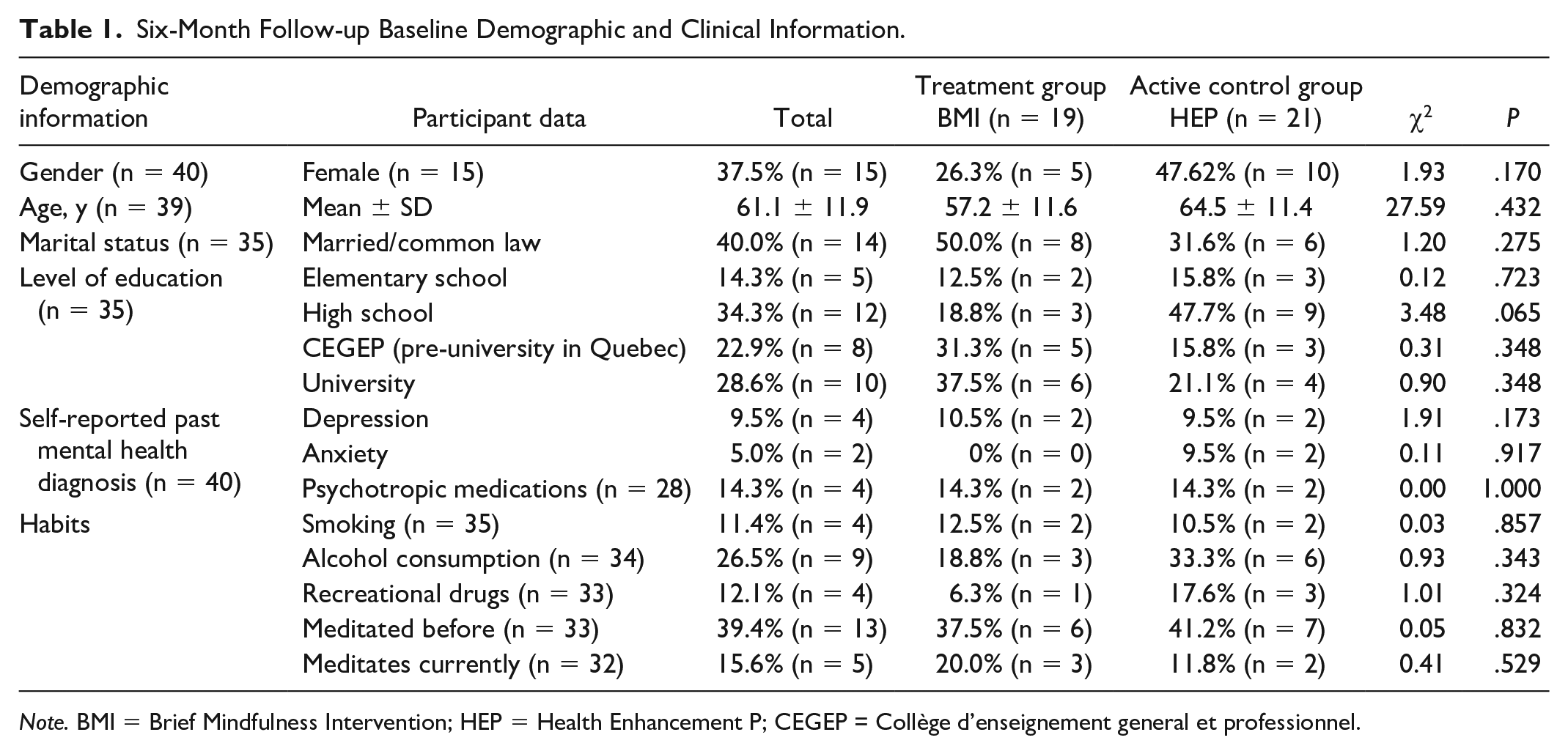
Note. BMI = Brief Mindfulness Intervention; HEP = Health Enhancement P; CEGEP = Collège d’enseignement general et professionnel.
There was no statistically significant interaction between the intervention and time on PHQ-9 scores at 6 months, F(1, 38) = 0.20, P = .65,
Two-Way Mixed ANOVA Results for PHQ-9 Depression Scores.

Note. ANOVA = analysis of variance; PHQ-9 = Patient Health Questionnaire–9; CI = confidence interval; Num DF = number of degrees of freedom in the model; Den DF = number of degrees of freedom associated with the model errors.
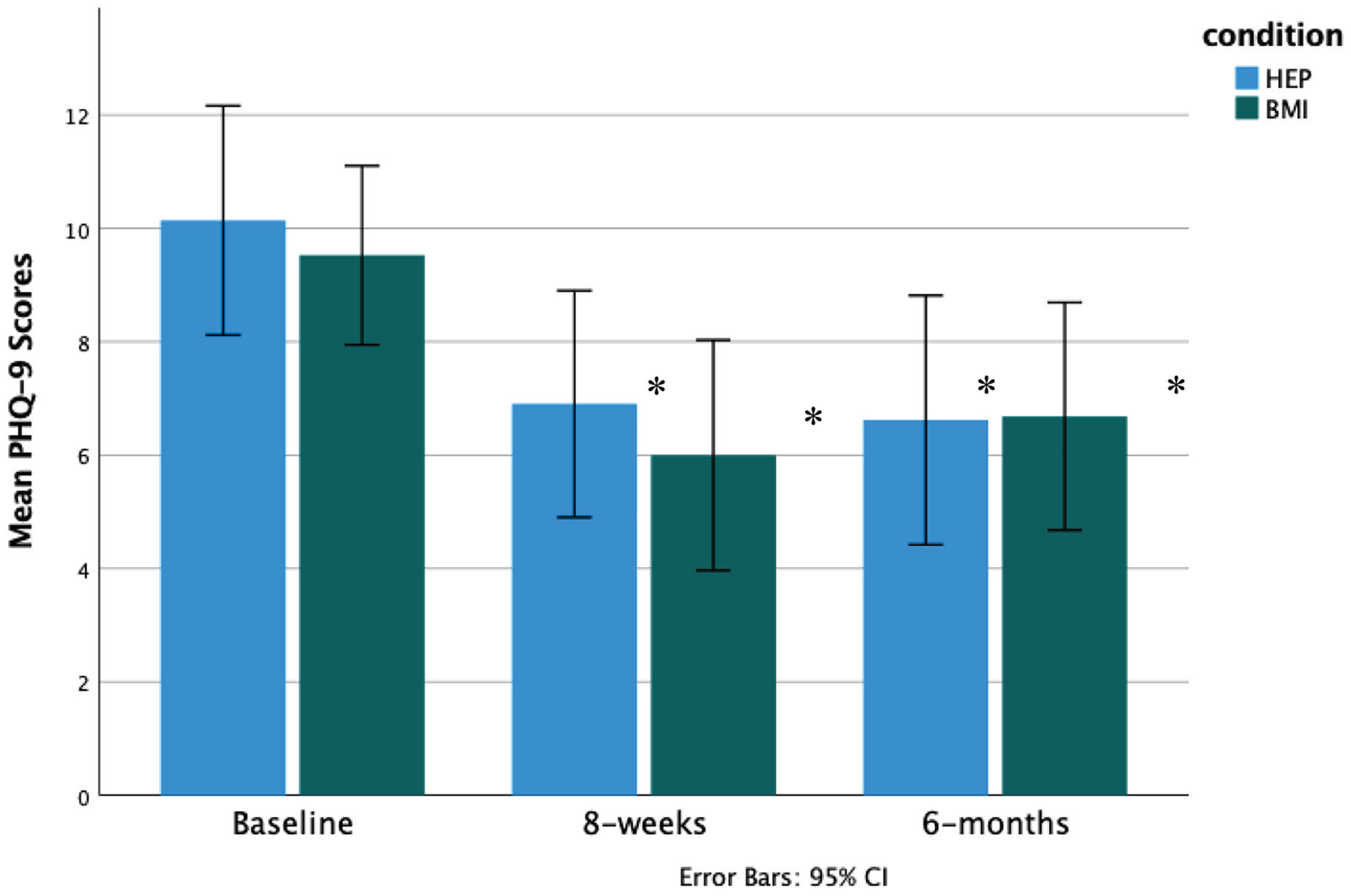
Change in PHQ-9 depression scores over time BMI versus HEP.
Two-Way Mixed ANOVA Results for GAD-7 Anxiety Scores.

Note. ANOVA = analysis of variance; GAD-7 = General Anxiety Disorder–7; CI = confidence interval.

Change in GAD-7 anxiety scores over time BMI versus HEP.
Exploratory repeated-measures t tests examining the differences in PHQ-9 and GAD-7 scores (separately) between baseline and 6 months highlight these findings (Table 4). In the BMI group, there was a statistically significant difference from baseline to 6 months on PHQ-9 scores, 2.84 ± 4.14, 95% CI = [0.85, 4.84], t(18) = 2.99, P = .008, with a medium effect size (d = 0.69), as well as a statistically significant difference from baseline to 6 months for GAD-7 scores (4.68 ± 4.39, 95% CI = [2.56, 6.80], P < .000) with a large effect size (d = 1.07). In the HEP group, there was only a statistically significant difference in PHQ-9 scores from baseline to 6 months, 3.52 ± 4.16, 95% CI = [1.62, 5.42], t(20) = 3.875, P = .001, with a large effect size (d = 0.85). Therefore, both BMI and HEP seem to be efficacious in significantly reducing depressive symptoms in the long term, but only BMI seems to be efficacious in reducing anxiety symptoms.
Repeated-Measures t Test Results.

Note. CI = confidence interval; BMI = Brief Mindfulness Intervention; PHQ-9 = Patient Health Questionnaire–9; GAD-7 = General Anxiety Disorder–7; HEP = Health Enhancement Program.
Based on the KM survival curves (Figure 4), participants in the BMI group had a mean time to hospitalization of 154.26 days (95% CI = [129.72, 178.81] days), and participants in the HEP group had a mean time to hospitalization of 163.95 days (95% CI = [145.66, 182.25] days). Median survival times are not reported because more than 50% of participants in both groups were not hospitalized by the end of the 6 months. Similar percentages of censored cases (participants who were not hospitalized) were present in the BMI (73.7%) and HEP (76.2%) groups. The log-rank test showed non-significant results for differences between groups, χ2(1) = 0.07, P = .78. These findings suggest that BMI was not more efficacious than HEP in reducing participants’ likelihood of hospitalization.

Likelihood of hospitalization BMI versus HEP.
Discussion
To our knowledge, this is the first RCT examining the long-term efficacy of an 8-week BMI (vs a HEP control) in reducing depressive and anxiety symptoms, as well as likelihood of hospitalization, in patients receiving dialysis. We previously found that BMI and HEP may be helpful interventions for depressive symptoms, while BMI appeared to be superior to HEP for anxiety symptoms. 4 Here, we report follow-up data showing that these improvements are sustained at 6-month follow-up. Both BMI and HEP were associated with significant reductions in depression scores over 6 months, but BMI did not appear to be superior to HEP. Only BMI appeared to significantly reduce anxiety scores at 6 months. There was no significant difference between groups for likelihood of hospitalization, but 73.7% of BMI participants were not hospitalized between baseline and 6 months.
Although there is a lack of literature about MBIs in patients undergoing dialysis, our finding that both BMI and HEP were associated with reductions in depressive symptoms in patients receiving dialysis is consistent with the literature on MBIs for patients with and without cancer with depressive symptoms. Results of a large RCT (n = 118) comparing the efficacy of an 8-week Mindfulness-Based Group Therapy (MGT) with Treatment as Usual (TAU) in reducing depressive symptoms in participants diagnosed with depression, anxiety, and stress disorders were similar to our findings. 25 A statistically significant improvement was found in patients’ depressive symptoms (including the PHQ-9 scores) at 1-year follow-up in both groups. 25 Furthermore, a meta-analysis of 7 RCTs examining the effectiveness of MBIs in improving depression in patients with cancer found that MBIs were associated with a significant decrease in depression for up to 12 weeks after the end of the MBIs. 26 An important difference between these meta-analyses and our study is that the studies in the meta-analyses used either TAU, waitlist, or general education as a control, whereas we used an active control (HEP). It is interesting that depression scores were reduced both in the HEP group and in the BMI group, and that these effects were sustained at 6 months for both groups. Numerous elements of HEP, such as light exercise, music/art therapy, healthy eating, and learning about anxiety and stress, are similar to elements of a structured psychoeducation program with effect magnitudes comparable with those of psychotherapies such as cognitive behavioural therapy (CBT). 4 Thus, the efficacy of HEP in reducing depressive symptoms may be due to HEP being a strong active control in addition to non-specific factors.4,26
Our findings that symptoms of anxiety only appeared to significantly decrease in the BMI group over 6 months are consistent with the literature for short-term and long-term effectiveness of MBIs in reducing anxiety among patient populations with medical and psychological diagnoses. 27 A meta-analysis of 9 RCTs (n = 965) comparing MBIs with usual care, waitlist, or no intervention, in cancer patients (with the majority undergoing hematopoietic stem cell transplants) found that MBIs reduced the severity of anxiety at ≤1 month postintervention and at 1 to 6 months postintervention. 27 Furthermore, a review of 17 studies examining the long-term effects of MBIs in improving anxiety (mean length of follow-up = 27 weeks) in patients with psychiatric conditions (including depression and generalized anxiety disorder) and medical conditions (including cancer) suggested that MBIs improved symptoms of anxiety across a wide severity range, as well as symptoms associated with medical conditions. 10 Similar to our findings, these improvements were associated with medium effect sizes (Hedges’s g = 0.60). 10 It is interesting that in our study, symptoms of anxiety significantly improved only in the BMI group, and these effects were sustained over 6 months, which was not the case for HEP. This may reflect that specific elements of the BMI, such as its mindfulness and/or CBT components, were more efficacious than HEP in sustaining anxiety symptom reductions in the long term for patients receiving dialysis. Anxiety presents an exciting target for the long-term effects of MBIs, especially given that it is associated with poorer health outcomes in patients receiving dialysis, independently of depression. 28
Although we found that BMI was not more efficacious than HEP in reducing the likelihood of hospitalization in patients receiving dialysis, more than 70% of participants in each group were not hospitalized from baseline to 6 months. Depression and anxiety have been found to be significant predictors of hospitalization in patients receiving dialysis.5,29 Furthermore, a longitudinal study found that in 159 patients undergoing dialysis over a 12-month period, 13% to 18% had new onset of depression and anxiety symptoms. 29 To our knowledge, there is no research on the effects of psychosocial interventions or MBIs on reducing the likelihood of hospitalization in patients receiving dialysis, but MBCT has been shown to be efficacious as treatment for relapse prevention of recurrent depression, 30 and MBTs have been shown to be effective in reducing anxiety in the long term. 28 Although our results were not statistically significant, this may be due to our modest sample size, rather than the intervention itself being ineffective in reducing the likelihood of hospitalization for patients receiving dialysis. Future research could examine the association between BMI and patients receiving dialysis likelihood of hospitalization with a larger sample.
Strengths and Limitations
This study has numerous strengths. To our knowledge, it is the first study examining the long-term effects of an MBI for patients undergoing hemodialysis. Indeed, even more generally, there is little research on the long-term effects of MBIs for depression and anxiety. Another strength is the length of this study’s follow-up period (6 months), which is common in the literature on clinical trials of psychological interventions. 31 Furthermore, a longitudinal cohort study (n = 439) examining the effect of low-intensity CBT for depression and anxiety symptoms reported that around 70% of relapse events (ie, relapse in depressive and/or anxiety symptoms) are detected in the first 4 months following treatment (ie, over 6-month follow-up). 32
A limitation of our study was the modest sample size. Attrition is common in long-term follow-up periods, but our study had a high retention rate at 6-month follow-up (85.1%). Another limitation was the lack of a waitlist control, which prevents us from conclusively distinguishing the effects of the interventions from other non-specific factors, such as regression to the mean, repeated measurements, or natural fluctuations in symptoms. These findings should be confirmed in an RCT with a larger sample, ideally with a waitlist control arm in addition to an active comparator.
Conclusions
Here, we present 6-month follow-up data from an RCT examining the effects of BMI (compared with HEP) in reducing depression and anxiety symptoms, as well as the likelihood of hospitalization in patients undergoing hemodialysis. Both BMI and HEP had sustained efficacy in reducing depressive symptoms at 6 months. Of note, BMI appeared to be more efficacious than HEP in reducing anxiety symptoms in this population. Both BMI and HEP may thus be useful treatments with long-term benefits for patients receiving dialysis, but BMI may be more desirable given its efficacy in reducing both depressive and anxiety symptoms, benefits that are sustained in the long term. Future research could expand on these results by studying the long-term effects of BMIs in depression and anxiety with larger sample sizes, and in comparison with other psychosocial interventions to further establish the long-term efficacy of BMIs for depression and anxiety in this population.
Footnotes
Ethics Approval and Consent to Participate
The study was approved by the Research Ethics Boards at all participating hospitals. All participants provided informed written consent.
Consent for Publication
Consent for publication was provided by all authors.
Availability of Data and Materials
Not Available.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Soham Rej received an investigator-initiated grant from Satellite Healthcare to conduct this study and receives a salary award from the Fonds de Recherche Québec Santé.