
Abstract
Background:
Low physical activity levels and poor physical functioning are strongly associated with poor clinical outcomes and mortality in adult kidney failure patients, regardless of treatment modality. Compared with the general population, individuals with chronic kidney disease are physically inactive, have reduced physical abilities and difficulties performing routine daily tasks, lower health-related quality of life, and higher cardiovascular morbidity and mortality. In addition, frail kidney failure patients have higher hospitalization and mortality rates as compared with other kidney failure patients. Evidence suggests that assessment and recommendations for physical activity should be part of standard care for kidney failure patients. Structured exercise can improve physical function and quality of life in frail older adults and may be used specifically for management of frailty in kidney failure. However, research is needed to determine best practices for implementation of physical function measurements and physical activity promotion in standard kidney failure care.
Objective:
The proposed Move More study will assess the feasibility of a physical activity intervention offered to the kidney failure inpatients in Calgary, Alberta. Specifically, this study is designed to examine the effects of an early physical activity/mobility intervention led by a kinesiologist, and supported by the clinical care team including physiotherapists (PT) and nurse clinicians.
Methods:
The Move More study is a single-arm pilot intervention examining feasibility and optimal improvement in real-world conditions. Kidney failure inpatients at the Foothills Medical Centre will be recruited to participate. Patients will receive an individualized in-hospital physical activity/mobility intervention. Frailty and physical function will be assessed at baseline and postintervention prior to hospital discharge. The goal is to recruit 24 to 36 patients.
Conclusions:
Evidence needed to support the inclusion of mobility and physical activity as part of standard care will be gathered, with knowledge gained used to help direct future physical activity programming for kidney failure inpatients.
Background
Chronic kidney disease (CKD) prevalence is now as high as 71.9 per 1000 individuals in Canada. 1 CKD is associated with high morbidity, mortality, and poor clinical outcomes, leading to challenges for patients, families, and health care providers. 2 As CKD progresses to kidney failure, these issues are exacerbated, and health care costs for patient care increase due to required dialysis, long transplant waiting times, and high hospitalization rates.2,3 Individuals with kidney failure are often physically inactive and have reduced physical abilities and difficulties performing routine daily tasks, lower health-related quality of life (QOL), and higher cardiovascular morbidity and mortality compared with the general population.4-6 Due to frailty and reduction in functional independence, many persons with kidney failure require frequent readmissions to hospital with prolonged lengths of stay, eventually leading to a higher rate of admission to long-term care facilities. 7
Evidence suggests that physical activity assessments and recommendations should be included in advanced kidney care. 8 Patients with kidney failure experience high levels of fatigue, deconditioning, and poor QOL. 8 Physical activity also improves physical performance, and self-reported function, as well as blood pressure and maximal exercise capacity9-11 in patients with kidney disease. In addition, physical activity has been shown to improve QOL and cognitive function while reducing symptoms of depression in kidney patients. 10 Similarly, a randomized controlled physical activity intervention for elderly medical inpatients demonstrated improved physical function and reversed the typical functional decline associated with hospitalization. 12 In addition, researchers measured positive changes in cognitive and mood status, QOL, length of stay, falls, and readmissions 3 months after discharge. 7 Evidence suggests that critically ill patients who undergo physical activity interventions have enhanced functional capacity, strength, mobility, QOL, reduced length of stay, and a higher probability of being discharged home. 13
Due to general deconditioning and increased muscle wasting, the prevalence of frailty and limited physical function in kidney failure patients is high. 11 More than 60% of kidney failure patients are considered frail, compared with only 11% of older adults. 14 Frailty increases the risk of health complications such as falls, cardiovascular events, hospitalization, disability, reduced QOL, and mortality.10,15-17 Therefore, the management of frailty is central to kidney failure care. Physical activity interventions show promise for managing frailty in geriatric populations. 18 A systematic review of physical activity for frail individuals found high adherence and no adverse events in most studies, concluding that physical activity is safe and feasible for an aging population, with greater impact during early stage frailty. 18 Furthermore, kidney failure patients are interested in increasing physical activity and improving their physical function. 2 Research is thus needed to identify optimal strategies to implement physical function assessments and promote physical activity in kidney failure care. 11
The purpose of the proposed study is to assess the feasibility and preliminary efficacy of an early physical activity intervention in the care of kidney failure inpatients. It is hypothesized that the intervention will be feasible to administer and for patients to participate in.
Methods
Study Design
The Move More study is a single-arm pilot intervention examining feasibility and optimal improvement in real-world conditions. An overview of study procedures is shown in Figure 1. Ethical approval was obtained through the Conjoint Research Ethics Board of the Faculties of Medicine at the University of Calgary (REB18-2134).
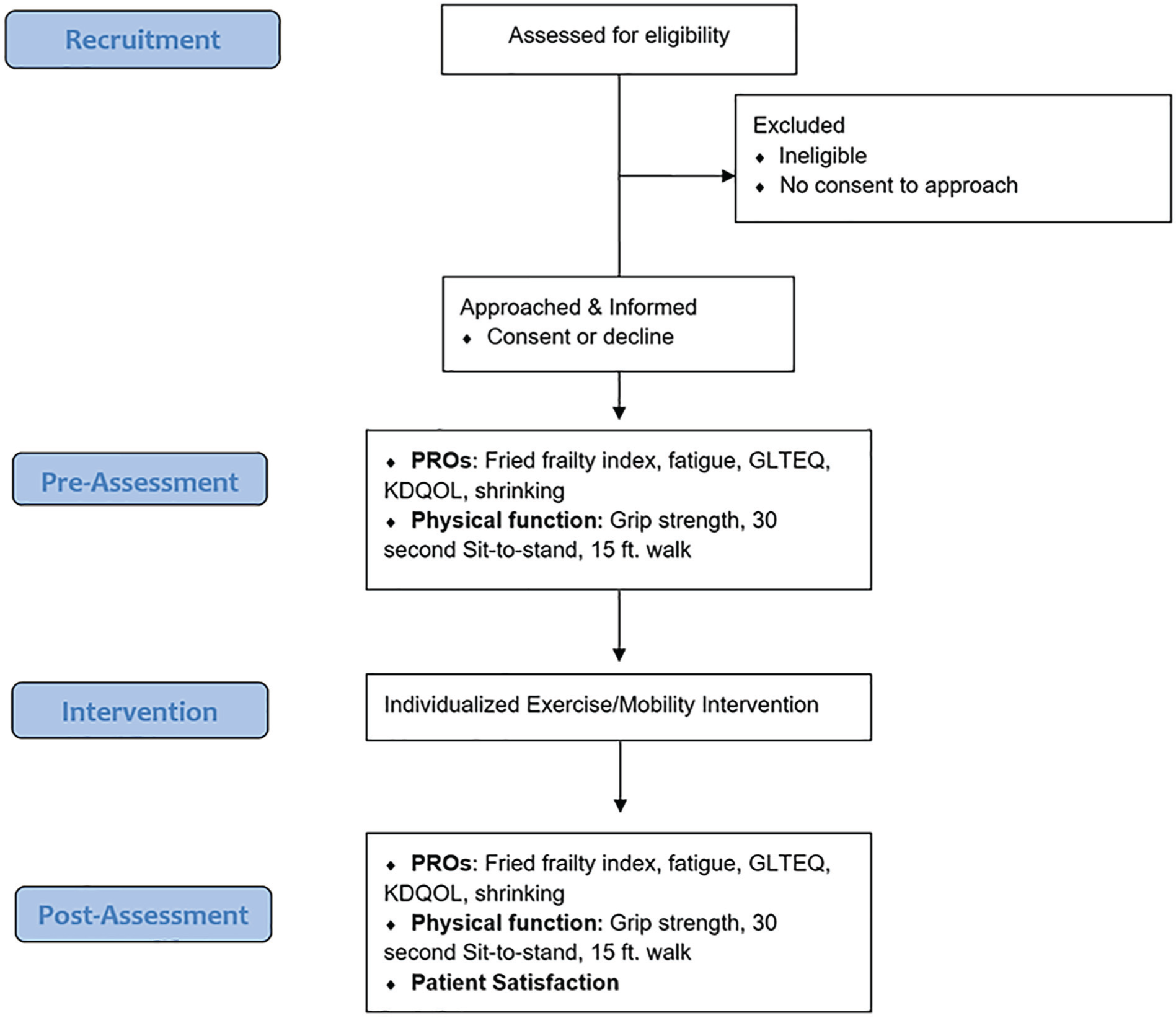
Flowchart of study design.
Participants/Study Population
Kidney failure inpatients on Unit 37 at the Foothills Medical Centre in Calgary, Alberta, will be invited to participate. Eligibility criteria are (1) kidney failure inpatients on maintenance dialysis (hemodialysis or peritoneal dialysis), (2) Anticipated Date of Discharge (ADOD) greater than 7 days, and (3) deemed medically stable to participate in physical activity by a nurse or nurse clinician. Exclusion criteria due to medical instability are defined as (1) unstable vital signs, poor oxygen saturation on room air, (2) decreased level of consciousness, confusion, (3) febrile (temperature >38.3oC), (4) chest pain or shortness of breath at rest, (5) signs of GI bleed, (6) pain which can be potentially exacerbated by physical activity intervention, or (7) a permanent negative change in medical status (eg, change to palliative care). Patients will remain enrolled if there is a temporary decline in medical status that prevents participation if the patient is expected to recover. Due to the variability in medical care for maintenance dialysis patients, patients will remain enrolled in the study if there is a temporary transfer off the kidney inpatient unit to another unit for procedures or other medical interventions. Patients who are permanently transferred to another unit will be discharged from the study.
Study Procedure
Eligible participants will be identified by nurse clinicians or the research coordinator. The patient will then be presented with a consent to contact by unit staff before receiving further information about the study from the research team. Those who agree to participate will sign an informed consent form before completing a baseline assessment and exercise education session to learn how to perform tailored exercises with a kinesiologist. The kinesiologist will supervise exercise with the patient 1 to 3 times per week, and the unit staff will monitor and record all exercise sessions.
Standard of Care
Standard of care for Unit 37, physiotherapy (PT), and/or occupational therapy (OT) are essential in discharge planning. PT and/or OT will see patients who have acute care goals or acute needs to improve function to a level where they can be safely discharged from hospital. The addition of a kinesiologist to the care pathway will allow for mobility interventions in patients who would not otherwise be seen by PT or OT, including (1) independent patients or those with baseline function to focus on preventing functional decline while in hospital, (2) patients discharged from physiotherapy due to a plateau in function or achievement their acute care goals but are still waiting for medical management or placement to a care facility, and (3) patients from long-term care facilities without acute care goals.
Physical Activity Intervention
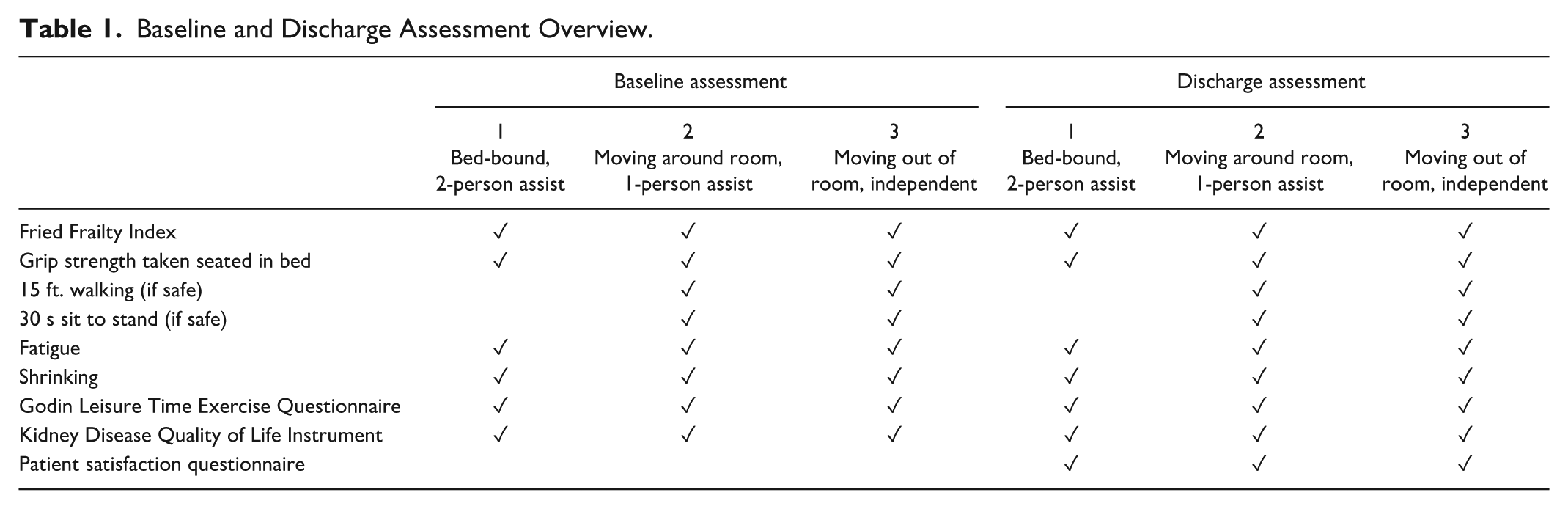
Inpatients will receive an individualized physical activity intervention according to baseline measures. Table 1 specifies measures collected at baseline and discharge. Patient mobility is determined by a review of charts and nursing/ PT notes to determine level of assist. There are three intervention phases, (1) bed-bound (two-person assist/full lift), (2) moving around room (one-person assist), and (3) moving out of room (independent), each with its own exercise protocol (Table 2). Exercise will be tailored based on phase and participant’s exercise preferences.
Baseline and Discharge Assessment Overview.
Physical Activity Intervention.

Participants will complete prescribed exercises daily and progress as determined by the Kinesiologist. All exercise will be done on the unit, off of dialysis. Strength exercises will be selected from the Vivifrail Multi-Component Physical Exercise Program that has shown positive effects in elderly inpatients. 19 A target exercise intensity of 2 to 3 on the 10-point Borg rating of perceived exertion scale will be used, which is considered best practice in advanced kidney disease settings.20,21 In addition, participants will be encouraged to perform exercises beyond their daily prescription as tolerated.
Measures
Primary outcomes
The primary outcome of the study is the feasibility of administering an individualized early exercise/mobility intervention. As PT and OT usually only addresses acute care needs, kinesiology involvement to create early and ongoing mobility will be examined. Feasibility measures include (1) recruitment: those eligible, approached, consent/no consent, reasons for refusal, numbers participating, numbers recruited from advertising; (2) completion of the prescribed exercise/mobility intervention and reasons for noncompletion/withdrawal (recorded on the Electronic Medical Record [EMR]); (3) participant and health care practitioner (HCP) satisfaction with the exercise intervention, measured by satisfaction surveys; (4) HCP completion of clinical charting for FITT prescription (date, frequency, intensity, duration, type of exercise; progression through strengthening exercises) and level of assist needed (if any); (5) participant assessment; and (6) reporting of adverse events related to participation in the in-hospital exercise program. Feasibility will include 60% recruitment rate, 50% assessment completion, no adverse events related to the intervention, and high satisfaction as reported by both the participants and HCPs.
Secondary outcomes
Secondary outcomes of this study are frailty, functional measures, QOL, number of falls in-hospital, hospital length of stay (LOS), and 30-day readmissions. Frailty, functional measures, and QOL will be assessed at baseline and postintervention prior to hospital discharge. Hospital LOS and 30-day readmissions will be gathered from EMRs.
Frailty
A standardized definition of frailty was established in community-dwelling older adults 22 and utilized in kidney failure. 17 According to the Fried Frailty Index, frailty is defined as a clinical syndrome in which 3 or more of the following criteria are present: unintentional weight loss (10 or more pounds in the past year), self-reported exhaustion, weakness (grip strength), slow walking speed, and low physical activity. 22 If present, each criterion is given 1 point. A total score of equal to or less than 1 classifies the patient as nonfrail, 2 points is prefrail, and 3 or more points is considered frail. 22
Physical activity behavior
As part of the Fried Frailty Index, the Godin Leisure Time Exercise Questionnaire (GLTEQ) will measure usual physical activity habits. 23 The GLTEQ was used to assess physical activity behavior in many populations, including kidney patients.24,25 The GLTEQ will be assessed as outlined in Table 3.
Fried Frailty Index Scoring Values.
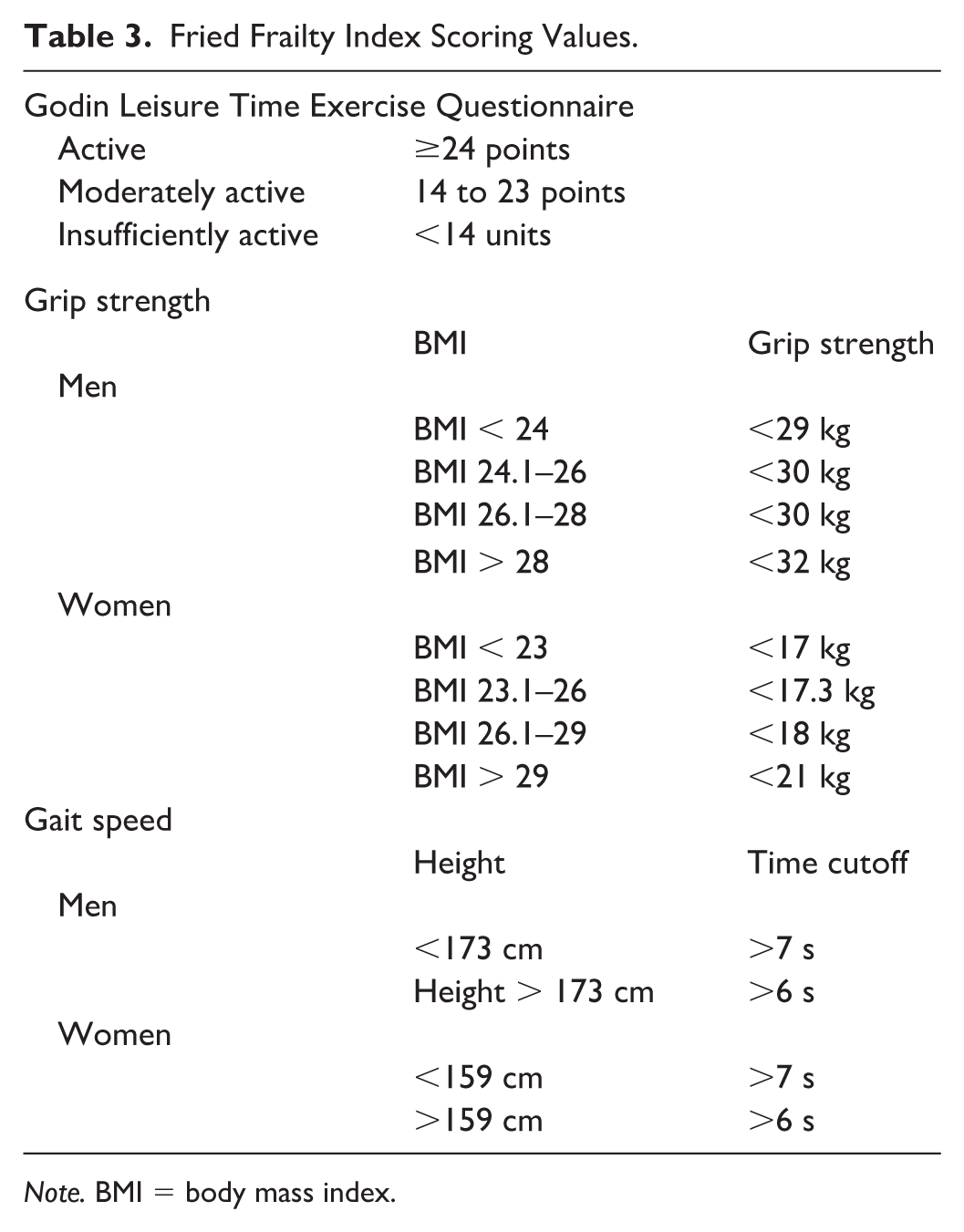
Note. BMI = body mass index.
Quality of life
The Kidney Disease Quality of Life Instrument (KDQOL) 26 is a 36-item self-report measure. It is designed to assess the QOL of individuals with CKD and kidney failure, including the burden of the disease, symptoms, and specific QOL questions.
Musculoskeletal functional measures
Lower body strength will be assessed using the 30-second Sit to Stand Test. 27 Upper body strength will be assessed using a Jamar hand grip dynamometer (Performance Health, Hydraulic, Illinois, USA), which has widely used in various chronic illnesses. 28 Patients will complete 3 trials per side and the highest value in kilograms from each will be taken and added together to get a cumulative value. Grip strength for frailty will be assessed as outlined in Table 3.
Walk speed will be assessed using the 15 ft. walking test. 22 Patients walk 15 ft. at a normal walking pace and the time it takes for them to complete this is recorded in seconds. 22 Walk speed test scoring is outlined in Table 3. Physical function tests may be skipped if patient medical or functional status prevents assessment.
If the patient’s grip strength is below the cutoff for their given BMI, then the person receives a 1 for this component of the Fried Frailty Index. If their grip strength is above the cutoff, then the person will receive a 0.
If the patient’s gait speed is slower than the cutoff, they receive a 1 for Fried phenotype. If it is faster than the cutoff, they receive a 0.
Demographics
Demographics and medical variables will be obtained by study staff via chart review. This includes age, gender, height, date and reason for admission (diagnosis), date of discharge, weight at admission and discharge, location discharged to, cause of kidney disease, type of dialysis, dialysis vintage, if there is a change in dialysis type while in hospital, comorbidities (eg, diabetes, hypertension, heart disease, stroke, peripheral vascular disease, neuropathy, retinopathy, chronic infections/wounds, amputations, falls), referral date, withdrawal and reason for withdrawal, and walking/mobility aids utilized. Hospital LOS and readmission rates over 30 days will be obtained by EMR review after patient discharge.
Sample size
All kidney failure patients admitted to the Nephrology Inpatient Service at the Foothills Medical Centre in Calgary requiring dialysis and meeting the inclusion criteria will be approached for participation in the feasibility study. As a feasibility study, no a priori sample size calculation was performed. It is anticipated that 24 to 36 patients will be recruited over 12 months.
Analysis
Participant demographics and outcomes will be summarized using descriptive statistics. For normally distributed continuous variables, means and standard deviation will be calculated. Nonnormally distributed continuous variables will be presented using median and interquartile range. For categorical variables, frequencies and percentages will be presented. Within-group changes in secondary outcomes of frailty, physical activity, QOL, and physical function will be examined using dependent sample t tests if normally distributed, the Mann-Whitney U test if nonnormally distributed, or Wilcoxon signed rank test if categorical. Descriptive statistics will be used to provide an overview of additional measures for LOS, in-hospital falls, and readmission. All analyses will be completed using SPSS statistics, version 26.0 (IBM, Markham, Ontario, Canada).
Dissemination
The results for the primary and secondary outcomes will be published upon study completion. Information from the study will also be disseminated to the staff and management on Unit 37 as well as the Department of Nephrology at the Foothills Medical Centre to encourage knowledge translation into clinical practice.
Discussion
Statement of Principal Outcomes
The proposed study will examine the feasibility and optimal improvement in real-world conditions of implementing an early physical activity intervention with kidney failure inpatients. Physical activity training can improve cardiovascular function and outcomes in kidney failure patients with limited physical function, which is associated with poor clinical outcomes and increased health care expenditures.8,11 This work will improve our understanding of the feasibility of physical activity in kidney failure inpatients and will begin to gather information on the potential ability to improve frailty, QOL, and reduce hospital LOS and rate of readmissions. Integrating an individualized physical activity regimen is part of the approach to management of frail patients with kidney failure. 14 The current study will also add to current literature on the psychosocial benefits of physical activity on QOL in kidney failure patients.24,26
Strengths and Limitations
A key strength of the proposed study lies in the integration of kinesiologists into the already diverse preexisting therapy team, consisting of physiotherapists, occupational therapists, and their assistants. A kinesiologist will support the clinical staff promote recruitment for mobility and activity services, and will ensure patient flow with the existing therapy team. Furthermore, a wide range of existing therapy equipment will be available to the kinesiologist to individualize exercise programming. The presence of a kinesiologist on the unit throughout the week also allows for constant monitoring and adaptation to enhance safety, adherence, and likely intervention effectiveness.
Due to the single-arm nature of the proposed research, we will not be able to discern between intervention effects and natural patient changes. This feasibility study will recruit a small sample of kidney failure inpatients, which limits statistical power to detect changes and may result in a homogenous participant population, reducing generalizability. As commonly seen in physical activity interventions, study participation may be biased toward highly motivated individuals with a strong history of physical activity. Although we will assess feasibility of integrating kinesiology-supported physical activity and mobility into standard kidney care, differences between our clinical environment and population compared with other locations may prevent direct translation of our intervention to other clinics. Therefore, the feasibility and optimal implementation of physical activity interventions must be assessed in various environments, while larger randomized controlled trials will be required to improve generalizability and address the intervention effectiveness.
Meaning of the Study: Possible Implications for Clinicians or Policy Makers
Kidney failure patients have a higher rate of admission to the hospital compared with the general population. 6 There are significant financial costs and emotional consequences of admission to the hospital. 6 In Canada, kidney failure has an economic burden of $1.0 billion, of which 69% is direct health care costs. 29 Management of frailty using the proposed physical activity intervention has the potential to decrease length of hospital stay and readmissions for kidney failure patients, reducing patient and health care burden.
Ongoing research aims to better understand the impact of exercise on kidney failure inpatients, adding to evidence on the value of early mobilization in critically ill patients for improving physical function at discharge. 13 The proposed study will inform the feasibility of delivering and participating in daily exercise (as charted by clinical staff and individual patient report) as part of routine kidney failure inpatient care. Last, physical activity for kidney failure inpatients has the potential to improve functioning, enhance patient outcomes, reduce hospital LOS, and enhance overall QOL.
Unanswered Questions and Future Research Directions
There is a lack of rigorous work examining exercise interventions for critically ill patients as well as limited research in kidney failure inpatients. 13 As such, the proposed work will help to establish feasibility of physical activity interventions in this population and kinesiologist integration within inpatient units. If feasibility is shown herein, larger randomized controlled trials will be required to examine intervention effectiveness. Multisite research will be necessary given the size of the kidney failure population. The implementation of physical activity interventions in various clinical settings will help to inform feasibility and best practices for different environments to improve generalizability. Future research is also needed to optimize exercise prescriptions for kidney failure inpatients by varying frequency, intensity, time, and type. Finally, explorations of cost-effectiveness for kinesiologist integration in clinical care will determine if and in what capacity such specialists should be included in kidney failure clinical teams.
Physical activity in kidney failure inpatients may benefit patients long after their discharge from the hospital. As we work to optimize in-hospital physical activity interventions and shift the culture on inpatient units, patients may continue to benefit in terms of function, QOL, and overall health as resources as the integration of kinesiology services become more prevalent.
Supplemental Material
sj-pdf-1-cjk-10.1177_2054358120987052 – Supplemental material for A Physical Activity Intervention Feasibility Study for Kidney Inpatients: A Basic Research Protocol
Supplemental material, sj-pdf-1-cjk-10.1177_2054358120987052 for A Physical Activity Intervention Feasibility Study for Kidney Inpatients: A Basic Research Protocol by Kathryn Wytsma-Fisher, Stefan Mustata, Theresa Cowan, Manuel Ester and S. Nicole Culos-Reed in Canadian Journal of Kidney Health and Disease
Footnotes
Acknowledgements
The authors gratefully acknowledge the support provided by James K. Gray and family.
Ethics Approval and Consent to Participate
Ethical approval was obtained via The University of Calgary Conjoint Health Research Ethics Board (CHREB) under ID REB18-2134. All participants provided consent to approach for initial meeting with the research team. Following that, all participants provided written consent to participate in the study.
Consent for Publication
All authors have reviewed the manuscript and provided their consent for publication.
Availability of Data and Materials
Data and materials are available from authors upon request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.