
Abstract
Background:
Low physical activity and functional impairment are prevalent and unaddressed in people receiving peritoneal dialysis (PD). Exercise has been shown to improve physical function and mental health for people with kidney disease.
Methods:
Cross-sectional descriptive survey aimed at identifying the exercise and physical activity perceptions and practice patterns of people receiving PD. The survey was developed and pretested with persons living with kidney disease, PD clinicians and exercise specialists.
Results:
There were 108 respondents (people receiving PD) with the majority from Canada (68%) and the United Kingdom (25%). Seventy-one per cent were engaged in physical activity two or more times per week. Most (91.8%) believed that physical activity is beneficial, and 61.7% reported healthcare provider discussion about physical activity. Perceptions regarding weightlifting restrictions varied: 76% were told not to lift weight with a maximum amount ranging from 2 kg to 45 kg. Few (28%) were instructed to drain PD fluid prior to physical activity. Mixed advice regarding swimming ability was common (44% were told they could swim and 44% were told they should not).
Conclusions:
Knowledge gaps suggest that education for both healthcare providers and patients is needed regarding the practice of exercise for people living with PD. Common areas of confusion include the maximum weight a person should lift, whether exercise was safe with or without intrabdominal PD fluid in situ and whether swimming is allowed. Further research is needed to provide patients with evidence-based recommendations rather than defaulting to restricting activity.
Introduction
Although life participation is a core peritoneal dialysis (PD) patient-reported outcome that requires physical activity engagement and adequate physical function, 1 low physical activity and functional impairment are highly prevalent and unaddressed in people receiving PD. 2 –4 Functional impairment in turn is associated with decreased physical activity, decreased life participation and poorer quality of life. 5 Poor physical function is also associated with increased risk of PD technique failure and mortality. 6,7
Exercise has been shown to improve physical function and mental health for people with kidney disease, 8 as well as improve kidney failure-related symptoms, including restless legs, cramping, fatigue and insomnia. 9,10 Small regional studies have provided some insights into PD exercise practices and perceptions. 11,12 However, little is known about exercise practice patterns or perceptions of people receiving PD across the world. 8 This information is important in view of the lack of large, randomised trials to inform evidence-based recommendations for activities such as weightlifting restrictions, optimal core strengthening activities and swimming in this unique population. In response to this knowledge gap, PD programmes provide inconsistent guidance regarding which of these activities are advisable. Describing the physical activity and exercise practices and perceptions of people living with PD is the first step to inform patient education, future areas of research and clinical recommendations in this area. Therefore, the primary aim of this study was to determine the exercise perceptions and practices of people receiving PD around the world. Our secondary objectives were to examine differences in perceptions and practices across respondent regions.
Methods
Study design and participants
This study is a cross-sectional descriptive survey aimed at identifying the exercise and physical activity perceptions and practice patterns of people receiving PD living in countries represented by Global Renal Exercise Network (GREX) members. This network aims to foster collaborative research and innovation in physical activity and exercise across multiple disciplines to optimise health outcomes in people with kidney disease and includes over 200 members from 38 countries (https://grexercise.arizona.edu) The survey was a web-based 25-item questionnaire (16 perception and practice questions, 9 demographic questions) developed and pretested with persons living with kidney disease, PD clinicians and exercise specialists. (Online Supplemental material Appendix 1). The English version of the survey was translated into the other official language of Canada, French, for distribution. People who were currently or previously on PD and who were over the age of 18 years were invited to participate in the survey. The project was approved by The University of Calgary Conjoint Health Research Ethics Board (REB21-0324), and all participants provided informed consent.
Data collection
Recruitment was done through national and international kidney organisation websites and social media platforms including Facebook and Twitter. The Kidney Foundation of Canada, British Columbia Renal Agency, Canadians Seeking Solutions and Innovations to Overcome; Chronic Kidney Disease (CanSOLVE CKD) Network, the Kidney Patient Involvement Network (KPIN) and GREX were used to disseminate the survey. In Alberta, Canada, recruitment was completed using posters at the Calgary PD unit and the Edmonton PD unit. We administered the survey online via REDCap (https://redcap.cru.ucalgary.ca) from July 2021 to May 2022. Surveys with identical free text responses and those which were not completed were excluded from analyses.
Statistical analysis
All variables were reported using simple frequency and descriptive techniques (e.g. frequency count, percentage, mean (standard deviation) and median (interquartile range)). We examined differences in key survey responses between men and women, and between North American and non-North American participants, using chi-square or Fisher’s exact tests as appropriate. Free text responses were collated and summarised in terms of emerging themes for reporting using inductive reasoning.
Results
Characteristics of respondents
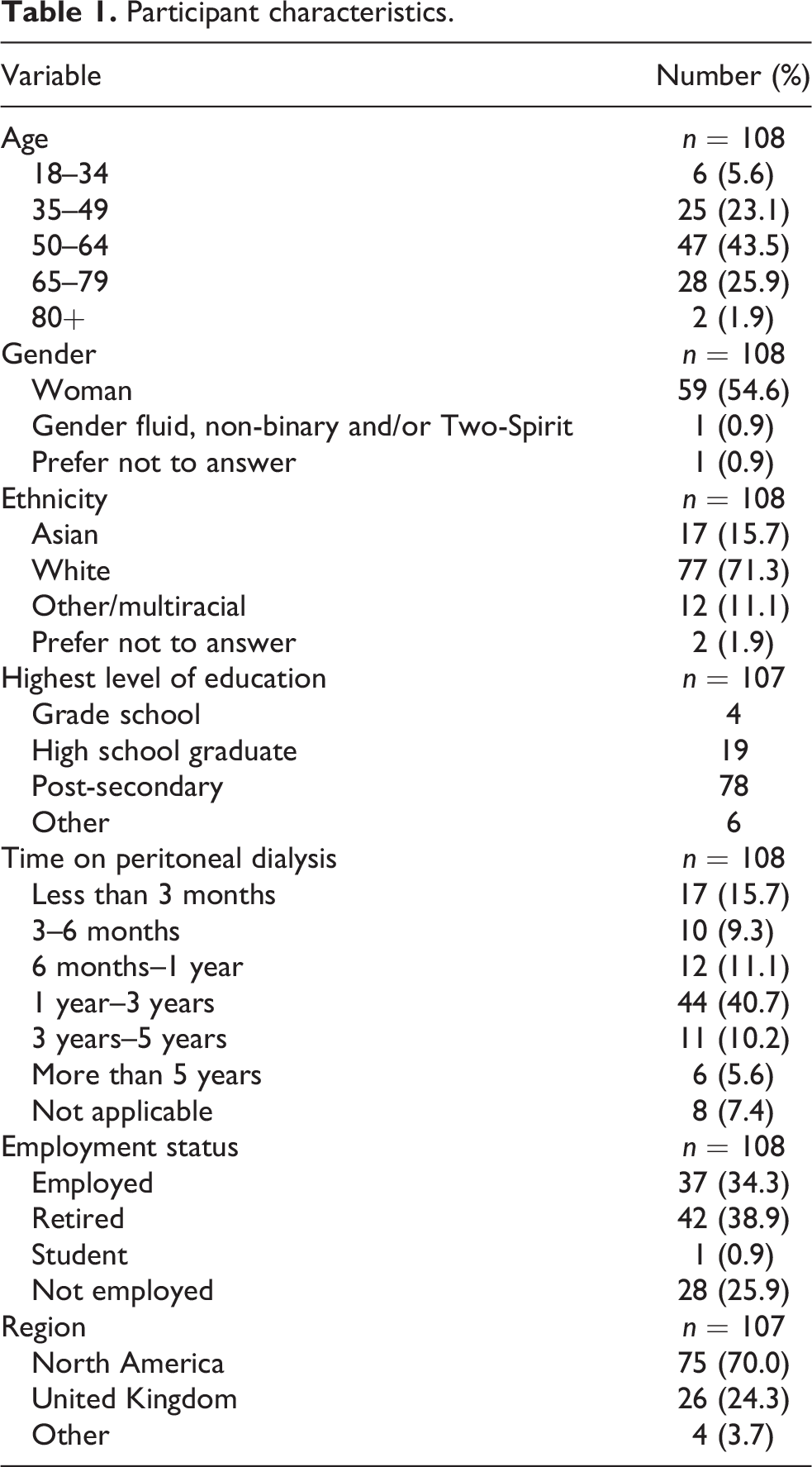
A total of 114 respondents answered the survey, and six surveys were excluded due to either incompletion (3) or duplication (3), leaving 108 respondents. The majority of the 108 respondents were from Canada (68%), followed by the United Kingdom (25%) and other (7%) (the United States, Australia, Taiwan and Mexico). Of the Canadian responses, 92% (67) were from Alberta, of which 66% (44) were from Northern Alberta and 34% (23) from Southern Alberta. Table 1 shows the respondent characteristics. The majority identified as women (55%) were 50–64 years old (43.5%), had received PD for 1–3 years (41%), completed post-secondary education (72.9%) and self-identified as white (71.3%).
Participant characteristics.
Respondent perceptions of physical activity
Table 2 describes perceptions regarding physical activity. Most respondents (91.8%) believed that physical activity is beneficial and 61.7% reported having previous discussions with their healthcare providers about physical activity. Among this subset, discussions regarding physical activity included type of activity they should engage in (70% of respondents), frequency (62%) as well as what types of activity to avoid (65%). Free text responses for the types of physical activity that were recommended included walking, resistance training, cycling/biking and stretching. Activities they were told to avoid included heavy lifting, swimming/water activities and abdominal exercises.
Perceptions of physical activity.
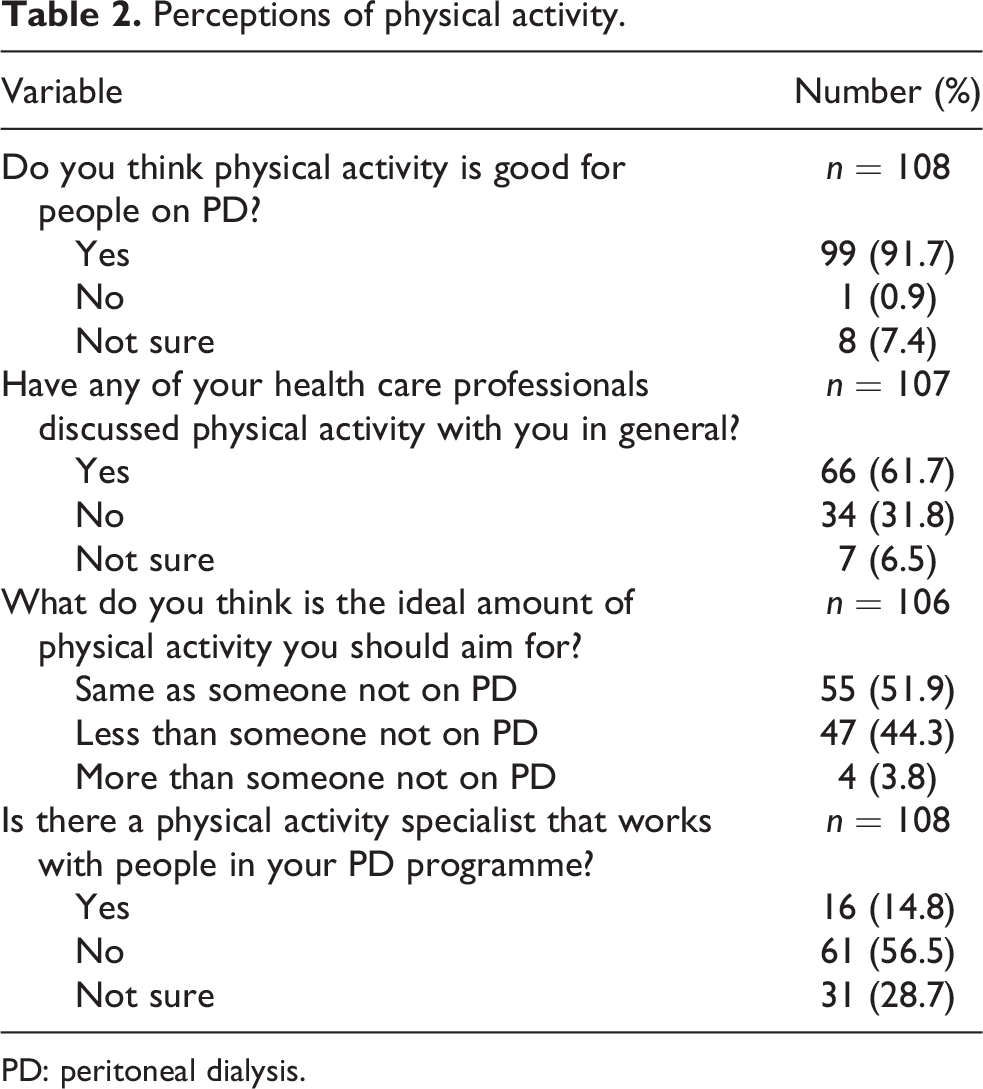
PD: peritoneal dialysis.
Equal numbers of respondents reported that they were told by their healthcare providers that they should (44%) and should not (44%) swim. Of the respondents who were told they should not swim, more than half stated that swimming was not recommended due to a heightened risk of potential infections. Among all respondents, 93% stated that they do not swim. Respondents who were given information about swimming received contradictory information about suitable locations. For example, some were told to never swim in oceans (5), lakes (3), pools (3) or hot tubs (3), while others were told they could swim in a pool (7) especially if it was the first thing in the morning or if they limited their swim to 30 min or less. Consistently, respondents reported that they had to seal the catheter site and keep it dry (10) while participating in water activities with no differences noted by region (data not shown).
Perceptions regarding weightlifting restrictions were also variable, with 76% of respondents indicating they were told not to lift a specific amount of weight, ranging anywhere from 2 kg to 45 kg. Few respondents reported receiving instructions about draining PD fluid prior to physical activity (28% yes, 53% no and 19% unsure). For those who were given advice regarding abdominal dialysate fluid, 74% reported the preference to have a dry or empty abdomen but stated that they should remain empty for only 1 h to a maximum of 2 h. We did not identify differences in exercise perceptions between men and women, nor between North American and non-North American respondents (Online Supplemental Table S1).
PD patients’ physical activity practices
Most respondents (71%) were engaged in physical activity two or more times per week (Figure 1) and had good exercise capacity (40.2% were not limited in their walking distance, Figure 2). Very few patients reported feeling unmotivated to carry out their daily activities in the previous week: 20.6% reported that they were rarely unmotivated (less than 1 day), 34.6% reported that some of the time (1–2 days) they were unmotivated, 26.2% reported occasionally (3–4 days) and 18.7% reported that most of the time (5–7 days) they were unmotivated to carry out their daily activities. Similarly, when asked how often they felt that everything they did was an effort in the past week, 23.4% responded that this happened rarely (less than 1 day), 32.7% some of the time (1–2 days), 20.6% occasionally (3–4 days) and 20.6% most of the time (5–7 days). Similar to exercise perceptions, we did not identify differences based on gender or geographic location (Online Supplementary Table S1).
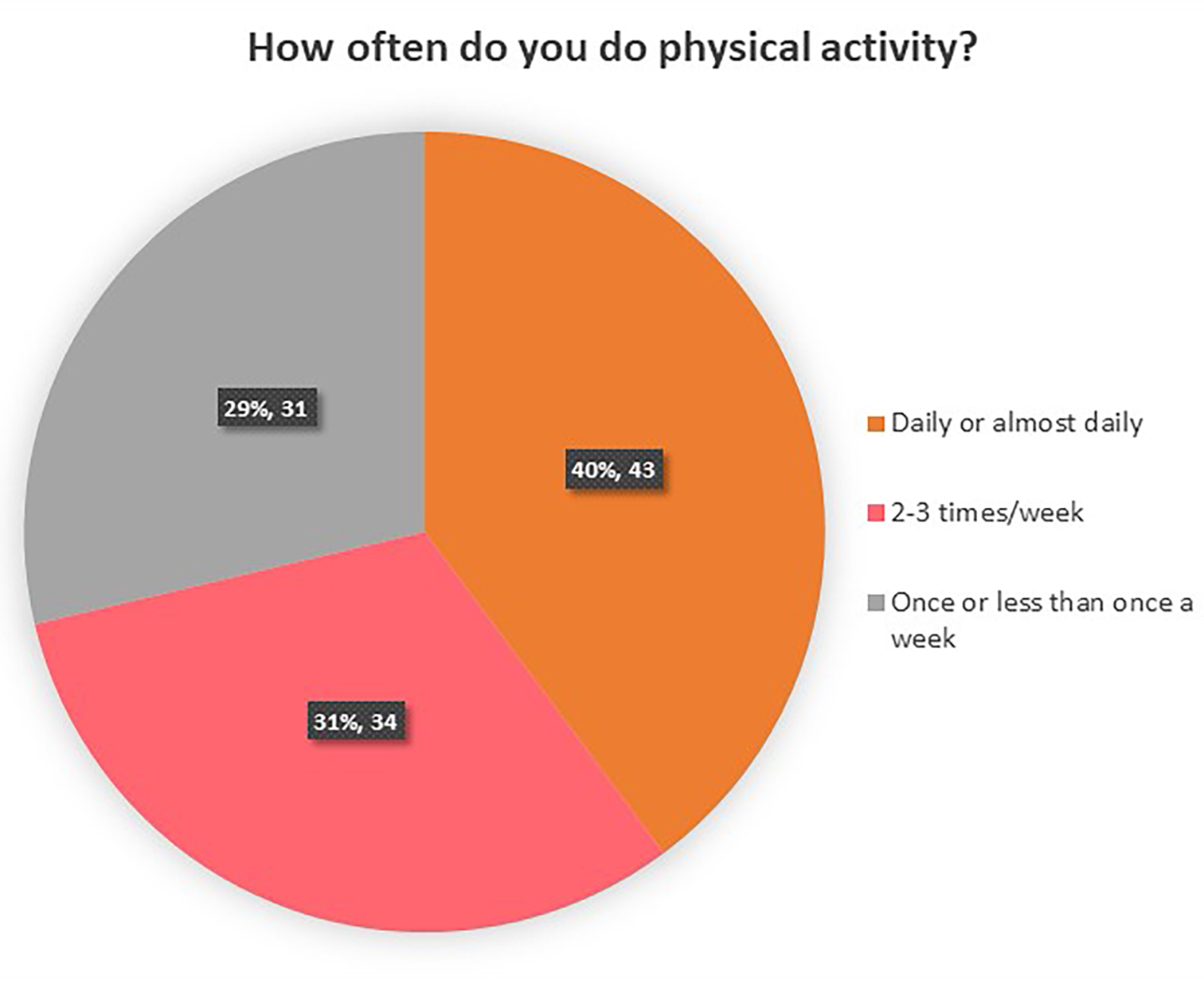
Frequency of physical activity.
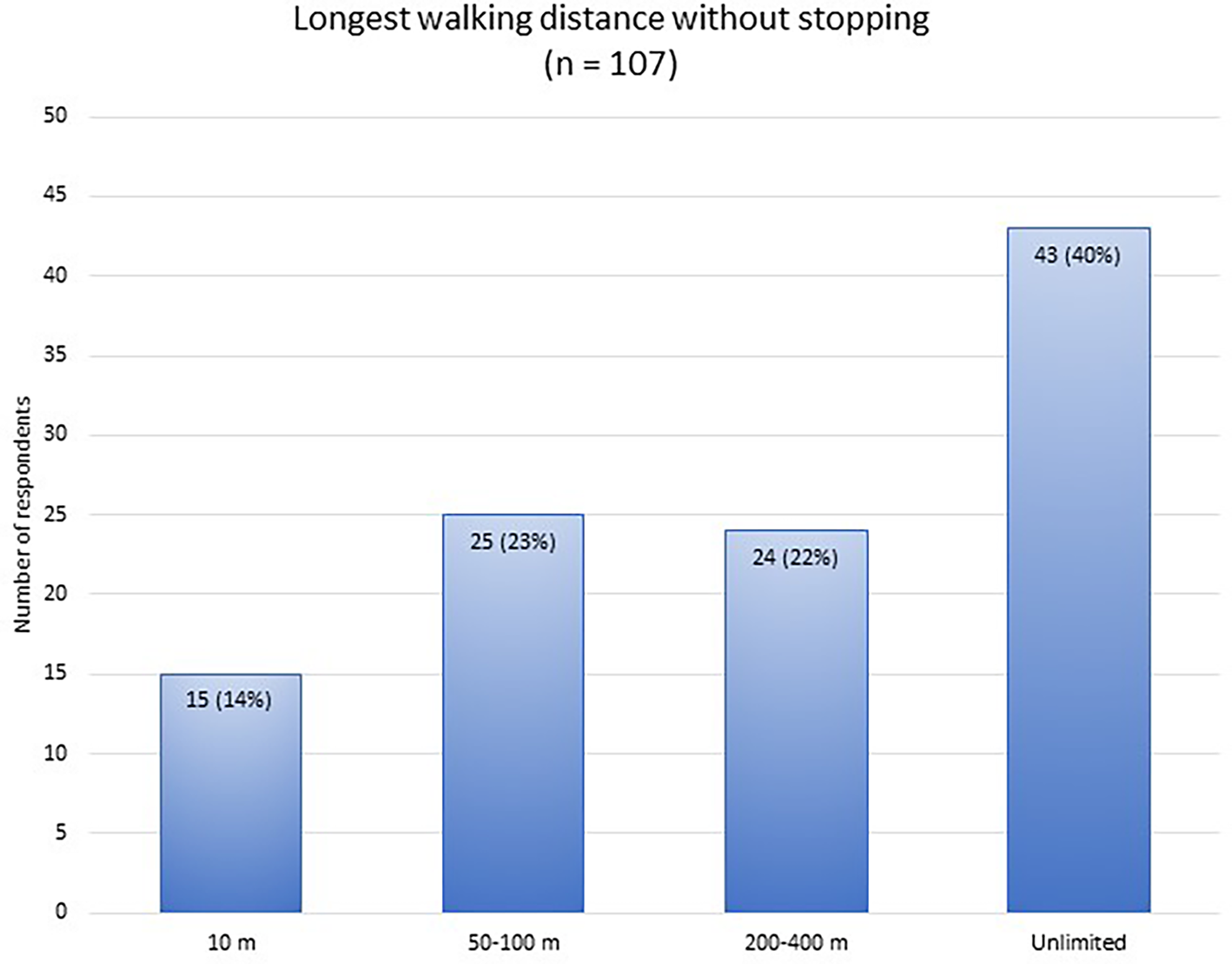
Exercise capacity.
Themes and respondents’ quotes
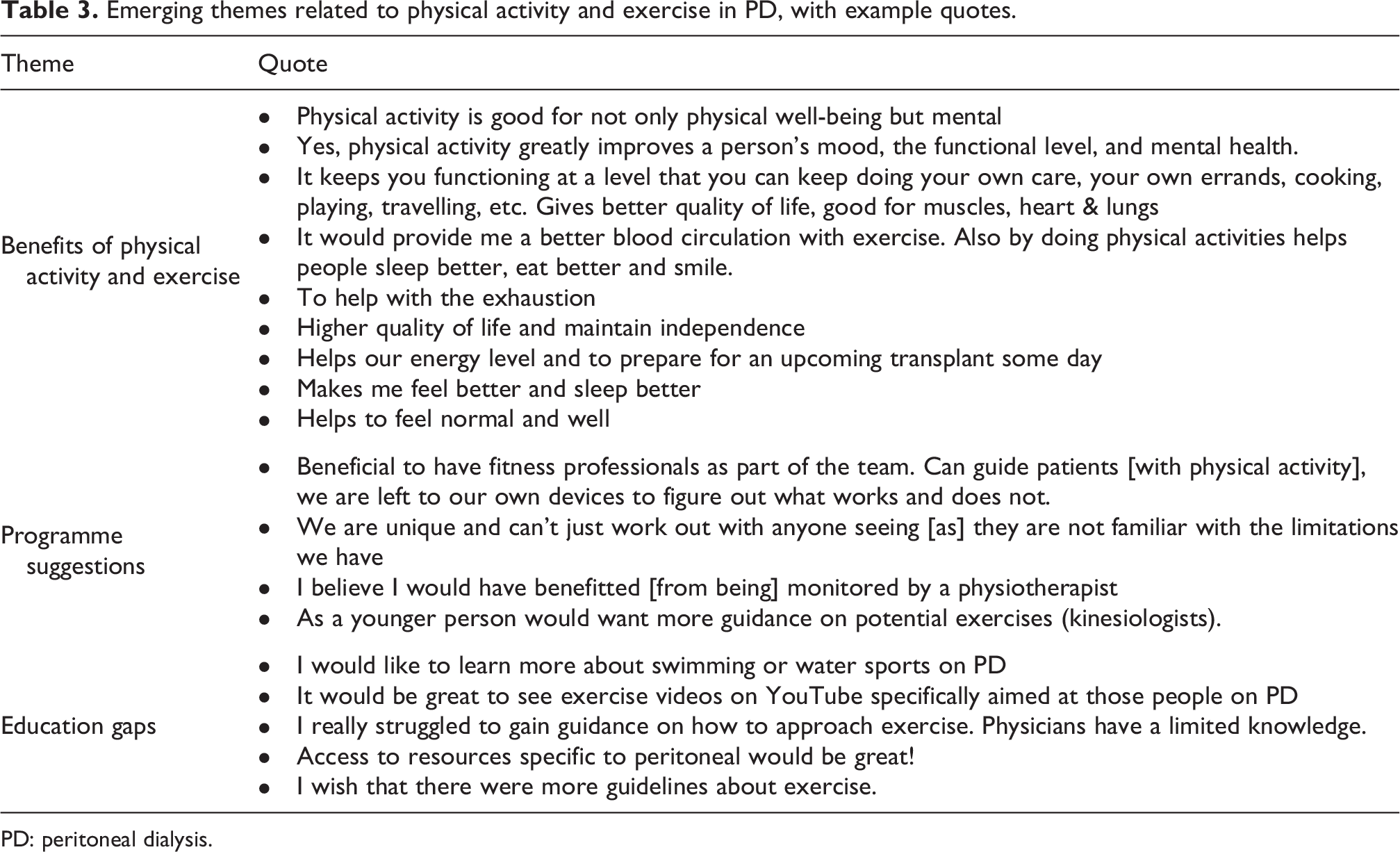
The text-based responses to questions revealed three dominant themes: the benefits of physical activity, programme requirements and gaps in education. Sample respondent quotes related to these themes are in Table 3. Most respondents were aware of the physical and mental health benefits of physical activity and exercise, with many reporting improved mood and resilience. In addition, respondents were aware that physical activity can help treat symptoms of kidney disease by improving energy levels, sleeping habits, quality of life and by reducing fatigue. Several respondents made comments regarding maintaining one’s health and optimising strength to prepare for a kidney transplant. Having access to exercise professionals who are knowledgeable about the unique requirements of PD was perceived to be a beneficial resource for physical activity guidance for people on PD. Several gaps in patient education were highlighted ranging from the need for access to resources specific to PD, information regarding swimming and lifting weights and the lack of healthcare provider awareness on exercise recommendations for people on PD.
Emerging themes related to physical activity and exercise in PD, with example quotes.
PD: peritoneal dialysis.
Discussion
In this cross-sectional survey, we elicited the physical activity perceptions and practices of people on PD. Our survey respondents were knowledgeable regarding the benefits of exercise and physical activity on physical and mental health for people receiving PD. The respondents were regularly physically active and had good physical function (40% were able to walk without stopping). Despite their awareness regarding the benefits of physical activity and exercise to improve the symptoms commonly associated with kidney disease, many misconceptions emerged which highlight the knowledge gaps regarding exercise practices for people receiving PD. Areas of conflicting advice include the maximum weight a person should lift, whether exercise is best performed with or without intrabdominal PD fluid in situ and whether swimming is allowed.
Unfortunately, there is no clear guidance on the maximal weight lifting restrictions, but recent International Society for Peritoneal Dialysis (ISPD) exercise recommendations 13 suggest that weightlifting should be done without intra-abdominal PD fluid to ensure the lowest levels intra-abdominal pressure. Less than 30% of respondents reported being given instructions regarding emptying their abdomen of PD fluid prior to and during exercise. The advice regarding recommendations for swimming from PD programmes is conflicting, with some programmes recommending swimming be avoided completely; however, ISPD recommends swimming in sea water or pools that are well maintained to minimise exposure to waterborne pathogens. The conflicting advice received demonstrates knowledge gaps among both healthcare providers and patients. Education regarding the practice of exercise for people living with PD is needed. An exercise and physical activity specialist could help with these gaps and inform providers and patients regarding safe exercise practices and exercise programmes. Unfortunately, only 14.8% of respondents reported having knowledge of the presence of a physical activity/exercise specialist working with their programme.
There have been three other survey studies exploring the perceived benefits and barriers of exercise amongst people on PD: a small Australian sample of mostly male (69%), age 65 ± 10.9 years, 12 a UK sample of 124 patients, mean age 62.1 ± 15.2 years, male 66% 14 and a Canadian study of 117 patients, age 64 ± 15 years, male 66%. 11 Similar to our findings, respondents had a positive attitude towards exercise and its effects on health despite the low rate of physical activity (14% physically active in the UK population and 40% walked a moderate to vigorous amount for the last 3 of 7 days in the study by Moorman et al. 11 ). Specific exercise practices and PD-related concerns were not investigated in these studies.
Based on previous studies which cited very low activity levels in dialysis patients, 14,15 we anticipated that the need for promotion of the benefits of physical activity in chronic disease would be highlighted by findings from our survey. However, the respondents in our survey were a physically active cohort who were aware of the benefits of activity including improving one’s physical and mental well-being as well as to help manage symptoms of kidney disease. Our findings revealed that more nuanced education and specific exercise recommendations for both healthcare providers and patients is needed. This Canadian-dominated survey reflects an active population amongst a nation with a high proportion of exercise programmes embedded within kidney care. Despite this, our study still revealed knowledge gaps regarding exercise practices for people receiving PD which is in part due to lack of evidence. Further research regarding the effects of weightlifting, core strengthening exercises and the safety of swimming is needed to provide patients with evidence-based recommendations rather than defaulting to restricting activity. Current recommendations from ISPD and GREX, 13 while based on low quality evidence, are a good starting point for clinicians and exercise specialists to ensure consistency of advice.
Limitations
The limitations of this survey include a small sample size with a population that is predominantly white and from Canada. The majority of respondents were from Alberta, likely leading to an underestimation of the variability in perception and practices which limited our ability to explore for regional differences. The survey was only offered in English and French languages thus limiting diverse representation. The small sample size limited our statistical power to fully explore gender and regional differences in exercise perceptions and practices. Another limitation was that convenience sampling and the web-based design likely contributed to selection bias with inclusion of people with positive attitudes towards physical activity and exercise. As with any survey, the responses may be limited by social desirability bias. Furthermore, this was an educated and motivated population where 40% reported daily exercise thus limiting the generalisability of the results. Given the limitations of this small non-diverse data set, the generalisability of the findings to the PD population at large need to be further evaluated in larger studies. Regardless, this is one of the largest global studies of the perceptions and practices related to physical activity among people receiving PD, and its findings provide insight into gaps in knowledge.
Conclusion
Our results revealed that although people receiving PD are aware of potential benefits of physical activity and exercise, conflicting advice is provided regarding weightlifting, swimming and the role of a dry or empty abdomen prior to exercise. There is a need for more educational resources including videos to enable people receiving PD to fully participate in physical activity and exercise. Future research exploring the impact of lifting heavy weights, the relationship between core strengthening exercise and risk of hernia formation and the risk of PD-related infections with water-related activities is needed to develop these educational materials. Until then, clinicians and exercise specialists are referred to the ISPD/GREX recommendations 13 to minimise variability in the advice given to people receiving PD. Future funding and research is needed to close the knowledge gaps highlighted in this study.
Supplemental Material
Supplemental Material, sj-docx-1-ptd-10.1177_08968608241237686 - Exercise perceptions and practices of people receiving peritoneal dialysis: An international cross-sectional survey
Supplemental Material, sj-docx-1-ptd-10.1177_08968608241237686 for Exercise perceptions and practices of people receiving peritoneal dialysis: An international cross-sectional survey by Jennifer M MacRae, Trinity A Tam, Tyrone Harrison, Oksana Harasemiw, Clara Bohm, Paul N Bennett, Nancy Verdin, Nicki Scholes-Robertson, Madeleine Warren and Stephanie Thompson in Peritoneal Dialysis International
Footnotes
Acknowledgement
None.
Author contributions
JMM: concept, design of the work, data analysis, first draft, revisions and approval; TAT: substantial contribution to manuscript drafts and final approval; TH: data analysis, interpretation and final approval; OH: design, data analysis and manuscript approval; PNB: design, analysis, draft revisions and approval; NV, MW and NSR: design and manuscript approval; ST design, analysis, manuscript preparations and final approval.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The views expressed are those of the author(s) and not necessarily those of the ISPD.
Ethical approval
The University of Calgary Conjoint Health Research Ethics Board; REB21-0324.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article presents independent research funded by the International Society for Peritoneal Dialysis (ISPD).
Informed consent to participate
Yes.
Informed consent to publish
Not applicable.
Supplementary material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.