
Abstract
Background:
Reduced kidney function and distorted kidney anatomy in patients with autosomal dominant polycystic kidney disease (ADPKD) may complicate stone interventions more compared with the general population.
Objectives:
To review studies describing the safety and efficacy of the 3 main stone interventions in adults with ADPKD: shock wave lithotripsy (SWL), ureteroscopy, and percutaneous nephrolithotomy (PCNL).
Design:
Systematic review.
Setting:
Any country of origin.
Patients:
Adults with ADPKD who underwent SWL, ureteroscopy, or PCNL.
Measurements:
Being stone free after the intervention and postoperative complications as reported by each study, which included pain, bleeding, and fever.
Methods:
Relevant studies published until February 2019 were identified through a comprehensive search of MEDLINE, EMBASE, Web of Science, BIOSIS PREVIEW, and CINAHL. Studies were eligible for review if they reported at least one outcome following SWL, ureteroscopy, and/or PCNL in adults with ADPKD. We then abstracted information on study characteristics, patient characteristics, intervention details, and postintervention outcomes and assessed the methodological quality of each study using a modified Downs and Black checklist.
Results:
We screened 221 citations from which we identified 24 studies that met our review criteria. We identified an additional article when manually reviewing the reference list of an included article, yielding a total of 25 studies describing 311 patients (32 SWL, 42 ureteroscopy, and 237 PCNL). The percentage of patients who were stone free after 1 session ranged from 0% to 69% after SWL, 73% to 100% after ureteroscopy, and 45% to 100% after PCNL. The percentage of patients with ADPKD that experienced at least one postoperative complication ranged from 0% to 33% for SWL, 0% to 27% for ureteroscopy, and 0% to 100% for PCNL.
Limitations:
The number and quality of studies published to date are limited.
Conclusions:
The efficacy and safety of stone interventions in patients with ADPKD remains uncertain, with wide-ranging estimates reported in the literature.
Trial Registration:
We did not register the protocol of this systematic review.
What was known before
The 3 most common interventions used to manage stones are shock wave lithotripsy, ureteroscopy, and percutaneous nephrolithotomy. These interventions may have differential efficacy and safety profiles when used in patients with autosomal dominant polycystic kidney disease (ADPKD) compared with the general population.
What this adds
This systematic review of 25 studies (311 patients in total) demonstrated estimates on the proportion of patients with autosomal dominant polycystic kidney disease (ADKPD) who were stone free after an intervention vary widely in the literature, as well as the proportion who experienced at least one postoperative complication. Many studies had methodological limitations. The results of this review confirm more rigorous studies are needed.
Introduction
Autosomal dominant polycystic kidney disease (ADPKD) is a genetic kidney disorder with no cure.1,2 It is characterized by focal cyst development leading to a progressive enlargement of both kidneys and kidney failure.3,4 The prevalence of stones in patients with ADPKD ranges from 3% to 59%.5 The wide range of kidney stone prevalence reported in the literature can be explained by several factors including inconsistent stone definitions, different distributions of stone risk factors, potential recall bias in studies that relied on patient self-reported data to identify stone events, and relying on past imaging reports for reasons other than stone identification. 5 Kidney stones in patients with ADPKD are associated with significant morbidity. For example, stones are a major determinant of pain and may accelerate chronic kidney disease progression.6,7 For these reasons, effective stone management is important in patients with ADPKD. However, the distorted kidneys and the reduced kidney function in patients with ADPKD may make active stone removal more challenging. For example, the cysts in patients with ADPKD may hinder optimal stone access and hence the success rate of stone interventions.
A published clinical practice guideline states that stone management in patients with ADPKD should not differ from the general population, and recommends that if necessary that stone interventions be considered. 8 The guideline authors also indicated that their recommendation was based on limited evidence.
Irrespective of whether a patient has ADPKD or not, urgent intervention is often required in the presence of infection/urosepsis, intractable pain, vomiting, impending acute renal failure, and/or obstruction. 9 Currently, shock wave lithotripsy (SWL), ureteroscopy, and percutaneous nephrolithotomy (PCNL) are commonly used procedures to remove stones. 8 The choice of stone intervention to treat stone is primarily dependent on stone characteristics such as stone location and size and availability of equipment. In some instances, a combination of interventions may be required to remove stones. Shock wave lithotripsy emits shock waves from an external device, which then propagate through the body and cause the stones to fragment.10,11 The fragmented stones then pass on their own in the subsequent weeks. Shock wave lithotripsy is least invasive stone intervention and is not recommended for pregnant women, and for patients with uncontrolled hypertension, uncontrolled coagulopathy, or a distal urinary obstruction to where stone is located. 12 Ureteroscopy is performed by inserting a rigid, semi-rigid, or flexible ureteroscope through the urethra and into the ureter and positioning it close to the stone.13,14 Instruments, such as laser, are used to fragment the stones, and these stone fragments can be left to pass or can be removed using instruments such as stone baskets or graspers. 15 During PCNL, a renal calyx is punctured percutaneously with fluoroscopy and/or ultrasound guidance to gain an access to the stone. 16 Stones are then fragmented using instruments, such as lasers or pneumatic lithotripters, and removed using tools such as graspers or suction devices. 9 Percutaneous nephrolithotomy is relatively the most invasive stone intervention. 9
We undertook this systematic review to critically appraise and summarize the results of studies which described the efficacy and safety outcomes of the 3 main stone interventions (SWL, ureteroscopy, and PCNL) in adults with ADPKD. The outcomes of interest were the proportion of patients who were stone free after the intervention and the proportion who experienced at least one postoperative complication.
Methods
Design and Study Selection
We conducted this systematic review using an internal prespecified protocol and reported this review according to the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) statement (Supplementary Table S1). 17
We included studies that met the following eligibility criteria: (1) published English language full-text articles and conference proceedings; (2) any study design; (3) at least 2 patients with ADPKD included in the study, (4) with and without a comparator group, and (5) described any efficacy or safety outcome following at least any one of SWL, ureteroscopy, and/or PCNL in adults with ADPKD and kidney stones. If multiple publications reported outcomes on similar group of patients, then we abstracted data on the study published more recently. We only included studies with comparators if outcomes of a stone intervention were compared between ADPKD and non-ADPKD populations who underwent the same stone intervention; we did not include studies if outcomes of 2 different interventions were compared in patients with ADPKD.
Identifying Relevant Articles
With an experienced librarian, we developed a comprehensive search strategy (Supplementary Table S2) to identify eligible published, original journal articles and conference proceedings on kidney stone interventions performed in adults with ADPKD. We retrieved all citations using MEDLINE (1947 to February 2019), EMBASE (1947 to February 2019), Web of Science, BIOSIS Preview (1955 to February 2019), and CINAHL.
Two reviewers (V.K. and R.J.) removed duplicates and rated the remaining title and abstracts obtained from the search syntax. We retrieved the full text of all “relevant” and “potentially relevant” articles to further assess study eligibility. To identify additional eligible articles, we also manually searched the reference list of all included articles, used the “cited by” function in Google Scholar and Web of Science, and the “similar article” feature of PubMed. The 2 reviewers resolved any disagreement by consensus.
Data Abstraction
One author (V.K.) developed a standardized form to abstract data from each study including information on study, patient and stone characteristics, interventions, and outcomes. Two authors (V.K. and R.J.) pilot-tested and improved the form by independently extracting data from 5 eligible articles. Using the final data abstraction form (see Supplementary Table S3), 2 abstractors independently extracted data from remaining studies, recorded the data, and resolved any disagreement by consensus.
Two authors (V.K. and G.G.) assessed the methodological quality of each of the included studies using a modified Downs and Black checklist (Supplementary Table S4). We assigned a score between 0 and 22 for all included studies, with a higher score indicating better methodological quality.
Data Analysis
Results were described qualitatively. The heterogeneity of included studies precluded a formal meta-analysis.
Results
Figure 1 summarizes the study selection process. Our search strategy yielded 221 citations that we reviewed and identified 24 eligible articles. We identified an additional article when manually searching the reference lists of the study conducted by Delakas et al. 18 This yielded a total of 25 relevant articles (311 patients with ADPKD) published between 1993 and 2019. Most studies were conducted in India (n = 7) followed by the United States (n = 6), China (n = 3), Greece (n = 2), and Kuwait (n = 2). One study was conducted in each of the following countries: Azerbaijan, Denmark, Iran, Romania, and Taiwan. Of the 25 included articles, 24 studies were case series (96%), and 1 (4%) was a cohort study. Sixteen (64%) of these were full-text journal articles, and 9 (36%) were conference proceedings.

Study selection.
The number of patients in each study ranged from 2 to 29 cases (2-30 kidneys), and the mean age of the patients ranged from 32 to 61 years. The stone interventions were performed between October 1981 and January 2017. It was unclear whether the interventions were emergent or elective in all included studies. The study and patient characteristics of each included study are summarized in Table 1, and overall outcomes of stone interventions are listed in Table 2.
Study and Patient Characteristics of Included Studies.

Note. NR = not reported; ADPKD = autosomal dominant polycystic kidney disease; SD = standard deviation.
A modified Downs and Black checklist was used to assess the methodological quality of each included study. The methods quality score ranged between 0 and 22 with higher scores indicating higher quality.
The described cases are a subset of a larger case series.
The reported length of follow-up is not the average but rather constant for all included patients.
Outcomes of Stone Interventions.

Note. NR = not reported; ADPKD = autosomal dominant polycystic kidney disease; SD = standard deviations.
Quality Assessment of Studies
The methods quality score was highly variable and ranged between 4 and 12 out of 22 (where higher scores indicates studies of higher methodological quality).
The ADPKD and outcome definitions affect the internal validity of a study. Only 1 study reported the case definition of ADPKD, which defined ADPKD using the validated, Ravine ultrasonographic criteria.34,41
Definition for stone-free status post-intervention was highly variable across studies. Seven of the 25 studies specified and defined stone-free status as complete clearance or residual fragments less than a prespecified size. The prespecified size for an acceptable residual fragment was less than 4 mm for 5 studies, less than 2 mm for 1 study, and less than 1 mm for 1 study.
The sampling strategy and the source population influenced the generalizability of the findings to the broader ADPKD population who underwent stone intervention. Seven of the 25 studies specified how cases were recruited, and all 7 studies included consecutive or all patients within a specified time frame.13,14,23,27,33,35,38 One study recruited patients from an outpatient setting, 21 and 4 studies recruited patients from a hospital setting.18,25,34,40 For the latter, it was unclear whether the cases were recruited from a same day surgery setting, emergency department, inpatient, or an outpatient hospital-based clinic.
One conference proceeding described the efficacy outcomes of PCNL performed in patients with ADPKD compared with non-ADPKD controls, without adjustment for any covariates. 26
Shock Wave Lithotripsy
We identified 7 case series describing the outcomes and experience of treating stones in patients with ADPKD with SWL (in total, 32 patients).14,18,19,20,21,22,23 The characteristics of SWL for each study are summarized in Table 3.
Characteristics of Shock Wave Lithotripsy (SWL).

Note. SD = standard deviation; kV = kilovolts; U/S = ultrasound; KUB = kidney, ureter, bladder; NR = not reported; CT = computed tomography.
None to 69% of the patients were stone free after a single SWL session, and 15% to 67% of the patients received additional follow-up procedures to achieve stone-free status.14,18,19,20,21,22,23 In 4 of the 6 case series that examined at least one postoperative SWL complication, no patients experienced any complications postoperatively.21,19,20,22 The percentage of patients that experienced at least one complication was unclear in 1 study, 18 and 33% of the patients described by Singh et al 23 experienced fever postoperatively. The reported postoperative complications of SWL in patients with ADPKD included colic pain and fever.18,23 Delakas and colleagues 18 specified that none of the patients experienced any intraoperative complications, whereas the remaining 6 case series did not report any intraoperative complications.14,19,20,21,22,23
Ureteroscopy
We identified 6 case series reporting stone treatment in patients with ADPKD using ureteroscopy (in total, 42 patients).13,14,22,23,24,25 The characteristics of ureteroscopy are detailed in Table 4.
Characteristics of Ureteroscopy.

Note. NR = not reported; U/S = ultrasound; KUB = kidney, ureter, bladder; CT = computed tomography.
After a single session, 73% to 100% of the patients were stone free.13,24,25 In 4 case series, no patients required a second procedure to facilitate complete stone removal,14,22,23,24 whereas another case series reported 15% undergoing a second ureteroscopy 1 week following the first procedure. 13 The percentage of patients that underwent a second procedure was unclear or not reported in 1 case series. 25 Three case series reported that none of the patients experienced any postoperative complications.14,22,24 About 20% to 27% of the patients experienced at least one postoperative complication, such as fever, hematuria, and pain in the remaining 3 case series.13,23,25 One case series reported that not a single patient experienced any intraoperative outcomes during ureteroscopy, 13 whereas the remaining 5 case series did not report about any intraoperative outcomes.14,22,23,24,25
Percutaneous Nephrolithotomy
Sixteen case series 14,23,27,28-40 and 1 cohort study 26 reported the use of PCNL for stone removal in adults with ADPKD, with 3 to 29 patients per series (3 to 30 kidneys) (in total, 237 patients). Percutaneous nephrolithotomy–specific characteristics of each study are detailed in Table 5.
Characteristics of Percutaneous Nephrolithotomy (PCNL).
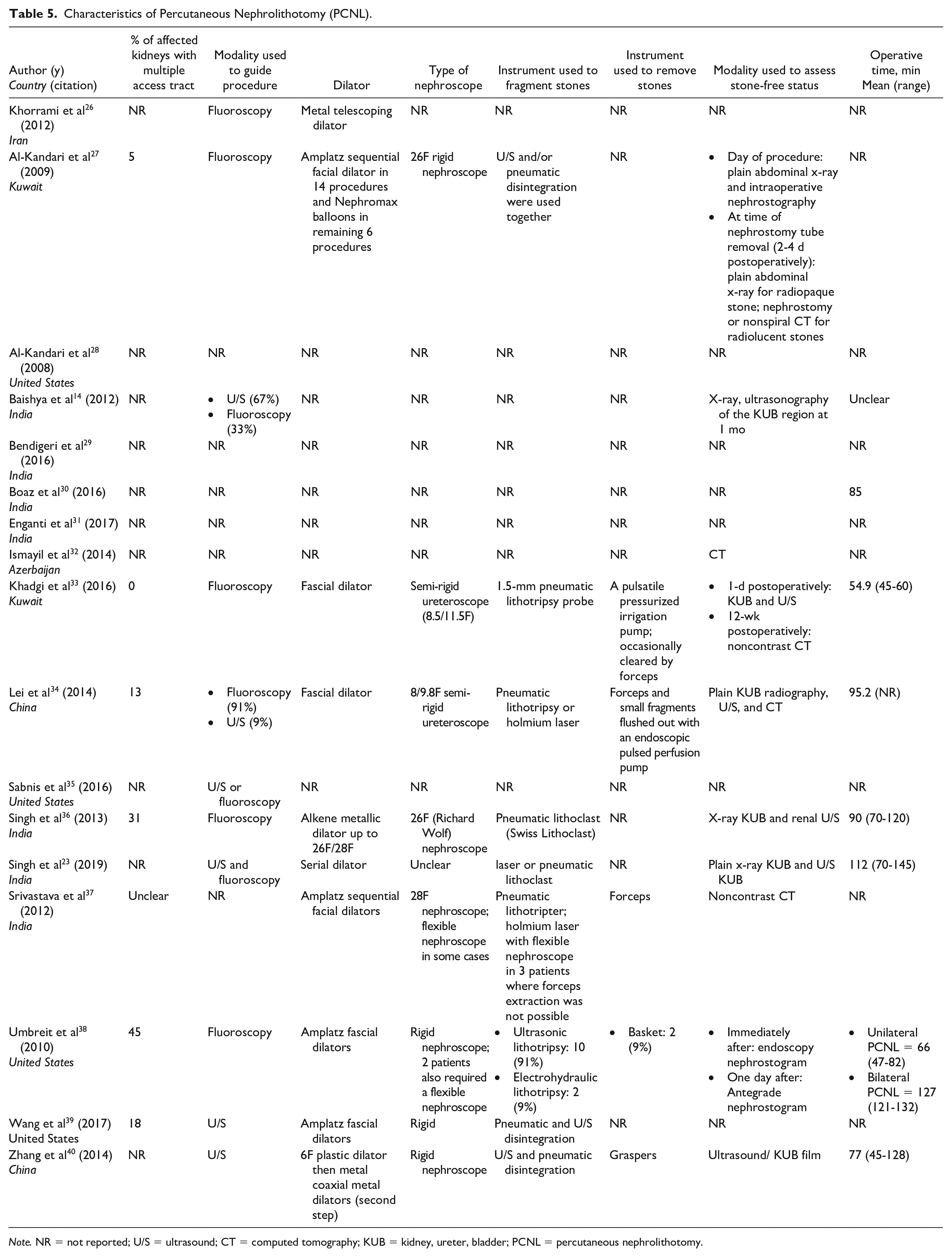
Note. NR = not reported; U/S = ultrasound; CT = computed tomography; KUB = kidney, ureter, bladder; PCNL = percutaneous nephrolithotomy.
The stone-free status of patients after a single session ranged from 45% to 100%, and 0% to 64% of the patients required a follow-up procedure for residual stones among the 12 studies that reported it.14,27,28-30,32-40 Two studies reported no patients experienced any postoperative complications,38,28 7 case series did not report the percentage of patients with complications,23,29,34,36,37,39,40 and 15% to 100% of patients experienced at least one complication among the remaining 7 case series.14,23,27,30-33 The postoperative complications of PCNL included fever, pain, hematuria, bleeding, urinary tract infection, cyst infection, perirenal hematoma collection, hydrothorax, hemothorax, pneumothorax, paralytic ileus, worsening of preexisting renal failure, blood transfusion, renal pelvic perforation, urinary leakage from nephrostomy tube, and sepsis.14,23,27,29-37,39,40 None of the patients described by Umbreit et al 38 experienced any intraoperative complications. In 3 other case series, at least one patient experienced an intraoperative complication, including bleeding, renal pelvic tear, and hypotension28,30,36; the remaining studies did not clearly report any intraoperative complications.14,23,27,29,31-35,37,39,40
Khorrami et al 26 conducted a cohort study of patients undergoing PCNL, comparing 8 patients with ADPKD to 100 patients without ADPKD. There were no significant between-group differences in stone-free status, the rise in the concentration of serum creatinine after the procedure, or the decline in concentration of hemoglobin after the procedure. 26 However, urinary leakage lasted significantly longer in patients with ADPKD compared with patients without ADPKD. 26
Discussion
We conducted a systematic review of 25 studies describing at least one postoperative outcome of SWL, ureteroscopy, and PCNL in patients with ADPKD to summarize the literature and to identify knowledge gaps. The estimates are limited by small sample sizes and between-study variability in patient characteristics, stone characteristics, and treatment protocol. This concern notwithstanding, based on the literature published to date, the percentage of patients who were stone free after 1 session ranged from none to 69% for SWL, 73% to 100% for ureteroscopy, and 45% to 100% for PCNL. The overall complication rate ranged from none to 33% for SWL, none to 27% for ureteroscopy, and none to 100% for PCNL. Postoperative complications experienced by patients with ADPKD after any intervention included residual stones, pain, and fever. Postoperative hematuria was observed after ureteroscopy and PCNL. Other PCNL complications included urinary leakage, bleeding, renal pelvic perforation, perirenal fluid collection, urinary tract infection, cyst infection, worsening renal failure, hydrothorax, hemothorax, pneumothorax, and paralytic ileus.
The postoperative complication and stone-free rates of all 3 stone interventions were highly variable. The variability in postoperative complication and stone-free rates can be explained by between-study variability in the definitions used for stone-free status, sample size, treatment protocol, timing when imaging was performed postintervention, and the type of imaging performed to assess stone-free status postintervention. For example, among all imaging modalities used to assess stone-free status, computed tomography (CT) is the most sensitive modality to detect residual stones.42,43 Ultrasound and kidney, ureter, and bladder (KUB) radiograph cannot detect radiolucent stones, such as uric acid stones, and the ultrasound performance is poor for patients who are obese and patients with residual fragments less than 5 mm42,43 and would be expected to be less sensitive in the setting of ADPKD. As a result, studies that use CT postoperatively would report a lower stone-free rate compared with studies that use ultrasound or KUB. Patient and stone characteristics, including ADPKD-specific characteristics such as residual renal function and cyst volume and location, influence intervention choice and subsequent success and complication rates. In general, symptomatic stones that are between 1 and 2 cm would be treated with either SWL or ureteroscopy, and PCNL would be reserved for stones greater than 2 cm, or in patients where retrograde access is not possible. The success rate of all 3 interventions is dependent on gaining optimal access to stones. 44 Therefore, variability in patient and stone characteristics across studies also explain the variability in reported success and complication rate.
It is difficult to determine whether SWL, ureteroscopy, and PCNL are truly efficacious and safe in patients with ADPKD because the variability described above also limits indirect comparison of stone interventions success and complication rates between that reported in patients with ADPKD and the general population. Furthermore, the ADPKD cases described in the studies were likely more selected than the general population because of their complex kidney anatomy. Future randomized controlled trials or observational studies that use a representative sample of patients with ADPKD and address potential confounding factors are required to elucidate whether ADPKD is truly associated with poor outcomes following SWL, ureteroscopy, and PCNL.
Our findings must be interpreted with caution due to several limitations. First, except for 1 cohort study, all studies were clinical case series. Although case series give some insight into the outcomes of stone interventions and are useful for generating new hypotheses, the observations are not necessarily generalizable to the broader ADPKD population. Based on our systematic, comprehensive search, the conference proceeding published by Khorrami et al (2012) is the only cohort study in the literature. 36 Although they compared the outcomes of PCNL in patients with ADPKD to patients without ADPKD, they did not adjust for any covariates. Second, the sample size of all included studies, including the cohort study, was small so the reported estimates were imprecise. Third, most of the data were retrospectively collected. As a result, the conclusions were highly dependent on the accuracy of medical records. The retrospective and unsystematic approach to data collection may also have introduced attrition bias. 45 Attrition bias is when patient’s prognosis affects their follow-up; patients with a less favorable outcome will more likely return for follow-up visits. As a result, the interventions may misleadingly appear less safe and efficacious in this group of patients. Fourth, the inclusion and exclusion criteria were not explicitly reported in all identified studies. Finally, all studies published to date did not describe the cystic volume in patients with ADPKD. As a result, it was difficult to elucidate whether and how cystic volume influences postoperative complication and success rates.
Aside from inherent limitations of the information in the primary studies, with respect to the quality of this review, we used a very comprehensive search strategy to identify relevant literature. Data were carefully abstracted using a robust form. Our study is the first systematic review to summarize the outcomes of stone interventions in adults with ADKPD.
Conclusions
Our systematic review shows that empirical evidence on the efficacy and safety of SWL, ureteroscopy, and PCNL in ADPKD is limited. Our findings corroborate Mallett et al’s suggestion to undertake methodologically rigorous studies to understand the consequences of these procedures in patients with ADPKD. 8
Supplemental Material
SUPPLEMENTARY_MATERIALS_1 – Supplemental material for Efficacy and Safety of Surgical Kidney Stone Interventions in Autosomal Dominant Polycystic Kidney Disease: A Systematic Review
Supplemental material, SUPPLEMENTARY_MATERIALS_1 for Efficacy and Safety of Surgical Kidney Stone Interventions in Autosomal Dominant Polycystic Kidney Disease: A Systematic Review by Vinusha Kalatharan, Racquel Jandoc, Gary Grewal, Danielle M. Nash, Blayne Welk, Sisira Sarma, York Pei and Amit X. Garg in Canadian Journal of Kidney Health and Disease
Footnotes
Acknowledgements
We thank our librarian, John Costello, for reviewing the search strategy.
Ethics Approval and Consent to Participate
Since this systematic review did not involve human investigation, ethics approval was not required.
Consent for Publication
Not Applicable.
Availability of Data and Materials
All data are presented in the original article.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Y.P. served as an expert consultant on drug development (Otsuka, Pfizer, and Genzyme/Sanofi) related to autosomal dominant polycystic kidney disease.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The ICES Kidney, Dialysis, and Transplantation Program provided funding for this study. V.K.’s training was supported by the Canadian Institutes of Health Research Doctoral Scholarship and the Doctoral Scholarship from the KRESCENT Program (a national kidney research training partnership of the Kidney Foundation of Canada, the Canadian Society of Nephrology, and the Canadian Institutes of Health Research). A.X.G. was supported by the Dr. Adam Linton Chair in Kidney Health Analytics and a Clinician Investigator Award from the Canadian Institutes of Health Research.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.