
Abstract
Background:
Ureteroscopy is a minimally invasive treatment option for upper tract stones. The distorted kidney anatomy in patients with autosomal dominant polycystic kidney disease (ADPKD) may place them at higher risk for ureteroscopic complications.
Objective:
To compare the 30-day risk of ureteroscopic complications between patients with and without ADPKD.
Design:
Retrospective cohort study.
Setting:
Ontario, Canada
Patients:
Seventy three patients with ADPKD and 81 445 patients without ADPKD who underwent ureteroscopy for upper urinary tract stones between April 1, 2002, and March 1, 2018.
Measurements:
A 30-day risk of (1) hospital presentation with ureteroscopic complications (which was a composite outcome of either emergency department visit or hospital admission with acute kidney injury, urinary tract infection, or sepsis); (2) all-cause hospital presentation; (3) all-cause hospital admission; and (4) all-cause emergency department visit.
Methods:
We regressed outcomes on demographic variables, health care use in the prior 1-year, various procedures and comorbidities related to the outcome in the prior 5 years, and prescribed medications filled in the past 120 days using modified Poisson regression to compare the risk ratio (RR) of each outcome between patients with and without ADPKD.
Results:
The median (interquartile, IQR) age was 44 (38-60 years) in the ADPKD group and 53 (42-64) in the control group. About 40% were women in both groups. The risk of ureteroscopic complications was not significantly different in patients with versus without ADPKD (8.2% vs 4.3%; adjusted RR = 1.5, 95% confidence interval [CI] = 0.7-3.2). Patients with versus without ADPKD were more likely to present to hospital after their procedure (35.6% vs. 20.0%; adjusted RR = 1.6, 95% CI = 1.2-2.2), which included a statistically significant increase in the risk of presenting to the emergency department (32.9% vs. 19.0%; adjusted RR = 1.6, 95% CI = 1.1-2.2) but not hospital admissions (10.9% vs. 5.0%; adjusted RR = 1.8, 95% CI = 0.9-3.4).
Limitations:
The low numbers of events led to imprecision around the estimates.
Conclusion:
Patients with ADPKD have a higher risk of return to the hospital within 30 days of ureteroscopy for stone disease.
Trial registration:
We did not register this study.
What was known before
The distorted kidney anatomy in patients with autosomal dominant polycystic kidney disease (ADPKD) may make performing ureteroscopy challenging. Efficacy and safety of ureteroscopy in patients with ADPKD remains uncertain, with wide-ranging estimates of postoperative outcome and the percentage of patients stone free after ureteroscopy reported in the literature.
What this adds
Patients with ADPKD experienced an increased risk of return to hospital within 30 days following ureteroscopy compared to patients without ADPKD.
Introduction
Autosomal dominant polycystic kidney disease (ADPKD) is a genetic kidney disorder with no cure.1,2 It is characterized by focal cyst development which leads to progressive enlargement of both kidneys, and eventual kidney function loss.3-5 Much of the current research on patients with ADPKD is focused on delaying time to the onset of end-stage kidney disease (ESKD). However, ADPKD is a systemic disorder with other morbidities that warrant attention to prevent loss of health-related quality of life. 6 One such morbidity is upper tract stones. 7 Stones in patients with ADPKD are a significant determinant of pain and may be associated with a higher risk of ESKD.7,8 Currently, there is limited evidence on how best to manage upper urinary tract stones in patients with ADPKD.
In the general population, stones less than four millimeter in size usually do not require a surgical intervention, and will often pass within four weeks of symptom onset. 9 Pain may be managed with narcotics or nonsteroidal anti-inflammatory drugs (NSAIDs). 9 However, urgent intervention is often required in the presence of infection/urosepsis, intractable pain, vomiting, impending acute renal failure, and/or significant obstruction. 10 Currently, shockwave lithotripsy (SWL), ureteroscopy, and percutaneous nephrolithotomy (PCNL) are potential treatment options; however, ureteroscopy is the most common intervention used in both patients with and without ADPKD. 11
A comprehensive systematic review conducted by our team confirms there is limited information on the risk of ureteroscopic complications in patients with ADPKD. 12 All studies were either clinical case series or reports, and most studies reported data from a single center. Overall, these limitations lead to uncertainty in how to counsel patients with ADPKD on expected postoperative ureteroscopic complications. In this study, we described the 30-day cumulative incidence of selected ureteroscopic complications, all-cause hospital presentation, all-cause hospital admission, and all-cause emergency department visits following ureteroscopy in patients with compared to patients without ADPKD.
Methods
Design and Setting
We conducted a retrospective cohort study using linked health care administrative databases held at ICES (a not-for-profit research institute). Health care services in Ontario are funded through the Ontario Health Insurance Plan (OHIP) program, with the exception of outpatient medications, which are only funded for segments of the population, including all people 65 years of age and older. These health care encounters are recorded in administrative databases, which are linked using unique, encoded identifiers and held at ICES. We reported this study following guidelines set up for studies conducted using routinely collected observational data (Supplementary Material Table S1).
Data Sources
We created the study cohorts, described baseline characteristics, defined the exposure, and ascertained outcomes using administrative codes detailed in Supplementary Table S2. A total of 7 databases were used: the Canadian Institute for Health Information (CIHI) Discharge Abstract Database (DAD), Same Day Surgery (SDS), and the National Ambulatory Care Reporting System (NACRS) databases contain diagnostic and clinical information on hospital admissions, same day surgery, and all emergency department visits in Ontario, respectively. The OHIP database captures physician-billing claims for all hospital and outpatient services for patients covered under OHIP. The Registered Persons Database (RPDB) includes reliable demographic and vital information. Canadian Organ Replacement Register (CORR) contains information on all maintenance dialysis and kidney transplant patients. Ontario Drug Benefit (ODB) database contains information on all dispensed outpatient prescriptions for Ontarians with a valid health card and who are aged 65 years and older, resident of long-term care facilities, receiving services under the Home Care program, Trillium Drug Program recipient, receiving social assistance, or under the Special Drugs program. The Ontario Laboratories Information System (OLIS) contains most of Ontario’s laboratory test results. All variables were complete, except for neighborhood income quintile (missing in 0.2%) and rural residency status (missing in 0.1%); we imputed the middle neighborhood income quintile and urban residence for missing values, respectively.
Population and Timeline
We identified all patients who underwent ureteroscopy between April 1, 2002, and March 31, 2018, using OHIP and Canadian Classification of Health Intervention (CCI) codes. OHIP billing codes are submitted by physicians to obtain payment for the interventions/procedures they perform. The OHIP billing codes for ureteroscopy and stone treatment have been extensively used in prior studies and are expected to have excellent validity similar to other fee-for-service codes.13-15 CCI is a health-related intervention classification system developed by the Canadian Institute for Health Information for administrative purposes. We excluded the following patients: (1) missing or invalid encrypted unique patient identifier, date of birth, sex, or date of death, (2) visiting non-Ontarians who received care from a health care facility in Ontario; (3) patients aged 18 and below to exclude patients with autosomal recessive polycystic kidney disease who may have been misclassified as patients with ADPKD; (4) patients with database codes for open stone surgery, SWL, and PCNL in the previous 90 days to try and ensure that ureteroscopy was the first stone intervention performed for the stone; and (5) kidney transplant recipients to ensure the ureteroscopy was performed for stones in the polycystic kidneys. Any stone intervention codes that appeared within 90 days of each other were considered interventions performed for the same stone.
The cohort entry date, to reflect the time of the ureteroscopic procedure, was either the hospital discharge date (for patients who underwent ureteroscopy in a hospital), registration date (for patients who underwent ureteroscopy at the time of an emergency department visit), or the date of the ureteroscopy (for patients who had the procedure performed in an outpatient setting). We looked back from cohort entry date until April 1, 2002, (earliest date when could identify patients with ADPKD using our administrative databases) for International Classification of Diseases, 10th Revision (ICD-10) codes related to ADPKD and classified patients as having or not having ADPKD. 16 ICD-10 codes related to ADPKD in our province have a positive predictive value of 85% (95% confidence interval [CI]: 79% to 89%), only identify patients who presented at the hospital with ADPKD, and differentiate patients with ADPKD from patients with other cystic kidney diseases.16,17 After classifying each patient as affected or not affected with ADPKD, we excluded patients with OHIP diagnosis codes for congenital anomalies of the urinary system (753) and other renal cystic disease (593) from the patients without ADPKD cohort only; although these OHIP diagnosis codes identify a lot of patients with ADPKD, the codes also indiscriminately capture the vast majority of patients with similar conditions. 17 Therefore, excluding patients with OHIP diagnosis codes 753 and 593 would ensure that there are no patients with ADPKD in the control group. We also excluded patients with baseline characteristics that were present in one group but not the other (see Supplementary Material Tables S3). For patients who underwent more than one ureteroscopy, we included only the first ureteroscopy event. We followed each patient for 30 days from cohort entry date to ascertain outcomes.
Outcomes
Outcomes assessed in the 30 days following ureteroscopy were hospital presentation with ureteroscopic complications (which was a composite outcome of either emergency department visit or hospital admission with acute kidney injury [AKI], urinary tract infection [UTI], or sepsis), all-cause hospital presentation (which was either emergency department visit or hospital admission for any reason), all-cause hospital admission, and all-cause emergency department visit. We identified hospital presentation with AKI, UTI, and sepsis using ICD-10 codes.18-20
Analysis
We assessed the baseline characteristics of both cohorts using medians and interquartile ranges (IQRs) for continuous variables, and frequencies and percentages for categorical variables. We used standardized differences to compare the baseline characteristics between patients with and without ADPKD. A standardized difference greater than 10% indicates important imbalance.
We estimated the unadjusted and adjusted risk ratios of outcomes and their associated 95% CIs using modified Poisson regression with a robust variance estimator and risk difference of outcomes and its respective 95% CIs using binomial regression. 21 We adjusted for the following covariates for all the models: ADPKD, date of cohort entry, age, sex, rural residency status, income quintile, local health integration network (LHIN), health care encounter in the prior 1 year (hospital admission, emergency department visit, primary-care physician visit, and intensive care unit visit), comorbid conditions in prior 5 years (acute interstitial nephritis, AKI, anemia, atrial fibrillation, chronic liver disease, chronic lung disease, coronary artery disease, depression, diabetes mellitus, hemorrhage, hypertension, kidney tumor, obesity, prostatic hyperplasia, UTI, and urinary tract obstruction), procedures performed in the prior 5 years (cystoscopy, percutaneous stent, and surgery), prescription filled in the prior 120 days (angiotensin-converting enzyme inhibitor or angiotensin receptor blockers, and proton pump inhibitors), and estimated glomerular filtration rate value greater than or less than 60 mL/min/1.73 m² or missing.
We considered and assessed for multicollinearity using variance inflation factor (a variance inflation factor of >2 indicates presence of multicollinearity) between the covariates listed above. The variance inflation factor was greater than 2 for proton pump inhibitors, diuretics, antidiabetic medication, antibiotics, and calcium channel blockers. After omitting the latter 4 variables, the variance inflation factor was less than 2 for all remaining covariates in the adjusted model.
As a post-hoc analysis, we examined the most common reasoning for presenting to the emergency department and median IQR time to the outcomes for both patients with and without ADPKD. All statistical analyses were performed using SAS 9.4 (SAS Institute, Inc, Cary, NC), and 2-tailed p values less than .05 were interpreted as statistically significant.
Results
Cohort Selection and Baseline Characteristics
Our cohort included 73 patients with ADPKD, and 81 445 patients without ADPKD who underwent ureteroscopy (Figure 1). Ureteroscopy was performed across 40 unique institutions for patients with ADPKD, and across 228 unique institutions for patients without ADPKD. The characteristics of both groups are summarized in Table 1. Compared to patients without ADPKD, patients with ADPKD were younger (median age 44 vs. 53 years), and equally likely to come from a rural area (12.3% vs. 12.1%). About 39.7% of the patients with ADPKD, and 38.7% of the patients without ADPKD were women.
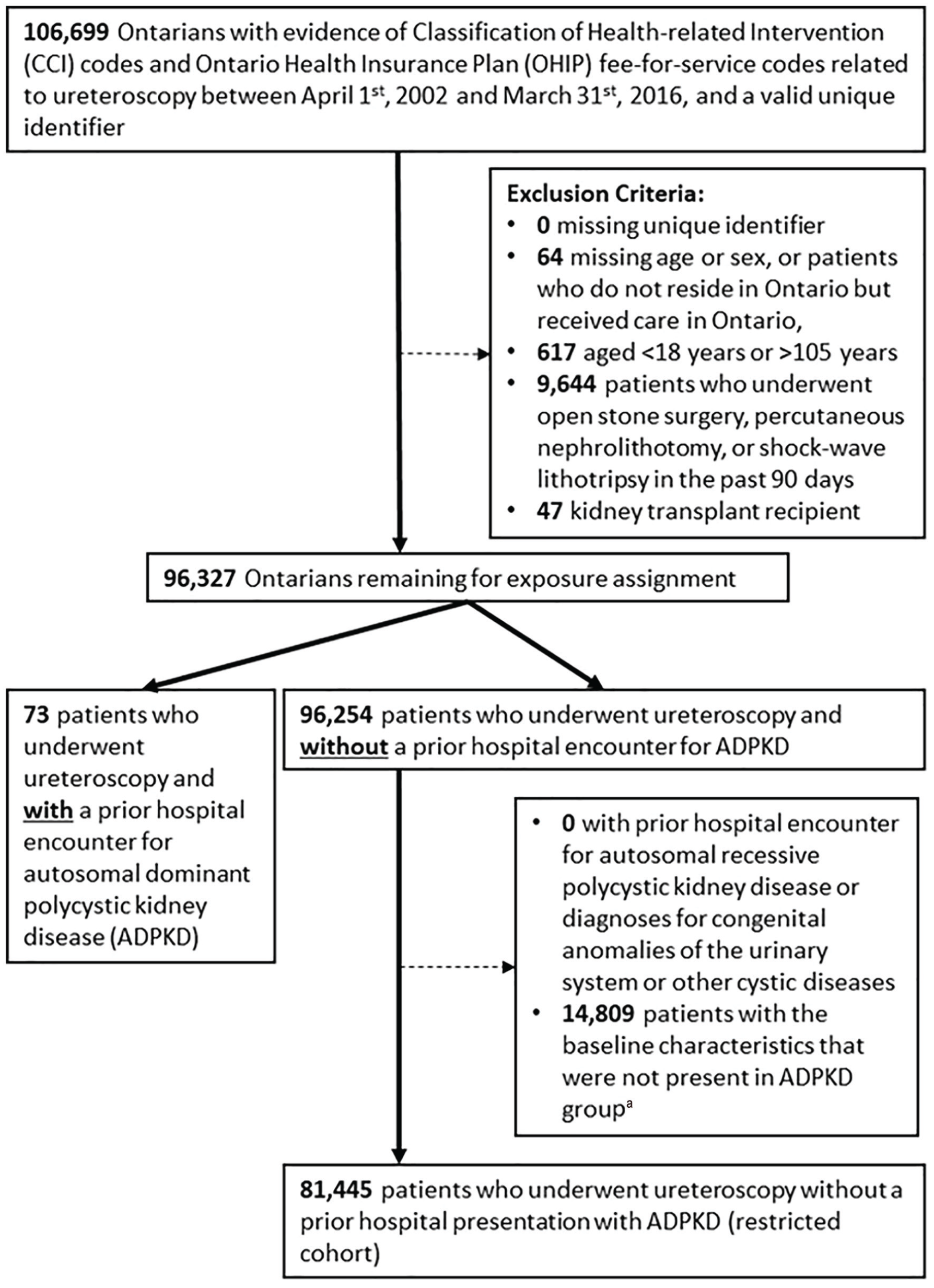
Cohort selection.
Characteristics of Patients With and Without ADPKD at the Time of Cohort.

Note. ADPKD = autosomal dominant polycystic kidney disease; IQR = interquartile range.
Unlike hypothesis testing, standardized difference is not influenced by sample size. A standardized difference of <10% indicates negligible difference.
Average neighborhood income was categorized into fifths on index date. Income quintile was missing for 0.18% of the entire study cohort. For these individuals, middle-income quintile was assigned.
Rural/urban residency status was missing for .05% of the entire study cohort. For these individuals, we assumed they resided in an urban area.
Data on prescription filled was only available in 32 patients with ADPKD, and 31 411 patients without ADPKD.
Diabetic medications represent a combination of insulin and antiglycemic medications.
Data on kidney function was only available in 41 patients with ADPKD and 38 155 patients without ADPKD.
Follow-Up
None of the 73 (0.0%) patients with ADPKD and 142 of 81 445 (0.2%) patients without ADPKD died during the 30-day follow-up.
Outcomes
The risk of ureteroscopic complication was not significantly different between patients with and without ADPKD, although the estimates were imprecise (6 of 73 [8.2%] patients with ADPKD vs. 3537 of 81 445 [4.3%] patients without ADPKD; adjusted RR 1.5, 95% CI = 0.7 to 3.2) (Table 2). Median (IQR) time to ureteroscopic complication among those who had one was 16 (5-20) days in patients with ADPKD versus 8 (4-15) days in patients without ADPKD.
30-Day Risk of Ureteroscopic Complications, Hospital Presentation, Hospital Admission, and Emergency Department Visits in Patients With Compared to Patients Without ADPKD.
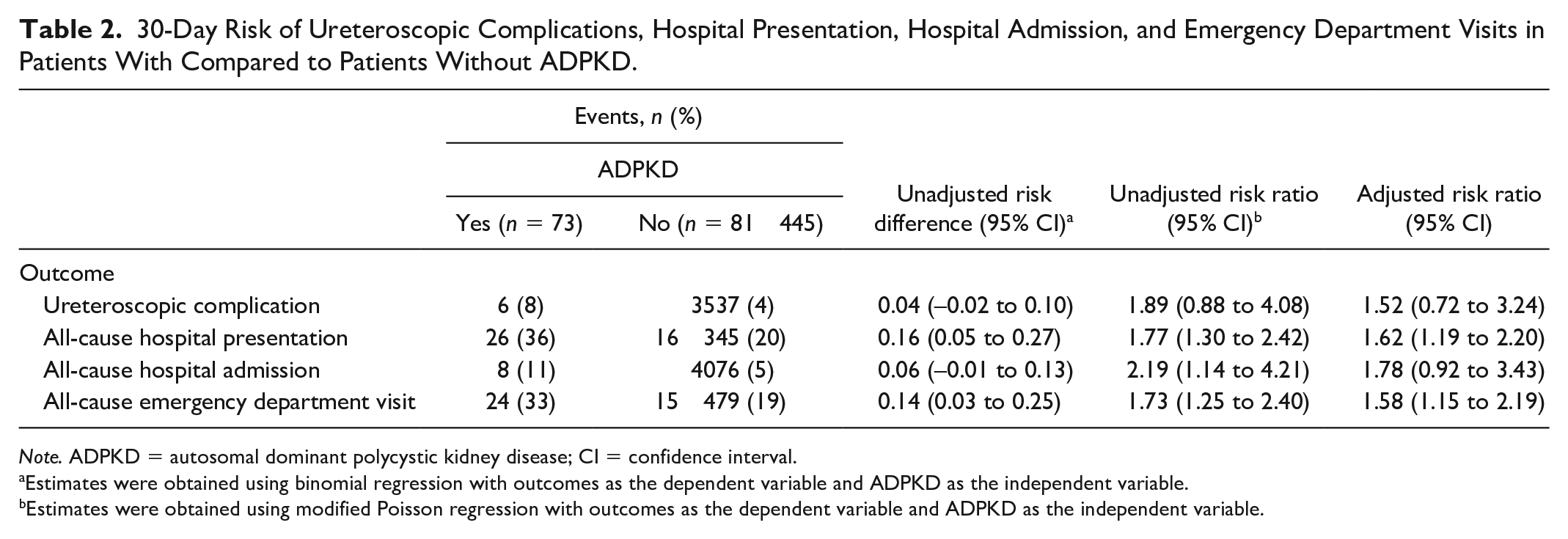
Note. ADPKD = autosomal dominant polycystic kidney disease; CI = confidence interval.
Estimates were obtained using binomial regression with outcomes as the dependent variable and ADPKD as the independent variable.
Estimates were obtained using modified Poisson regression with outcomes as the dependent variable and ADPKD as the independent variable.
Compared to patients without ADPKD, patients with ADPKD were more likely to present to hospital after their procedure (26 of 73 [35.6%] patients with ADPKD vs. 16 345 of 81 445 [20.0%] patients without ADPKD; adjusted RR = 1.6, 1.2-2.2), which included a statistically significant increase in the risk of presenting to the emergency department (24 of 73 [32.9%] vs. 15 479 of 81 445 [19.0%]; adjusted RR 1.6, 95% CI = 1.1-2.2) but not hospital admissions (8 of 73 [10.9%] vs. 4076 of 81 445 [5.0%]; adjusted RR = 1.8, 0.9-3.4) (Table 2). The most common diagnosis for those coming to the emergency department was renal colic or abdominal pain; 9 (12.3%) patients with ADPKD and 3908 (4.7%) patients without ADPKD presented to the emergency department with one of these diagnoses. Twenty four (33.9%) patients with ADPKD and 32 627 (40.0%) patients without ADPKD had stent placed on date of cohort entry. Median (IQR) time to emergency department visit (6 [2-15] days in patients with ADPKD versus 5 [2-11] days in patients without ADPKD.
Discussion
The distorted kidney anatomy in patients with ADPKD may make performing ureteroscopy challenging compared to the general population. We described the 30-day risk of ureteroscopic complications, all-cause hospital presentation, all-cause hospital admission, and all-cause emergency department visit in patients with ADPKD, and compared it to patients without ADPKD. In general, all outcomes were common (although not necessarily statistically significant) in the ADPKD population. Specifically, the 30-day risk of ureteroscopic complications was not significantly different between patients with and without ADPKD. However, there was a statistically significant increase in hospital presentation; this was observed when looking at emergency department visits alone, and similar point estimate was observed for hospital admission, but it was not statistically significant.
Our group recently conducted a thorough systematic review summarizing the outcomes of the three commonly used stone interventions in patients with ADPKD. Currently, there are only 6 case series describing the postureteroscopy outcome in a total of 43 patients with ADPKD with the largest case series consisting of 13 patients with ADPKD.22-28 According to the 6 published case series, the overall risk of complication ranged between 0% and 27%; postoperative complications described in the literature includes fever, pain, and hematuria.22-28 While case series and report provide insight into postoperative outcomes of ureteroscopy experienced by patients with ADPKD, it does not provide strong empirical evidence into whether ADPKD is truly associated with ureteroscopic complications. Our cohort study is the first and largest study to date to examine this association (approximately 6 times larger than the largest published case series). In addition, our study had minimal death; no patient with ADPKD died, and it is unlikely that many people would have traveled out of Ontario during the 30-day follow-up.
There may be reasons why patients with ADPKD presented to the emergency department after ureteroscopy more than patients without ADPKD. It is possible that patients with ADPKD may experience ureteroscopic-related complications that are not part of our composite outcome. For example, pain is a postureteroscopic complication according to the two case series published in the literature; as this was nonspecific, we did not include it in our composite outcome.24,28 Our post hoc analysis showed that pain is the most common reason for presenting to the emergency department and appear to be more prevalent in ADPKD.
Our study is not without limitations. First, the codes for ureteroscopy have not been formally validated, so we had to rely on clinical expertise and knowledge of billing practices to define the outcomes. However, we expect the codes for ureteroscopy to have excellent validity similar to other fee-for-services codes. The study is also limited by what is available in the health care administrative databases. We could not adjust for all important covariates, such as surgeon characteristics, and the accuracy and validity of each covariate was not perfect; this may have introduced residual confounding and affected the association between ADPKD and outcomes. We also could not examine whether the association between ADPKD, and the outcomes were modified by cystic burden, mutation type, and kidney size, and examine prior comorbidities as potential risk factors of outcome due to our small sample size. This study was not designed to examine the 30-day risk of return to hospital in patients with ADPKD compared to other genetic or cystic renal disease condition, which should be considered in future studies. We selected ureteroscopy complications that we thought would represent common issues encountered postoperatively, and rare complications such as ureteral perforation, or common complications such as retained stone fragments/incomplete stone treatment could not be accurately measured with administrative data. Patients may have been presumptively diagnosed with UTI; however, we expect the misclassification to be nondifferential between patients with and without ADPKD. Finally, the low event rate led to imprecision around the estimates. As a result, future studies with a larger number of patients are needed.
Conclusion
In this study of patients who underwent ureteroscopy for upper urinary tract stones, those with ADPKD did not have a statistically significant higher 30-day risk of selected ureteroscopic complications. However, they did have a significantly higher 30-day risk of all-cause hospital presentation and all-cause emergency department visits. Future studies with a larger number of patients are needed to better elucidate whether ureteroscopy is safe in patients with ADPKD.
Supplemental Material
sj-pdf-1-cjk-10.1177_2054358120972830 – Supplemental material for Complications in Patients With Autosomal Dominant Polycystic Kidney Disease Undergoing Ureteroscopy: A Cohort Study
Supplemental material, sj-pdf-1-cjk-10.1177_2054358120972830 for Complications in Patients With Autosomal Dominant Polycystic Kidney Disease Undergoing Ureteroscopy: A Cohort Study by Vinusha Kalatharan, Blayne Welk, Danielle M. Nash, Eric McArthur, Justin Slater, Sisira Sarma, York Pei and Amit X. Garg in Canadian Journal of Kidney Health and Disease
Footnotes
Acknowledgements
Parts of this material are based on data and/or information compiled and provided by CIHI. The analyses, conclusions, opinions, and statements expressed herein are those of the authors, and do not reflect those of the funding or data sources; no endorsement is intended or should be inferred here.
Ethics Approval and Consent to Participate
The use of ICES data in this project was authorized under section 45 of Ontario’s Personal Health Information Protection Act, which does not require review by a Research Ethics Board. No informed consent from patients was required.
Consent for Publication
Consent for publication was obtained from all authors.
Availability of Data and Materials
Not applicable.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Y.P. served as an expert consultant on drug development (Otsuka, Pfizer, and Genzyme/Sanofi) related to autosomal dominant polycystic kidney disease. All other authors declare no competing interests.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by ICES, which is funded by an annual grant from the Ontario of Health and Long-Term Care (MOHLTC). The ICES Kidney, Dialysis, and Transplantation Program provided funding for this study. V.K.’s training was supported by the Canadian Institutes of Health Research Doctoral Scholarship and the Doctoral Scholarship from the KRESCENT Program (a national kidney research training partnership of the Kidney Foundation of Canada, the Canadian Society of Nephrology, and the Canadian Institutes of Health Research). A.G. was supported by Dr. Adam Linton Chair in Kidney Health Analytics and a Clinician Investigator Award from the Canadian Institutes of Health Research.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.