
Abstract
Background:
An increased number of end-stage renal disease patients suffer psychosocial conditions and may experience delayed access to transplantation due to listing restrictions. However, it remains to be shown whether preexisting psychosocial conditions confer an independent risk factor of poor posttransplant outcomes.
Objective:
We addressed this gap in knowledge by conducting a retrospective cohort study to investigate an independent association between the risk of death after transplant and having a diagnosis of psychosocial conditions 1 year prior to starting dialysis.
Methods:
All cases of adult deceased-donor kidney transplantation performed in Ontario, Canada, between April 1, 2002, and March 31, 2013, were used. Propensity score matching was applied to adjust for potential endogenous bias of using predialysis psychosocial status to predict posttransplant mortality. Survival analysis techniques, including Kaplan-Meier curves and Cox proportional hazards modeling, were also used.
Results:
Our results indicate a 49.4% (hazard ratio [HR] = 1.494 [95% confidence interval (CI) = 1.168-1.913]) increased relative risk of posttransplant death to be associated with predialysis psychosocial conditions, when other factors are held constant. The effect is significant (P = .001) and is independent of other known predictors of death including advanced age.
Conclusions:
Findings from this study offered strong support for the development of psychosocial evaluation to screen candidates prior to transplant listing and early interventions for transplant candidates with psychosocial concerns.
What was known before
Psychosocial conditions such as depression are common among end-stage renal disease patients and may adversely affect kidney transplant outcomes.
What this adds
Early diagnosis of psychosocial conditions at 1 year prior to dialysis initiation is an independent risk factor of all-cause death after deceased-donor kidney transplantation. Having predialysis psychosocial conditions is associated with a 49.4% increased relative risk of death after transplant.
Introduction
End-stage renal disease (ESRD) is associated with high symptom burdens that severely affect patients’ functional status and quality of life. Apart from physical conditions such as fatigue and dyspnea, psychosocial conditions (PCs) are highly prevalent among ESRD patients. 1 Depression is the most common PC that coexists with ESRD, affecting 20% to 57% of the population.2-5 Other common PCs among ESRD patients include anxiety, personality disorders, psychotic disorders (eg, schizophrenia), and other mental health issues (eg, substance abuse). 6
Transplantation is the most sought-after ESRD treatment that extends life expectancy7,8 and improves life quality.7,9 However, outcomes of transplant are sensitive to a range of factors, some of which are closely related to PCs. Correlates of depression among ESRD patients (eg, multiple comorbidities)10,11 are usually prognostic of death after transplant. 12 Furthermore, having PCs may be associated with a higher likelihood of nonadherence after transplant,13-18 which is a major risk factor of acute rejection,19,20 graft failure,19,21 and death. 22 In Ontario, Canada, having a history of PCs (such as depression and schizophrenia) predisposed patients to a 17% decreased odds of completing transplant workup within 2 years of referral and a 12% decreased odds of transplantation. 6 Hence, for patients with PCs who are transplanted, they are likely to have been exposed to an extended wait time on dialysis, which is a risk factor for poor survival after transplantation.23-25
Studies seldom looked at transplant recipients with an early diagnosis of PCs as most of them focused on recipients who presented with PCs after transplantation.26-28 As early PCs that were diagnosed before dialysis initiation may not translate into active PCs that persist after transplantation, 29 it remains unclear from the current literature whether early psychosocial symptoms constitute an independent risk factor of poor patient survival after transplant. A single-center study in Toronto, Canada, 19 was unable to identify an effect of having a history of PCs on the rate of acute rejection, graft failure, or death-censored graft failure. However, as the literature has demonstrated, a history of PCs is likely to influence posttransplant outcomes via multiple pathways (eg, by extending pretransplant dialysis duration), a mechanism that introduces endogenous bias in the estimation of a true treatment effect.
In this study, we examined a 2-fold study objective, including (1) to test the hypothesis that kidney transplant recipients with a diagnosis of PCs at 1 year prior to initiating dialysis experienced a longer pretransplant dialysis time than their PC-free counterparts, and (2) to assess the relationship between the risk of death after kidney transplantation and a diagnosis of PCs at 1 year prior to initiating dialysis. We used a cohort (n = 4582) of deceased-donor kidney transplant recipients from Ontario, Canada, in the analysis as living-donor kidney transplants are often associated with different patient cohorts and allocation routines. 30 Propensity score matching method was applied to derive an unbiased relative risk of death due to predialysis PCs.
Materials and Methods
Study Design and Patient Cohort
We conducted a retrospective, population-based, cohort study of adult recipients of first-time, kidney-only transplantation from a deceased donor in Ontario, Canada, between April 1, 2002, and March 31, 2013 (n = 5922). This time period was chosen to align with Ontario’s adaptation of the International Statistical Classification of Disease and Related Health Problems, Tenth version, Canada (ie, ICD 10-CA) in 2002. 31 Patients were followed up until death or till April 1, 2014. Patients who had received a preemptive transplant, living-donor transplant, multi-organ transplant, re-transplant, or had age <18 years at the time of transplantation were excluded.
Data Source
This study used a population-based data set derived by the Institute for Clinical Evaluative Sciences (ICES) that links various administrative databases to patient-level data from the Canadian Organ Replacement Register (CORR) by a validated unique patient identifier. Dialysis centers, transplant centers, and organ procurement organizations in Canada are obligated to report all cases of end-stage organ failure and the respective treatments to the CORR. 32 Hence, the CORR contains complete follow-up data for ESRD patients from the first renal replacement therapy to death. 32
Tracking Comorbidity
The Johns Hopkins Adjusted Clinical Group (ACG) system, 33 a well-validated method of categorizing comorbidities and predicting mortality, 34 was used to classify patient’s comorbidity at 1 year prior to starting dialysis. This was computed using administrative records, including ICD 10-CA diagnosis codes from the Discharge Abstract Database (DAD), a database that includes acute care inpatient hospitalizations; physician billing codes from the Ontario Health Insurance Plan (OHIP); and records from the National Ambulatory Care Reporting System (NACRS). The ICD 10-CA codes were assigned to 1 of the 32 Aggregated Diagnosis Groups (ADGs) based on 5 clinical dimensions, including the duration of the condition, severity, diagnostic certainty, etiology, and involvement of special care. 33 ADGs were further collapsed into 12 Collapsed ADGs (CADGs) based on the likelihood that the condition would persist or recur, severity, and the type of health care services required. 33 Supplementary Table S1 summarizes each of the 12 CADGs and the ADGs as well as common ICD 10-CA codes that they comprise. In our study, each of the 12 CADGs was denoted using an indicator variable.
Outcome and Exposure Variables
All-cause death after transplant is the outcome of our study. Each patient’s date of death was obtained from Ontario’s Registered Person Database (RPDB), a population-based registry. The main exposure of interest is represented by a binary variable that indicates a diagnosis of PCs at 1 year before dialysis initiation, CADG 10. 33
Covariates
Additional patient-level covariates considered in our analysis included demographic characteristics (from the RPDB): sex (female or male), race (Caucasian, Asian, Black, Indian subcontinental, other races, or unknown race), and location of residence (membership of 1 of the 14 Local Health Integration Networks or LHINs) 35 ; transplant-related information (from CORR records): age at transplantation (age group of 21-30, 31-40, 41-50, 51-60, 61-70, or 71+), primary kidney diagnosis (glomerulonephritis, diabetes, renal vascular, congenital or hereditary, other diagnoses, or unknown diagnosis), peak class I panel reactive antibody or PRA (<20%, 20%-79%, ≥80%, or unknown), blood type (O, A, B, AB, or unknown), year of transplantation (2002-2013), transplant center (membership of 1 of the 6 transplant centers in Ontario) 36 ; comorbidity status: 11 CADGs. We calculated pretransplant dialysis duration as the interval in days between the dialysis initiation date and the transplantation date (both dates were obtained from the CORR).
Statistical Analysis
We denoted patients with CADG 10 = 1 to be in the PC group while those with CADG 10 = 0 to be in the PC-free group. Baseline characteristics of patients were summarized by group. A χ2 test was used to assess the distribution of categorical variables in the 2 groups and a 2-sample t test was used for the mean of continuous variables.
Propensity Score Matching
An independent association between the risk of posttransplant death and the status of predialysis PCs cannot be estimated directly using a crude regression due to potential endogenous bias. 37 Propensity score methods aim to create a balanced distribution of observed covariates between the exposed and the unexposed subjects before estimating an unbiased causal effect. To do so, a propensity score or the probability of being exposed conditional on observed covariates is estimated.38-41 Three primary techniques are then applied to calculate the effect, including matching, covariate-adjustment, and stratification (or subclassification).40,41 Although there is no agreement on the most appropriate technique to use, 41 matching is commonly applied when the number of unexposed subjects far exceeds the number of exposed subjects. 40 In our study, the ratio between patients in the PC and PC-free group is about 1:4, which is significant enough to necessitate a matching analysis.
We followed an analytical process demonstrated by Austin 42 and Austin and Mamdani. 41 First, propensity score was estimated by a logistic regression that modeled the probability of having PCs given measured confounders that were hypothesized to influence both the likelihood of having PCs and the risk of posttransplant death. 43 These confounders included patient sex, age, race, transplant year, primary kidney diagnosis, comorbidity, and pretransplant dialysis duration. We also included variables that were prognostically important correlates of posttransplant death but not of predialysis PCs because controlling for them would potentially reduce bias.43-45 These covariates included patient’s location, transplant center, and peak PRA. We followed a structured, iterative algorithm 39 to determine a specification of the logistic model that produced balanced propensity scores in the PC/PC-free groups. Details of the construction of a propensity score and balance diagnostics were presented in the Supplementary Appendix. We applied greedy 1:1 matching without replacement that used a caliper distance that equaled 20% of the standard deviation of the logit of propensity score to form matched pairs.46,47 Balance diagnostics were performed where McNemar tests (for categorical variables) or paired t tests (for continuous variables) were used to assess the distribution of characteristics in the 2 groups after matching. 47 Standardized differences were calculated to ensure no covariates exceeded the 10% threshold. 41
Absolute and Relative Risk of Death
Kaplan-Meier curve was used to estimate patient survival in the matched sample. To avoid bias due to the matched nature of our sample, we used stratified log-rank test that was based on the 6 patient age groups rather than the conventional log-rank test to determine whether PC/PC-free patients had different survival functions.42,48 The absolute increase in the risk of death due to PCs at different time points after transplant was computed. 42 A univariate Cox proportional hazard model was applied in the matched sample to regress posttransplant survival on PC status. This estimated a hazard ratio (HR) of having PCs on death or the relative risk of death due to PCs. 42 Robust estimation of the standard error of the HR was applied to reduce the bias from the matched sample. 49 A Cox proportional hazards analysis using the original, unmatched sample was conducted to compare the results derived from the matched analysis.
Sensitivity Analysis
Imputation of pretransplant dialysis duration (n = 288 missing) was based on patient’s blood type, a variable that has been demonstrated 50 to strongly predict pretransplant dialysis time. Specifically, the mean duration for patients with nonmissing value in the same blood type group was used. Analyses were conducted using the command psmatch2 51 in Stata/MP 13.1.
Results
Cohort Description
Among 5922 deceased-donor kidney transplant recipients (Figure 1) in Ontario, Canada, 225 patients had received the transplant preemptively; 540, 63, and 7 patients had received a second, third, or fourth transplant, respectively; 55 and 159 patients had age between 1 and 10 and 11 and 20 years at transplantation, respectively; 2 and 288 patients had unknown sex or unknown pretransplant dialysis duration, respectively; and 1 patient was lost to follow-up. Exclusion of these patients resulted in 4582 patients in the final cohort. Mean follow-up time after transplant was 2588.6 days or 7.1 years (SD = 1273.1 days).

Inclusion and exclusion of transplant recipients in the study cohort.
Baseline Characteristics
Table 1 summarizes baseline characteristics of patients based on PC status. At 1 year prior to initiating dialysis, 20.8% (n = 954) of patients had a diagnosis of PCs. About 16.1% of them (n = 154) died after transplantation within our observational period while 14.2% of PC-free patients (n = 517) died. This difference was not statistically significant (P = .14). Patients with PCs tended to be female (P = .06), had younger age at transplantation (P = .005), and had shorter pretransplant dialysis duration (P = .004). Notably, patients with PCs spent an averaged 1326.6 days (SD = 983.7 days) on pretransplant dialysis, which is 107 days less compared with PC-free patients (mean = 1434.1 days; SD = 1046.9 days) and 85 days less than the mean dialysis time of the entire cohort (mean = 1411.7 days; SD = 1034.9 days).
Comparing Baseline Characteristics of Transplant Recipients Based on Psychosocial Diagnosis (CADG 10) at 1 Year Prior to Initiating Dialysis, n = 4582.

Note. Categorical variables are summarized as counts and percentages in the respective PC or PC-free group, whereas continuous variables are reported as mean ± standard deviation. A χ2 test is used to compare the distribution of categorical variables between the 2 groups of patients. The mean of continuous variables is assessed using a 2-sample t test. CADG = Collapsed Aggregated Disease Group; PC = psychosocial conditions; PRA = panel reactive antibody; LHIN = Local Health Integration Network.
Difference of other comorbid conditions was observed between patients with and without PCs. Compared with PC-free patients, patients with PCs were more likely to also have conditions that were acute minor (CADG 1, P < .001), acute major (CADG 2, P < .001), likely to recur (CADG 3, P < .001), asthma (CADG 4, P = .005), chronic medical/stable (CADG 6, P < .001), preventive/administrative (CADG 11, P = .006), and pregnancy (CADG 12, P < .001). The distribution of patients with PCs also differ among the 6 transplant centers in Ontario (P = .02).
Risk of Death Due to Predialysis PCs
Results of propensity score matching is detailed in the Supplementary Appendix. A 1:1 caliper matching yielded 945 pairs of PC/PC-free patients where 99.1% of PC patients (945 of 954) in the original sample were matched to a PC-free patient. About 0.9% (n = 9) of PC patients could not be matched due to their high propensity scores and were thus discarded from the analysis. Balance diagnostics in the matched sample were summarized in the Supplementary Appendix.
Figure 2 shows Kaplan-Meier curves that depicted patient survival after transplantation. Before matching, log-rank test suggested a trend toward a different survival (P = .09) between PC/PC-free patients. Graphically, the 2 curves crossed as time increased (top half of Figure 2). After matching, we observed different survival patterns for patients in the 2 groups as those with PCs had a lower survival probability at all time points after transplantation and the absolute difference increased with time (bottom half of Figure 2). Stratified log-rank test based on the age groups confirmed the difference in survival between the PC/PC-free patients (P = .003, .006, .007, .02, .02, and .04 for age groups of 21-30, 31-40, 41-50, 51-60, 61-70, and 71+ years, respectively).

Kaplan-Meier curves of posttransplant patient survival before and after matching.
Table 2 presents the absolute risk of death due to predialyiss PCs at given time points after transplantation. While PC patients had a lower survival rate at all time points than PC-free patients, the absolute difference tended to grow with posttransplantation time, from 0.8% at 674 days (about 1.8 years) to 6.5% at 5385 days (about 14.7 years) after transplantation.
Kaplan-Meier Estimates of the Absolute Risk of Death Due to Predialysis PCs at Different Time Points After Transplantation Using the Matched Sample.
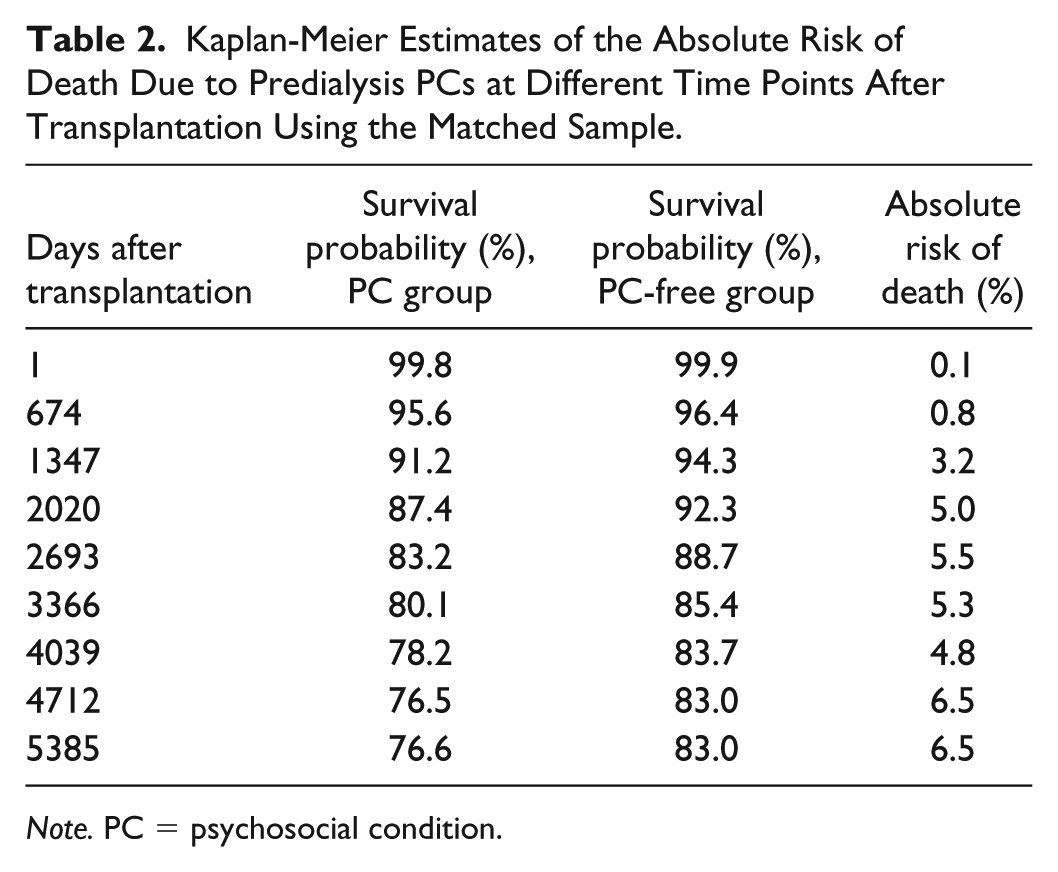
Note. PC = psychosocial condition.
Table 3 presents the results of a univariate Cox proportional hazard model that assessed the relative risk of death due to PCs in the matched sample. Compared with PC-free patients, those with PCs were associated with a significant (P =.001) 49.4% (HR = 1.494 [95% robust confidence interval (CI) = 1.168-1.913]) increased relative risk of death after transplant. We also estimated the HR of PCs using the unmatched sample. All of the 5 Cox models that adjusted for different covariates suggested a significant (P = .005-.09) relative risk of death due to PCs, but the HRs were smaller than the one derived from the matched analysis, ranging from 1.164 (unadjusted) to 1.285 (comorbidity-adjusted) to 1.286 (demographic-adjusted) to 1.287 (adjusted for all covariates), and to 1.296 (adjusted for covariates with P < .05 in the log-rank test).
Relative Risk of Posttransplant Death Due to Predialysis Psychosocial Conditions Using Different Methods.

Note. HR = hazard ratio; CI = confidence interval; CADG = Collapsed Aggregated Disease Group.
Adjusted for sex, age, race, and location.
In addition to all demographic variables, 11 binary variables of CADGs were adjusted.
This include sex, age, race, location, primary kidney diagnosis, transplant year, transplant center, CADG 6, and CADG 8.
Sensitivity Analysis
Of the 288 patients with unknown pretransplant dialysis duration, 118, 123, 35, and 12 patients had blood type O, A, B, and AB, respectively. For the other (n = 4582) patients, the mean pretransplant dialysis duration was 1515.4, 1278.9, 1629.1, and 1105.3 days for blood group O, A, B, and AB, respectively. After imputation, we re-run our original specification of the propensity score model and found no imbalance between the PC/PC-free group. Standard deviation of the logit of propensity score became 0.082 which suggested an optimal caliper distance of 0.016 to be used in the matching. This resulted in 947 pairs of PC/PC-free patients (99.3%) where 7 PC patients (0.7%) were excluded. Univariate Cox proportional hazard model estimated a 39.1% (HR = 1.391 [95% robust CI = 1.123-1.730]) significant (P = .03) relative increase of death due to PCs using the imputed matched sample. Hence, imputation of pretransplant dialysis duration using the blood group mean drove down the HR of PCs on death, which means our estimation is moderately sensitive to changes in patient’s length of dialysis before transplantation.
Discussion
To the best of our knowledge, this is the first study that used propensity score matching to estimate an unbiased effect of predialysis PCs on posttransplant death among deceased-donor kidney transplant recipients. We followed a rigorous analytical procedure and reported a 49.4% increased relative risk of death to be associated with a diagnosis of PCs at 1 year prior to dialysis initiation. This effect is independent of demographic characteristics, comorbidities, duration of pretransplant dialysis, transplant centers, and other clinical indicators of ESRD. In Ontario, Canada, the median wait time on dialysis before receiving a deceased-donor kidney transplant is 4.1 years (or 1507 days). 52 Hence, our results suggested that being diagnosed with PCs at as early as 5 years prior to the expected date of deceased-donor kidney transplantation constituted an important marker of poor survival after transplant.
Contrary to our hypothesis, ESRD patients with predialysis PCs in our cohort experienced a shorter dialysis episode prior to transplantation than their PC-free counterparts. The difference was clinically meaningful due to an absolute value of standardized difference that exceeded 10% (15%). It is unknown to us why predialysis PCs appeared to give transplant candidates faster access to transplantation, but even with the protective effect of a shorter pretransplant dialysis duration, predialysis PCs still conferred a negative effect on posttransplant survival, which in turn made our conclusion more compelling.
We also conducted multiple survival analyses using the unmatched sample of patients, which returned lower estimates of HR of predialysis PCs on posttransplant death. Hence, we conclude that without properly adjusting for confounding, conventional methods are likely to underestimate the true causal effect of early PCs on patient survival after transplant.
Our conclusion was not in congruence with most studies that assessed the effect of early PCs on posttransplant death. A evaluation 19 conducted at the Toronto General Hospital in Canada using 955 adult kidney transplant recipients reported no additional risk of acute rejection, graft loss, or death-censored graft failure among those with a history of mental health concerns. However, the study cohort was not exclusively nonpreemptive, deceased-donor transplant recipients. Rather, 56% and 12% of patients had received a living-donor transplant or a preemptive transplant. Hence, the worsened posttransplant outcome among recipients with pretransplant mental health issues may become less obvious when these patients also carried significant survival advantage related to receipt of a living-donor kidney and avoidance of dialysis.
A single-center study 53 that used the Stanford Integrated Psychosocial Assessment for Transplantation (SIPAT) to screen for problematic transplant candidates found no association between the rate of mortality at 1 year posttransplantation and a high SIPAT score (indicating severe PCs) before transplantation among 217 transplant recipients. They did, however, suggest higher rate of infections among patients with more severe pretransplant PCs, an event that is predictive of death. 23 Hence, we argue that although difference of mortality was not directly observed by the study possibly due to the short follow-up time and small sample of patients, their conclusions partially corroborated with ours.
Evans et al 54 analyzed 960 US veterans with mental health illnesses diagnosed at 1 year prior to a solid organ, including kidney (n = 396), or bone marrow transplantation. Three-year mortality was equal among patients with different pretransplant mental health status. However, they pointed out that one would expect a more divergent survival patterns after the fifth year where those with pretransplant mental health illnesses began to deteriorate much faster than their mentally healthy counterparts. In our analysis, we showed that the absolute risk of death due to PCs reached 5% after 2020 days (or 5.5 years) posttransplantation and continued to grow to 6.5% after 4712 days (12.9 years). Before 5.5 years, the absolute risk was less prominent (0.8% and 3.2% after 674 and 1347 days, respectively), which may in part explain why Evans et al were unable to conclude any effect. However, according to our results, the relative risk of posttransplant death due to PCs stayed constant throughout the trajectory of posttransplant follow-up at 49.4%.
There are possible explanations to our findings. Early PCs that were diagnosed before dialysis initiation may or may not translate into active PCs that persist after transplantation. 29 If they do, there is strong evidence from the literature that directly associates posttransplant PCs to elevated rates of nonadherence and death.26-28 If these symptoms do not persist after transplant, possibly due to being cured or controlled by psychiatric treatments prior to transplant listing, we suspect that some permanent neurocognitive and physical damage may have been occurred that predispose these patients to an irreversibly disadvantaged state at the time of transplantation. For example, chronic and heavy cannabis use has been shown to lead to permanent loss of memory and brain function impairment that are irreversible by active detoxification and abstinence. 55 Hence, past cannabis abusers in receipt of a transplant may face a high risk of not taking their medications due to increased forgetfulness, which subsequently heightens their risk of graft loss and death. 13
The high risk of posttransplant death due to predialysis PCs concluded in our analysis is not influenced by other predictors of death because of our use of propensity score matching. Hence, the study findings call for future policies and interventions that target the detection and correction of PCs prior to kidney transplantation. Our results suggest that early screening that occurred before dialysis initiation is likely to capture psychosocially impaired ESRD patients who may progress quickly to death after future receipt of a transplant. In Ontario, the determination of a patient’s psychosocial status largely relies on self-reported results during informal interviews, which are only conducted in preparation for transplant listing. 19 Hence, stringent policies are needed to enforce a comprehensive psychosocial assessment of ESRD patients before dialysis initiation. Prescription of antidepressant medications for ESRD patients who are soon to be transplanted needs to be carefully monitored to reduce future risk of drug interactions. Furthermore, we showed in our analysis that transplant candidates who were PC-free actually experienced a longer pretransplant dialysis episode, which reflects a potential inadequacy in the current algorithm used for the management of waitlisted patients. Because patients with predialysis PCs constitute a group of high-risk transplant candidates, transplant programs should allow sufficient time for these patients to engage in active psychiatric therapies before transplantation. This will enable patients without the risk to obtain a timely transplant and gain the full benefit of transplantation.
Our study has several limitations. First, we did not have information on patients with predialysis PCs who did not receive a transplant or died on the wait list. Hence, the psychosocial effect concluded in our analysis is likely to be a conservative estimation of the true effect as those who eventually received a transplant probably have relatively mild PCs that passed pretransplant assessment. 19 Second, we were unable to evaluate patient adherence after transplantation or if predialysis PCs persisted after transplantation. However, the objective of the study is to convey an independent association between early history of PCs and posttransplant death. Future studies with more comprehensive data need to elucidate the specific mechanism of how predialyiss PCs influence patient survival after transplant. Third, despite our acknowledgment on the heterogeneous nature of PCs among ESRD patients, we did not conduct any subgroup analysis to assess whether the risk of posttransplant mortality differed by types of PCs. This is due to our limited access to the person-level ICD 10-CA information in our data set which impeded us to make any further groupings of PCs. Similarly, although we concluded a statistically shorter duration of pretransplant dialysis experienced by patients with predialysis PCs compared with their PC-free counterparts, we were unable to provide any explanations to this observation using the study sample, largely due to our lack of information on patients’ specific PC characteristics. Hence, future investigators who have access to a more detailed tracking of transplant recipients may test the potential differences in pre- and posttransplant outcomes by groupings of early PCs.
Our study demonstrated some key strengths. First, we used a large provincial cohort of transplant recipients with complete follow-up data that enabled the tracking of patients from the year before dialysis initiation to death after transplantation. Second, patient’s predialysis psychosocial status was formally defined using ICD 10-CA diagnostic codes and the ACG system which allowed us to establish an explicit exposure variable in the analysis. Most importantly, we used propensity score matching method to effectively remove the confounding effect, a significant source of bias that we have demonstrated in our analysis to lower the independent effect estimation of predialysis PCs on posttransplant death.
Conclusions
The study finding indicates a strong and independent effect of early diagnosis of PCs on deceased-donor kidney recipient survival. Although the particular pathways by which predialysis PCs reduce posttransplant patient survival are unknown, future policies need to focus on early detection and correction of such conditions among ESRD patients, preferably before transplantation. Effective screening mechanisms for PCs among ESRD patients are required early in the trajectory of care to ensure ample treatment time to prepare patients for future transplantation.
Supplemental Material
PredialysisPCs_CJKHD_Rev2_Clean_supp_1 – Supplemental material for Impact of Predialysis Psychosocial Conditions on Kidney Transplant Recipient Survival: Evidence Using Propensity Score Matching
Supplemental material, PredialysisPCs_CJKHD_Rev2_Clean_supp_1 for Impact of Predialysis Psychosocial Conditions on Kidney Transplant Recipient Survival: Evidence Using Propensity Score Matching by Rui Fu and Peter C. Coyte in Canadian Journal of Kidney Health and Disease
Footnotes
Acknowledgements
The authors thank Dr. S. Joseph Kim for his guidance.
Ethics Approval and Consent to Participate
Institute for Clinical Evaluative Sciences (ICES) is a prescribed entity under section 45 of Ontario’s Personal Health Information Protection Act (PHIPA). Section 45 authorizes ICES to collect personal health information, without consent, for the purpose of analysis or compiling statistical information with respect to the management of, evaluation or monitoring of, the allocation of resources to or planning for all or part of the health system. Projects conducted under section 45, by definition, do no require review by a Research Ethics Board. This project was conducted under section 45, and approved by ICES’s Privacy and Compliance Office. ICES is a designated prescribed entity under section 45 of the PHIPA. Participant informed consent was not required for this study.
Consent for Publication
Not applicable.
Availability of Data and Materials
The data set from this study is held securely in coded form at the Institute for Clinical Evaluative Sciences (ICES). While data sharing agreements prohibit ICES from making the data set publicly available, access can be granted to those who meet prespecified criteria for confidential access, available at ![]() . The full data set creation plan is available from the authors upon request.
. The full data set creation plan is available from the authors upon request.
Author Contributions
R.F. and P.C.C. contributed to research idea, study design, and data acquisition; R.F. contributed to data analysis/interpretation and statistical analysis; and P.C.C. contributed to supervision or mentorship. Each author contributed important intellectual content during article drafting and accepted accountability for the overall work by ensuring that questions pertaining to the accuracy or integrity of any portion of the work are appropriately investigated and resolved.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by the Institute for Clinical Evaluative Sciences (ICES), which is funded by an annual grant from the Ontario Ministry of Health and Long-Term Care. The opinions, results, and conclusions reported in this article are those of the authors and are independent from the funding sources. No endorsement by ICES or the Ontario Ministry of Health and Long-Term Care is intended or should be inferred.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.