
Abstract
Background:
Frailty and functional decline are being recognized as important conditions in kidney transplant candidates. However, the ideal measures of functional status and frailty remain unknown as there is not a complete understanding of the relationship between these conditions and important post-transplant outcomes.
Objective:
The objective was to examine the association between different measures of frailty and functional status evaluated before or at the time of transplant with adverse clinical outcomes post-transplantation.
Design:
This study is a systematic review.
Setting:
Observational studies including cohort, case-control, or cross-sectional studies examining the effect of frailty and functional status on clinical outcomes. There were no restrictions on type of setting or country of origin.
Patients:
Adults who were waitlisted for kidney transplant or had received a kidney transplant.
Measurements:
Data including demographic information (eg, sample size, age, country), assessments of frailty or functional status and their domains, and outcomes including mortality, transplantation, graft loss, delayed graft function and hospital readmission were extracted.
Methods:
A search was performed in Medline, Embase, and Cochrane Central Register for Controlled Trials. Studies were included from inception to February 7, 2023. The eligibility of studies was screened by 2 independent reviewers. Data were presented by frailty/functional status instrument and clinical outcome. Point estimates and 95% confidence intervals from fully adjusted statistical models were reported or calculated from the raw data.
Results:
A total of 50 studies were identified, among which 36 unique instruments were found. Measurements of these instruments occurred mostly at time of kidney transplant, transplant evaluation, and waitlisting. The median sample size of studies was 457 patients (interquartile range = 183-1760). Frailty and lower functional status were associated with an increased risk for mortality. Similar trends were observed among other clinical outcomes such as graft loss and rehospitalization.
Limitations:
The heterogeneity in measurement instruments, study designs, and outcome definitions prevents pooling of the data. Selection bias and the validity of data collection could not be ascertained for some studies.
Conclusion:
Frailty and functional status measures are important predictors of post-kidney transplant outcomes. Further studies are needed to evaluate the best instruments to assess frailty and functional status, and importantly, interventional studies are needed to determine whether prehabilitation strategies can improve post-transplant outcomes.
Registration (PROSPERO):
CRD42016045251.
Introduction
Kidney transplantation is the treatment of choice for most patients suffering from end-stage kidney disease, offering improvements in survival and quality of life compared with dialysis.1,2 Over the last decade, there has been an increase in the number of individuals added to the waitlist for kidney transplants in Canada. 3 Although the number of kidney transplant procedures has also increased concurrently, it has not kept pace with the rate of waitlisting. 3 Consequently, the demand for kidney transplants has surpassed the available supply, making it challenging to provide life-prolonging procedures to everyone in need.4,5 In addition, candidates for kidney transplants tend to have health challenges such as older age, health comorbidities, frailty, and reduced functional capacity, making the evaluation assessment process more challenging.6-11
Frailty is an important determinant in health outcomes and is defined as a heightened state of vulnerability due to declines in strength, endurance, and physiologic function.12,13 Among waitlisted kidney transplant candidates, frailty has been associated with adverse outcomes following transplantation including delayed graft function (DGF), longer hospitalizations, and mortality.6,14 Similarly, a patient’s functional status is an indicator of their overall health and preparedness for transplantation.15,16 Functional status is distinct from frailty in that it measures the ability to complete tasks. Although decreased function is highly associated with frailty, where decreased strength and physiologic function can directly impact one’s abilities,17,18 persons with significant functional limitations due to conditions such as stroke or arthritis may not be frail. Conversely, persons with frailty may not demonstrate functional loss. An enhanced understanding of these risk factors is essential for identifying and mitigating adverse outcomes among at-risk transplant candidates. In addition, research has shown a potential improvement in physical function and frailty following transplantation.7,14,19-21 This potential reversibility with improved kidney function highlights the importance of understanding the impact of frailty and functional status on outcomes in the field of transplantation.
The objective of this systematic review was to examine the association between different measures of frailty and functional status evaluated before or at the time of transplantation with adverse clinical outcomes following kidney transplantation.
Methodology
The methodology used in this study expands upon a previously published systematic review examining frailty in advanced chronic kidney disease (CKD) 22 but with a specific focus on the kidney transplant recipient population. This review was written according to the Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) guidelines 23 and has been registered in the PROSPERO database (CRD42016045251).
Literature Search
A tailored literature search was performed in Medline, Embase, and the Cochrane Central Register of Controlled Trials. We searched for studies from inception to February 7, 2023. Search terms relating to frailty and functional status were used and included the following: kidney transplantation, frailty, muscle weakness, sarcopenia, and functional status (Item S1 in Supplementary Material). Eligibility was restricted to studies in the English language.
Primary research studies including cohort, case-control, and cross-sectional studies were eligible for review. No limitations were set on the duration of follow-up, study setting, or country of origin. Other inclusion criteria were as follows: (a) Population: Adults (≥18 years of age) who were waitlisted for kidney transplant or had received a kidney transplant. (b) Instrument: An assessment of overall frailty or functional status, or their individual domains, provided they measured impairment prior to or at time of transplantation. Both performance-based and self-reported measures were accepted. Frailty was defined as a syndrome resulting from various factors and characterized by reduced strength, endurance, and physiological function. Functional status was defined as an individual’s ability to carry out the normal activities of daily living required to meet basic needs, fulfill usual roles, and maintain health and well-being. (c) Outcome: The primary outcome of interest was mortality post-transplant or while on the kidney transplant waitlist. The following post-transplant outcomes were also collected: graft loss, DGF, hospital readmission, hospital length of stay, and transplantation. The following waitlist outcomes were collected: hospitalization and waitlist inclusion/removal. Composite outcomes such as death or delisting, post-transplant severe adverse events, and hospitalization or death were also captured.
Article Selection and Data Extraction
Studies were examined for eligibility by 2 independent reviewers. Articles that were deemed potentially relevant based on title and abstract were subsequently screened in greater detail, in which the full text was retrieved. When an article was not available in academic databases nor through our academic library, we contacted the corresponding authors in attempt to gain access to the article. The reference lists of included studies were scanned for validation and additional titles. When disagreements arose and consensus could not be reached between 2 reviewers, a third reviewer was consulted for final input.
An abstraction form was utilized to extract data points from the included studies. Items of interest were study design, subject characteristics, details on frailty and functional status instruments, and outcomes. Data were extracted by 2 independent reviewers and verified by both to minimize discrepancies.
Quality Assessment
Each of the included studies was assessed for risk of bias using a modified version of the Quality in Prognosis Studies tool.24-26 This tool provides 6 domains in which several prompting questions are asked about study participation and attrition, instrument and outcome measurements, study confounding, and statistical analysis and reporting. Each of the domains is given a rating of high, moderate, or low risk of bias by a reviewer and verified by another.
Data Analysis and Presentation
Study characteristics were compiled for each study. Sample size and population age were presented as means and standard deviations, unless otherwise indicated. Frailty and functional status instruments were categorized based on the domain they assessed and examined as separate exposures for each outcome (Box 1). Frailty was classified into 5 domains: overall frailty, sarcopenia, slow gait, strength measurement, and physical activity and fatigue. 27 Functional status measures were grouped into 3 categories: Activities of Daily Living (ADL),28,29 performance scale, 30 and physical performance. 31
Definition of Frailty and Functional Status and Their Groupings.

Key outcomes were reported as point estimates and 95% confidence intervals of fully adjusted statistical models. These analyses reported hazard ratios (HRs), odds ratios (ORs), and relative risks (RRs) and were adjusted for a minimum of sex and age, unless indicated differently. In the absence of such data points, unadjusted estimates were reported or calculated using frequencies of healthy vs impaired subject groups. When the same measurements were reported in different units, they were converted to the same units mathematically (eg, studies reporting on the 6-minute walk test were all presented as 100 m unit measures). The heterogeneity in study designs and instruments precluded the pooling of results; therefore, no specific heterogeneity testing was done, and a meta-analysis could not be performed. Finally, main study findings were reported as assessments, with the potential for multiple instruments and/or outcome assessments within a single article. For example, a study measuring the 5 independent frailty domains resulted in 5 distinct outcomes in the systematic review.
Results
Overview
The literature search identified 9414 unique citations (Figure 1). After the initial screening of titles and abstracts, 521 articles were further assessed for eligibility at the full-text level. After this stage, an additional 471 studies were excluded because they focused on a different population, did not report a relevant outcome, or did not measure frailty or functional status. The remaining 50 studies were included in this review.

Search results and study selection.
Supplementary Table S1 provides an overview of the demographic characteristics of the included studies (references available in Item S2). Overall, there were 21 studies (42%) that used a prospective cohort design, 15 studies (30%) used hospital records for data sources and 11 studies (22%) used registry data. The remaining 3 studies performed secondary analysis of established cohorts. Publication dates ranged from 2006 to 2022, with a median publication year of 2019. Most studies (n = 38; 76%) originated from the United States. The median sample size of included studies was 457 patients (interquartile range = 183-1760), and the total sum of sample size for all studies was 668 103 patients.
Instruments
The characteristics of the instruments used to examine frailty and functional status are reported in Supplementary Table S2. Among 50 studies, there were 36 unique instruments used to measure frailty (29 instruments) and functional status (7 instruments). In total, these instruments accounted for 86 assessments, including 63 assessments of frailty. Overall frailty was the primary domain of focus of these studies, noted in 26 assessments, followed by sarcopenia (n = 13 assessments), gait (n = 10 assessments), strength measurements (n = 9 assessments), and physical activity and fatigue (n = 5 assessments). The Fried Frailty Index, including variations of it, was the most frequently used instrument for frailty (n = 13). Functional status instruments accounted for 23 assessments, with the Karnofsky Performance Scale (Karnofsky) and 36-item short-form health survey (SF-36) physical functioning scales being the most used instruments (n = 6 each).
Overview of the Association Between Frailty and Functional Status Instruments and Mortality.

Note. 6MWT = 6-Minute Walk Test; ADL = Activities of Daily Living; aHR = adjusted hazard ratio; aOR = adjusted odds ratio; aSHR = adjusted subhazard ratio; CI = 95% confidence interval; DD = deceased donor; GA = geriatric assessment; HR = unadjusted hazard ratio; IADL = instrumental activities of daily living; Karnofsky = Karnofsky Performance Status; LD = living donor; MD = muscle density; nPFP = new physical frailty phenotype; OR = unadjusted odds ratio; Q = quartile; RR = unadjusted relative risk; SMI = Skeletal Muscle Index; SPPB = Short Physical Performance Battery; STS = Sit to Stand Test.
All models adjusted for a minimum of age and sex, unless otherwise noted. Where a choice of models exists, the most fully adjusted model is presented.
Median.
Mean.
Multiple adjusted models available.
Model not adjusted for sex.
Unadjusted model.
Scale inverted.
RR calculated from event data, or cumulative survival event data.
Model not adjusted for age.
Scale change.
For this study, Karnofsky was used to assess physical activity, instead of functional status.
Measurements using these instruments occurred at various clinical milestones, notably at time of kidney transplantation (n = 13), transplant evaluation (n = 13), or waitlisting (n = 7). Some studies reported multiple time points including at waitlisting and before transplantation (n = 3). The remaining 14 studies reported varying time points’ pre-kidney transplant.
There were 15 distinct outcomes that were examined across all studies. Mortality was the most frequently examined outcome, appearing in 28 studies, followed by hospital readmission after transplantation (n = 11 studies), graft loss (n = 14 studies), hospital length of stay (n = 8 studies), and DGF (n = 8 studies). Additional outcomes included waitlisting denial/removal (n = 8 studies) and kidney transplantation (n = 7 studies). Supplementary Table S3 outlines the remaining outcomes.
Critical Appraisal of Quality
The quality assessment of the studies is summarized in Supplementary Table S4. Four studies (8%) were assessed as having a low risk of bias across all 6 categories, and 6 studies (12%) had a low risk of bias across 5 of the categories. There were 20 studies (40%) assessed to have a high risk of bias in at least 1 of the categories. Overall, the studies performed the best in the outcome measurement category, with 34 studies (68%) identified as low risk of bias in this category.
Mortality
Table 1 provides an overview of the association between various frailty and functional status instruments and mortality. Overall, there were 45 assessments across 28 studies. The majority of studies examined the association in kidney transplant recipients, whereas some were in kidney transplant candidates while on the waitlist. Results were overall consistent between the 2 populations.
There were 14 categorical assessments examining overall frailty. Among these, 71.4% (n = 10) reported a statistically significant association, where being frail prior to transplantation was associated with a 2- to 7- fold increased risk of mortality among waitlisted and transplanted patients (Figure 2). An additional 7 assessments examined sarcopenia, in which 5 unique instruments were used. A single assessment evaluating sarcopenia as a continuous measure reported an increased risk of mortality (Supplementary Figure S1), whereas 3 of 6 categorical assessments of sarcopenia revealed a positive association between sarcopenia and mortality. When the remaining domains of frailty were examined, there was no consistent association with mortality.

Forest plot of the association between frailty as a categorical variable and mortality.§
Abbreviations: HR = hazard ratio; OR = odds ratio; RR* = relative risk calculated from event data; SMI = Skeletal Muscle Index; Unadj = unadjusted model; ¥ = comparison was inverted.

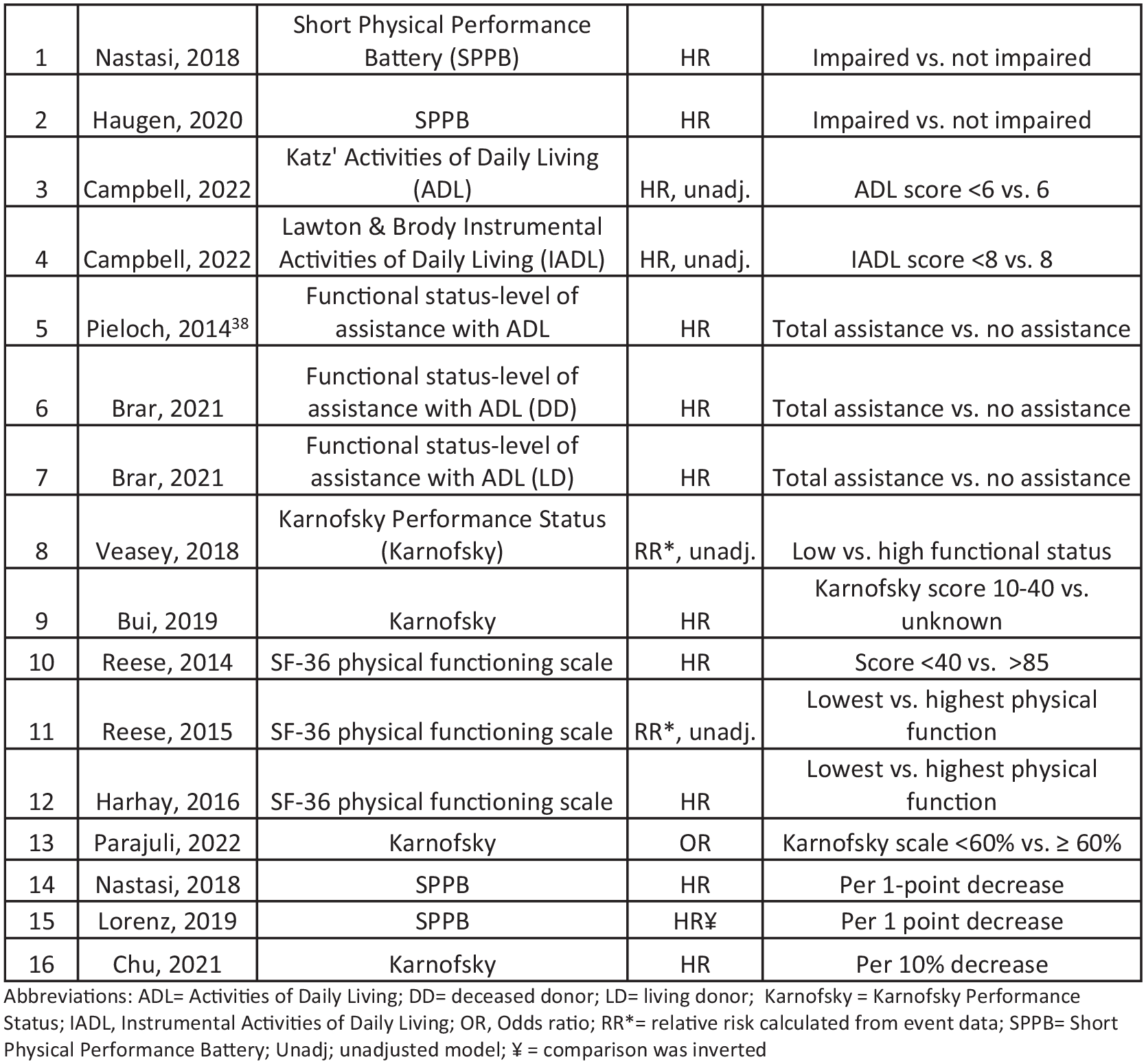
The relationship between functional status and mortality was examined among 16 assessments in 13 studies (Figure 3). Overall, individuals with impaired functional status based on categorical measures of ADL, Karnofsky, and SF-36 physical functioning scale had up to a 2.5-fold increased risk of mortality. Similarly, impaired function using ADL and Karnofsky as continuous measures was also associated with an increased risk of mortality.

Forest plot of the association between functional status and mortality.§
Supplementary Table S3 provides an overview of the association between various frailty and functional status instruments and the remaining outcomes.
Abbreviations: ADL = Activities of Daily Living; DD = deceased donor; LD = living donor; Karnofsky = Karnofsky Performance Status; IADL = Instrumental Activities of Daily Living; OR = odds ratio; RR* = relative risk calculated from event data; SPPB = Short Physical Performance Battery; Unadj = unadjusted model; ¥ = comparison was inverted.
Graft Loss
There were 13 assessments of frailty that examined graft loss outcome among transplanted patients (Figure 4). These assessments measured all domains of frailty, with a primary focus on overall frailty, as determined by the Physical Frailty Phenotype, and the domain of sarcopenia. Frailty by the Physical Frailty Phenotype was associated with a 2-fold increased risk of graft loss. Frailty as determined by sarcopenia also showed an increased risk for graft loss when used as a categorical measure (n = 3) but not as a continuous one (n = 1). The remaining domains of frailty revealed no association with graft loss.

Forest plot of the association between frailty and graft loss.§
There were 7 assessments of functional status that examined graft loss. Functional status by level of assistance with ADL showed a 2-fold increased risk of graft loss (n = 2). Similarly, the point estimates for most assessments of Karnofsky and SF-36 physical functioning were above 1.0, suggesting a positive association between poor physical functioning and graft loss (Figure 5).
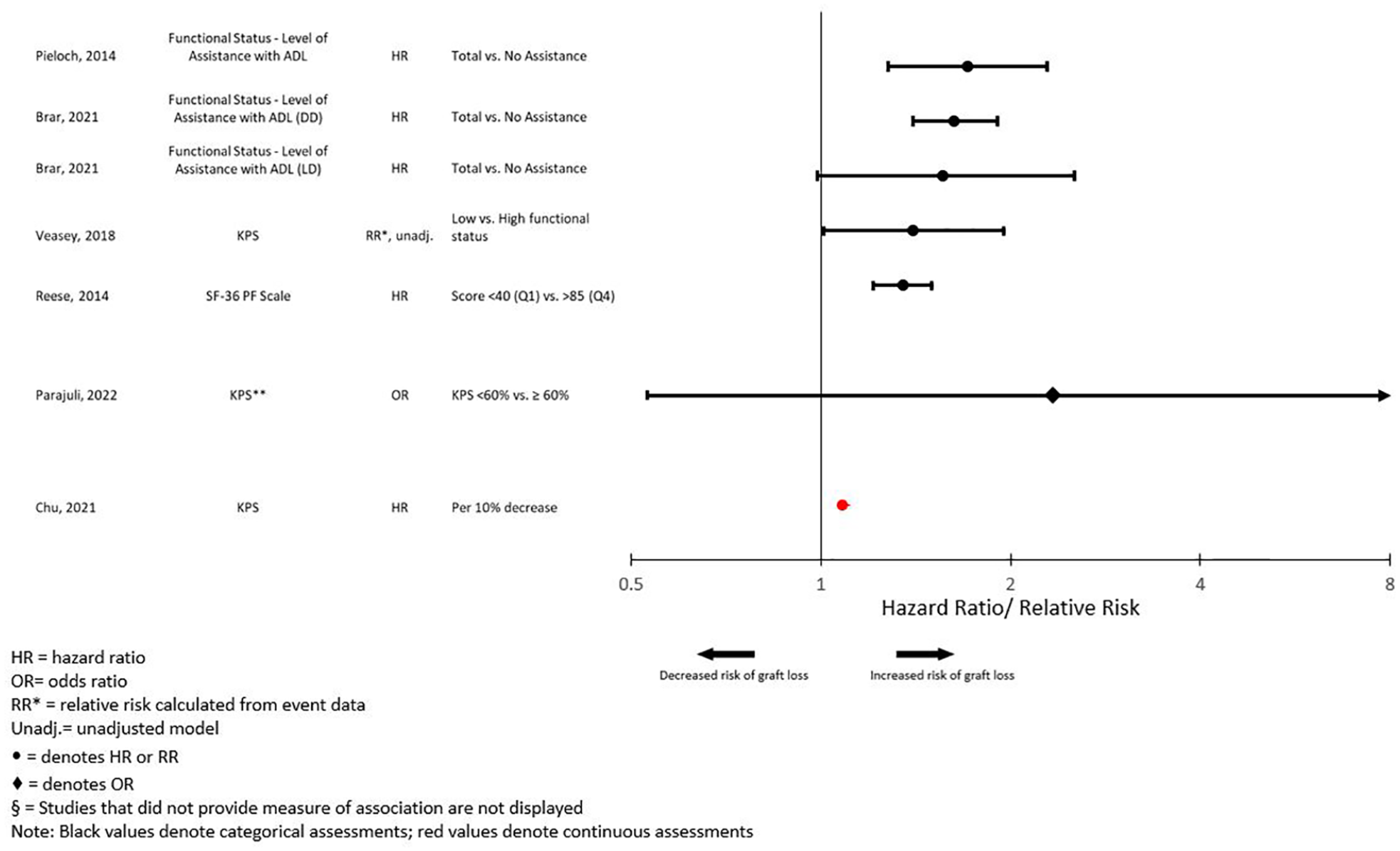
Forest plot of the association between functional status and graft loss.§
Hospital Readmission
The relationship between frailty and hospital readmission after transplantation was examined in 13 assessments across 5 studies. Various frailty instruments were examined and covered every domain of frailty. Among these, 9 assessments were examined categorically (Figure 6). For assessments measuring overall frailty, there was an increased risk for rehospitalization ranging from 2- to 4-fold among patients deemed frail prior to transplantation. When sarcopenia was examined, 2 of 3 assessments revealed a 4- to 7-fold increase in the risk of rehospitalization. A single assessment of strength found a 2-fold increased risk of rehospitalization among patients with weaker strength prior to transplantation. In contrast, frailty based on measurements of gait, physical activity, and fatigue were not significantly associated with rehospitalization. When frailty was examined as a continuous measure, only 2 of 4 assessments, which examined radiographically determined muscle attenuation prior to transplantation, found a statistically significant increased risk of rehospitalization after transplantation (Figure 7). Functional status was examined in 2 studies, with only 1 reporting significantly increased odds of rehospitalization among transplant patients with impaired functional status (Supplementary Figure S2). Finally, 6 assessments among 2 studies examined frailty and the risk of hospitalization while on the waitlist. Only 2 assessments found a statistically significant relationship.

Forest plot of the association between frailty as a categorical variable and rehospitalization.§
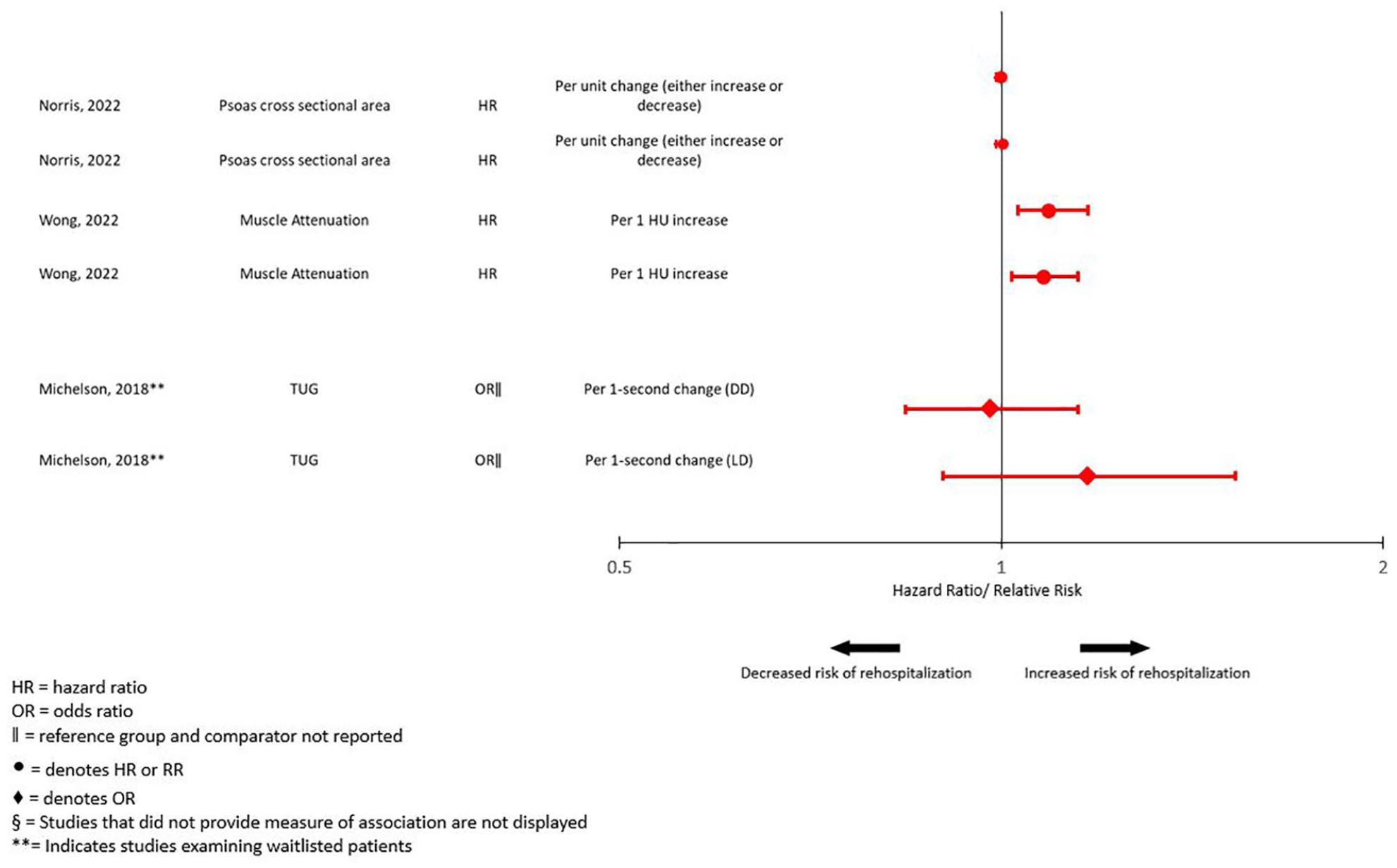
Forest plot of the association between frailty as a continuous variable and rehospitalization.§
Transplantation
The relationship between frailty and receiving a kidney transplant was examined in 8 assessments in 5 studies. Among these, 4 of the 8 assessments revealed a decreased likelihood (20%-61% reduction) of undergoing kidney transplantation among frail individuals (Figure 8). There were 4 assessments of functional status, with half reporting that impaired functional status was associated with a 16% to 26% decreased likelihood of undergoing kidney transplantation (Supplementary Figure S3).
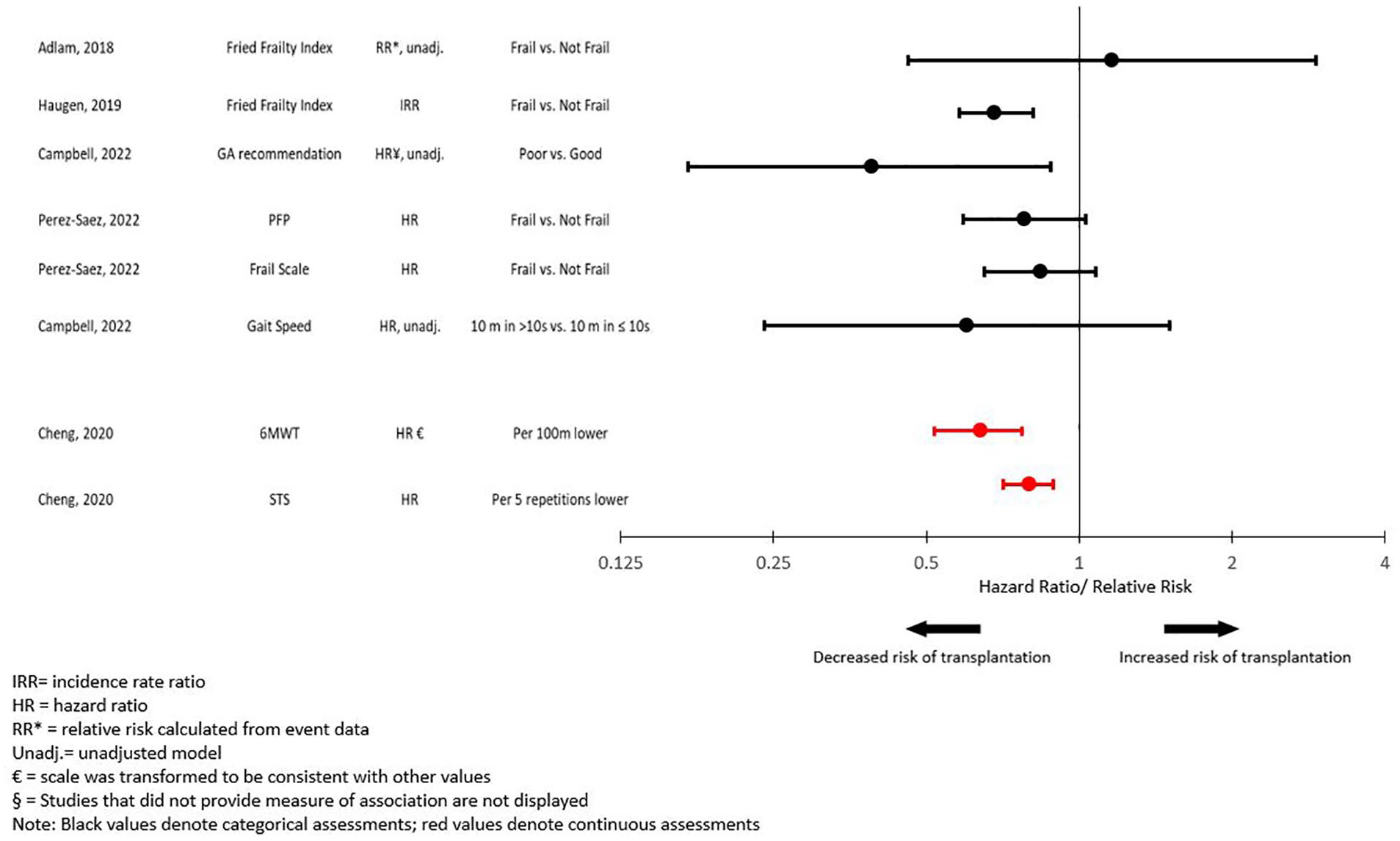
Forest plot of the association between frailty and transplantation.§
Delayed Graft Function
Frailty’s relationship with the occurrence of DGF post-kidney transplant was conducted through 10 categorical assessments (Supplementary Figure S4). Only 2 of 10 showed a significant association between frailty and DGF, with 1 study finding a 2-fold increased risk of DGF among patients identified as frail prior to transplantation, and another study finding an association between weight loss among transplant recipients prior to transplantation and decreased odds of DGF.
Three assessments examined functional status using Karnofsky and SF-36 physical functioning (Supplementary Figure S5). Two of these revealed an increased risk of DGF among patients with impaired functional status before transplantation.
Discussion
This systematic review identified 50 published studies using 36 unique instruments that examined the association between measures of frailty and functional status with key clinical outcomes in kidney transplant candidates. Both decreased functional status and frailty were associated with mortality. Similar trends were noted when examining graft loss and rehospitalization as outcomes. These findings reinforce the importance of considering frailty and functional status during the transplant evaluation process.
The magnitude of the effect of frailty on overall survival after kidney transplant is difficult to quantify. Given the heterogeneity of the studies included in this systematic review, we could not pool results nor perform a meta-analysis. However, the magnitude of the association of frailty with mortality in our study is in the same range as what our group has previously demonstrated for frailty in CKD patients 22 and what has been shown with diabetes pre-kidney transplant. 36 Therefore, the potential impact of frailty on kidney transplant outcomes and how to address this should be considered.
Although a growing number of studies have examined frailty’s impact on kidney transplant outcomes,6,8,37 there has been less focus on functional status. Our review adds to the available literature by summarizing the effects of pre-transplant frailty on relevant post-transplant outcomes. Our findings provide additional insights into the role of functional status in predicting adverse outcomes in transplant candidates, reinforcing its potential role as a prognostic factor and a possible assessment tool in the evaluation process.
Frailty has a long-reaching impact, not only affecting patients before surgery but also influencing an array of outcomes post-transplant.7,20,33-35,38-40 Studies have shown that the prevalence of frailty among kidney transplant candidates is nearly 20%.7,8,38 Kidney transplant guidelines highlight the need for studies to examine the utility of measuring frailty during the transplant evaluation process. 41 Despite the acknowledged importance of frailty in determining transplant eligibility, the use of standardized frailty assessment in clinical practice remains rare, suggesting a gap between its recognized importance and clinical implementation.11,22,42 Standardizing frailty measures would facilitate more consistent risk stratification, enabling clinicians to make more informed decisions regarding transplant eligibility, potentially improving recovery times and overall outcomes. It would also enhance the comparability of research findings and serve as a benchmark for quality improvement initiatives. This study advances the understanding of frailty and its interplay with kidney transplantation outcomes. Our work supports the initiative to develop and adopt validated, standardized frailty assessment tools by underscoring the absence of standardization in this field.
Furthermore, by identifying and addressing poor physical functioning and frailty before transplantation, health care providers can design and implement prehabilitation strategies specific for transplantation that may lead to improved outcomes.21,43 Identifying frailty and assessing functional capacity pre-operatively could offer opportunities to implement changes in approaches to care that have the potential to improve post-operative outcomes. Kidney transplant candidates generally have time to intervene with prehabilitation given the current waiting times for deceased donor kidney transplantation. 44 A pilot study by McAdams-Demarco examined center-based rehabilitation involving weekly physical therapy sessions on 5 transplant candidates. 21 Although the study reported improvements in overall health status and feasibility of the intervention, the small sample size and lack of control group limit the ability to draw definitive conclusions about its impact on post-operative outcomes such as hospital length of stay. 21 Although this preliminary work is hopeful, hard evidence is lacking on the effectiveness of such strategies in kidney transplant candidates. However, evidence from other surgical populations, such as colorectal, cardiac, and orthopedic surgery, suggests prehabilitation may improve post-operative outcomes, including reduced complications and shorter hospital stays.45-47 These findings indicate a potential for similar benefits in kidney transplantation. By focusing on improving patients’ strength, endurance, and physical functioning, implementing such programs could enhance outcomes after transplantation, but further research is needed to determine the efficacy of prehabilitation strategies in this specific patient population.
Although transplantation generally offers survival and quality of life advantages over remaining on dialysis, it is unclear whether there exists a threshold of frailty or diminished functional status beyond which the absolute risk of adverse outcomes is prohibitively high, and an individual should not receive a kidney transplant. The heterogeneity of frailty assessment tools and the lack of standardized cutoff points in the studies we reviewed, and the various other clinical factors which must be considered when evaluating an individual’s transplant candidacy would make it nearly impossible to define such a threshold. Even if there was an accurate, reliable, easy to implement assessment tool for frailty in transplant candidates, it is hard to see how it could be studied to determine one’s transplant candidacy in a prospective, controlled fashion. Observational prospective cohort studies where outcomes are stratified by frailty status could be informative, despite selection bias and confounding that are difficult to control for. They could help identify patients who may not benefit from transplantation due to excessive risk. As the age of waitlisted transplant candidates continues to grow, 48 frailty is likely to play an ever-growing role in transplant candidacy evaluation. Future research is needed to improve assessment tools and determine its impact on the risk-benefit balance of kidney transplantation.
Major strengths of our review are its size and broad scope. Our findings draw from a pool of 50 studies encompassing 668 103 patients. These factors increase the clinical applicability of our findings. In addition, our study investigated the impact of all frailty domains on various clinical outcomes, including the effect of functional status on adverse events, something previous systematic reviews have not addressed. Also, measurement methods were not restricted in this review. Therefore, numerous instruments measuring functional status and all the domains of frailty were included. Although our study provides valuable insights, it is not without limitations. The heterogeneity in the measurement instruments and study designs included in the review may limit the generalizability of the findings. Furthermore, the majority of studies originated from the United States, and we only included studies published in English, further limiting generalizability. It is important to note that there were variations in the study designs and assessment instruments across the included studies. Moreover, there were discrepancies in the definition of outcomes across studies. These factors introduce heterogeneity influencing the comparability of findings, and as a result, conducting a meta-analysis and pooling statistics could not be performed. In addition, many studies relied on secondary data sources such as registries, hospital records, and previous cohorts. This may have impacted the validity of data collection, assessment of exposure and outcomes, and may have led to selection bias in some of these studies.
Conclusion
This systematic review highlights the significant impact of frailty and decreased functional status on key outcomes in kidney transplant candidates, including mortality, graft loss, and rehospitalization. Our findings suggest that further studies are needed to evaluate the best instrument(s) to assess frailty and functional status, and importantly, interventional studies are needed to determine whether prehabilitation strategies can improve post-transplant outcomes in appropriate kidney transplant candidates.
Supplemental Material
sj-docx-1-cjk-10.1177_20543581241300777 – Supplemental material for Physical Frailty and Functional Status in Kidney Transplantation: A Systematic Review
Supplemental material, sj-docx-1-cjk-10.1177_20543581241300777 for Physical Frailty and Functional Status in Kidney Transplantation: A Systematic Review by Priscilla Karnabi, David Massicotte-Azarniouch, Shawn Marshall and Greg A. Knoll in Canadian Journal of Kidney Health and Disease
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by peer-reviewed grant from the Canadian Institutes of Health Research (grant #FDN-143239).
Ethics Approval
Not Applicable.
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Availability of Data and Materials
Not Applicable.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.