
Abstract
Background:
Living donor kidney transplantation (LDKT) has several advantages over deceased donor kidney transplantation. Yet rates of living donation are declining in Canada and there exists significant interprovincial variability. Efforts to improve living donation tend to focus on the patient and barriers identified at their level, such as not knowing how to ask for a kidney or lack of education. These efforts favor those who have the means and the support to find living donors. Thus, a Canadian Institutes of Health Research (CIHR)-organized workshop recommended that education efforts to understand and remove barriers should focus on health professionals (HPs). Despite this, little attention has been paid to what they identify as barriers to discussing LDKT with their patients.
Objective:
Our aim was to explore HP-identified barriers to discuss living donation with patients in 3 provinces of Canada with low (Quebec), moderate (Ontario), and high (British Columbia) rates of LDKT.
Design:
This study consists of an interpretive descriptive approach as it enables to move beyond description and inform clinical practice.
Setting:
Purposive criterion and quota sampling were used to recruit HPs from Quebec, Ontario, and British Columbia who are involved in the care of patients with kidney disease and/or with transplant coordination.
Patients:
Not applicable.
Measurements:
Semistructured interviews were conducted. The interview guide was developed based on a preliminary analytical framework and a review of the literature.
Methods:
Thematic analysis was used to analyze the data stemming from the interviews. The coding process comprised of a deductive and inductive approach, and the use of a qualitative analysis software (NVivo 11). Following this, themes were identified and developed. Interviews were conducted until thematic saturation was obtained. In total, we conducted 16 telephone interviews as thematic saturation was attained.
Results:
Six predominant themes emerged: (1) lack of communication between transplant and dialysis teams, (2) absence of referral guidelines, (3) role perception and lack of multidisciplinary involvement, (4) HP’s lack of information and training, (5) negative attitudes of some HP toward LDKT, (6) patient-level barriers as defined by the HP. HPs did mention patients’ attitudes and some characteristics as the main barriers to discussions about living donation; this was noted in all provinces. HPs from Ontario and British Columbia indicated multiple strategies being implemented to address some of these barriers. Those from Ontario mentioned strategies that center on the core principles of provincial-level standardization, while those from British Columbia center on engaging the entire multidisciplinary team and improved role perception. We noted a dearth of such efforts in Quebec; however, efforts around education and promotion, while tentative, have emerged.
Limitations:
Social desirability and selection bias. Our analysis might not be applicable to other provinces.
Conclusions:
HPs involved with the referral and coordination of transplantation play a major role in access to LDKT. We have identified challenges they face when discussing living donation with their patients that warrant further assessment and research to inform policy change.
What was known before
Rates of living donor kidney transplantation are declining. Current efforts focus on implementing educational interventions to address patient-identified barriers to living donation. A CIHR-organized workshop recommended that education efforts to understand and remove barriers should focus on health professionals instead as they play a crucial role in a patient’s decision to pursue living donation.
What this adds
We interviewed health professionals across 3 provinces of Canada with variable rates of living donor kidney transplantation. We report 6 themes that they perceive as barriers, most of which are easily modifiable. Our findings can help inform health delivery systems of targeted and effective interventions.
Introduction
Living donor kidney transplantation (LDKT) is associated with superior patient and graft survival when compared with deceased donor kidney transplantation.1-4 Those with LDKT experience lower rates of acute rejection, have earlier access to a transplant, and have an improved quality of life.2,5-12 Thus, there is considerable interest in increasing LDKT.4,11,13-18 Yet the overall rate of living donation in Canada is declining (16.8 per million population in 2007 to 15.2 per million population in 2016) and is 35% lower than several other Western nations.3,4,8,11,12 Furthermore, there exists significant interprovincial variability in LDKT rates. For example, in the provinces of Quebec (QC), Ontario (ON), and British Columbia (BC), <15%, 30%-40%, and 50-60% of the transplants done annually are from living donors, respectively. 3
Patient-identified barriers to LDKT, such as patients’ discomfort to approach potential donors and lack of knowledge, are well recognized.11,19-27 We conducted a systematic review and meta-analysis of educational interventions to address these barriers and noted that they were associated with a 2.5 higher odds of LDKT when compared with nonspecific education. 28 However, the quality across studies was mixed and we noted high risk of selection bias. Also, some of the more effective interventions are resource intensive and might not be sustainable at most centers.28,29 More importantly, it has been argued that shifting the burden of finding a donor to the patient has created an inequitable 2-tier system favoring those who have the social and financial means to learn this process and pursue LDKT.10,30 This has been systematically shown; a socioeconomic advantaged quartile of patients was 34% more likely to receive LDKT when compared with the most disadvantaged quartile. 31
Overall, less attention has been given to barriers stemming from the health professional (HP). These HPs include physicians, nurses, nurse practitioners, social workers, and other staff at dialysis and transplant centers who are involved in the care of patients with kidney disease and/or with transplant coordination. A Canadian Institutes of Health Research (CIHR)-organized workshop recommended that education efforts to understand and remove barriers should focus on HPs. 32 This is because the crucial role of HPs, especially nurses, in a patient’s decision to pursue LDKT is well recognized.13,33-41 It is also known that personal biases, lack of knowledge, and discomfort can lead to inconsistent and inexplicit recommendations, and that this may intensify inequity to LDKT especially in the disadvantaged populations.21,22,42-45 Previous studies have only focused on issues surrounding wait-listing and transplantation at the center- and system-level.43,46-54 When HP-level barriers to LDKT were examined, studies focused on nephrologists only42,55-57 and the input of frontline staff, such as dialysis nurses, was not captured. This is problematic due to a variety of reasons. First, decision-making on LDKT eligibility entails unique ethical, cultural, psychosocial, and medical uncertainties. Making this decision unilaterally may be reflective of an individual’s own perceptions and biases. Second, for nephrologists LDKT education may not be a priority given competing needs to educate on a myriad of other issues related to dialysis. 53 Physicians might think they are not accountable for transplant education.54,55 Last, education delivered by the physician might be ineffective.43,58
Given this, the aim of our study was to systematically explore HP-identified barriers to discussions of LDKT with patients in 3 provinces of Canada. We wanted to capture the input of those who are involved in the care of patients with kidney disease and/or with transplant coordination. We also aimed to explore if there are differences among HPs when informing their patients about living donation in 3 provinces of Canada with low, moderate, and high rates of LDKT.
Methods
Study Design
This is an interpretive descriptive study with the aim of developing a conceptual understanding of a phenomenon to inform clinical practice. 59 Interpretive description draws from various methodological approaches (grounded theory, ethnography, and phenomenology) to provide a basis upon which to analyze data that goes beyond description and is oriented toward theory development. Interpretive description rests on both naturalistic and constructivist epistemologies in emphasizing the central role of researchers in the interpretation of data; the latter not so much emerging by itself but rather stemming from decisions the researcher makes in generating findings.59,60 Thus, while interpretive description involves some form of theory development, it is in line with practical orientation.
Preliminary Analytic Framework: O’Neill et al’s Clinical Decision-Making Model
Interpretive description calls for the development of a preliminary analytic framework that will serve as theoretical scaffolding by guiding aspects of the study design, such as the elaboration of data collection instruments, while data analysis will take shape through the interplay between the empirical data and this preliminary framework.59,61 To understand what impedes HPs willingness or ability to engage in a discussion about LDKT with patients, a perspective around what shapes the decision-making process around assessing patients for referral and eligibility for LDKT, and the place discussions with patients occupy in that sense becomes useful. Thus, HP barriers to discussion need to be situated as part of the selection and evaluation of patients for LDKT, as well as how HPs perceive and define the barriers in that regard, particularly as they relate to discussing LDKT with patients. To that end, our preliminary analytical framework draws on aspects of O’Neill’s clinical decision-making model as found in Banning 62 and O’Neill et al63,64 and was adapted to issues pertaining to LDKT and HP-level barriers (Table 1). The main components related to clinical decision-making, according to this model, are as follows: (1) pre-encounter data which may include the role of guidelines, policies, procedures, prior knowledge, beliefs, assumptions about patients, and how risk is anticipated and controlled by HPs regarding LDKT; (2) situational and client modifications, that is interactions between HPs and patients, and the management of the patient’s care in particular environments (which may involve interactions and discussions related to LDKT) as well as organizational and resource issues; and (3) hypothesis generation, or the extent to which decisions are made on the basis of the patient’s condition or pattern recognition. With regard to LDKT, this pertains to what enters into the assessment and evaluation of patients and, in particular, how discussions with patients come into play. The aim thus becomes that of understanding how these 3 components interrelate with regard to HPs’ decisions in relation to LDKT and the manner in which discussions about LDKT with patients is enabled or inhibited as a result, and the place such discussions hold in assessing and referring patients for LDKT. Thus, our preliminary analytical framework drew on aspects of O’Neill’s clinical decision-making model and was adapted to issues pertaining to LDKT and HP perceived barriers (see Table 1).
O’Neill’s Clinical Decision-Making Model Adapted to LDKT and Health Professional–Identified Barriers.
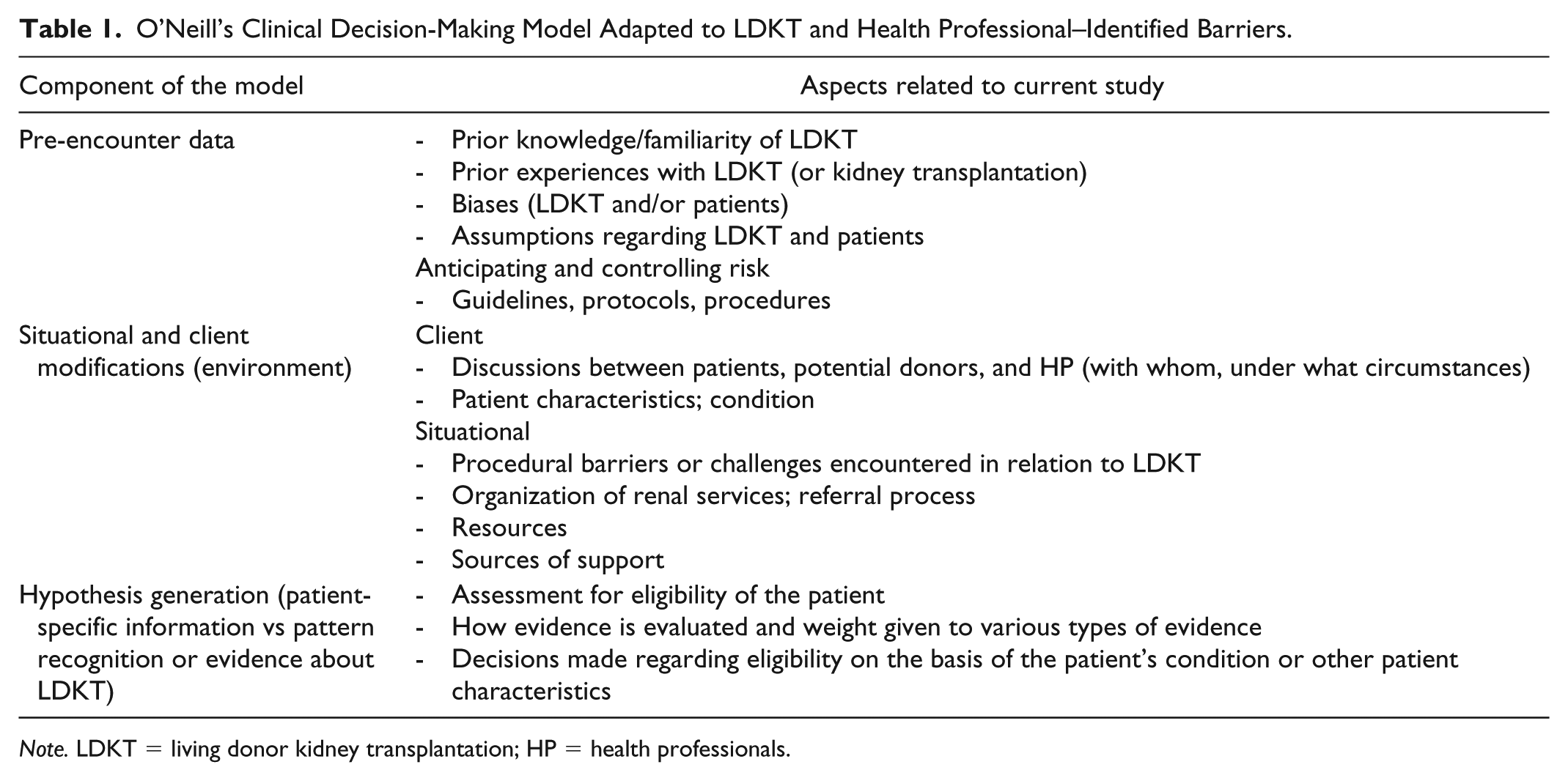
Note. LDKT = living donor kidney transplantation; HP = health professionals.
Sampling and Recruitment
A directory of dialysis centers, and transplant and nephrology clinics across Canada was used to create a recruitment list. Participants were selected by contacting the centers directly and based on referrals and were contacted via a letter of invitation (email or mail) or by telephone. Two sampling strategies were used to recruit potential participants. 65 The first step involved purposive criterion sampling to ensure the input of key stakeholders, such as transplant coordinators, dialysis nurses, and general nephrologists, was captured. Exclusion and inclusion criteria, as put forth in Table 2, were developed and used to select potential participants. We wanted to include the opinions of those who are involved in transplant coordination. Our focus in recruiting participants was HPs working either in chronic kidney disease clinics, dialysis centers, or within programs that combined these two with transplantation. Also, to ensure that key demographics were represented, this study resorted to a quota sampling method. We wanted to ensure that a minimum percentage of participants with certain characteristics, summarized in Table 3, were represented in the sample. 65 The recruitment process is outlined in a consort diagram (Figure 1). Participants who did not respond were contacted up to 3 times. Interviews were conducted over the telephone usually in the office setting by a senior qualitative researcher (K.C.).
Selection Criteria for Recruitment of Participants.

Targeted Sampling Quotas and Percentage of Participants Who Were Recruited.

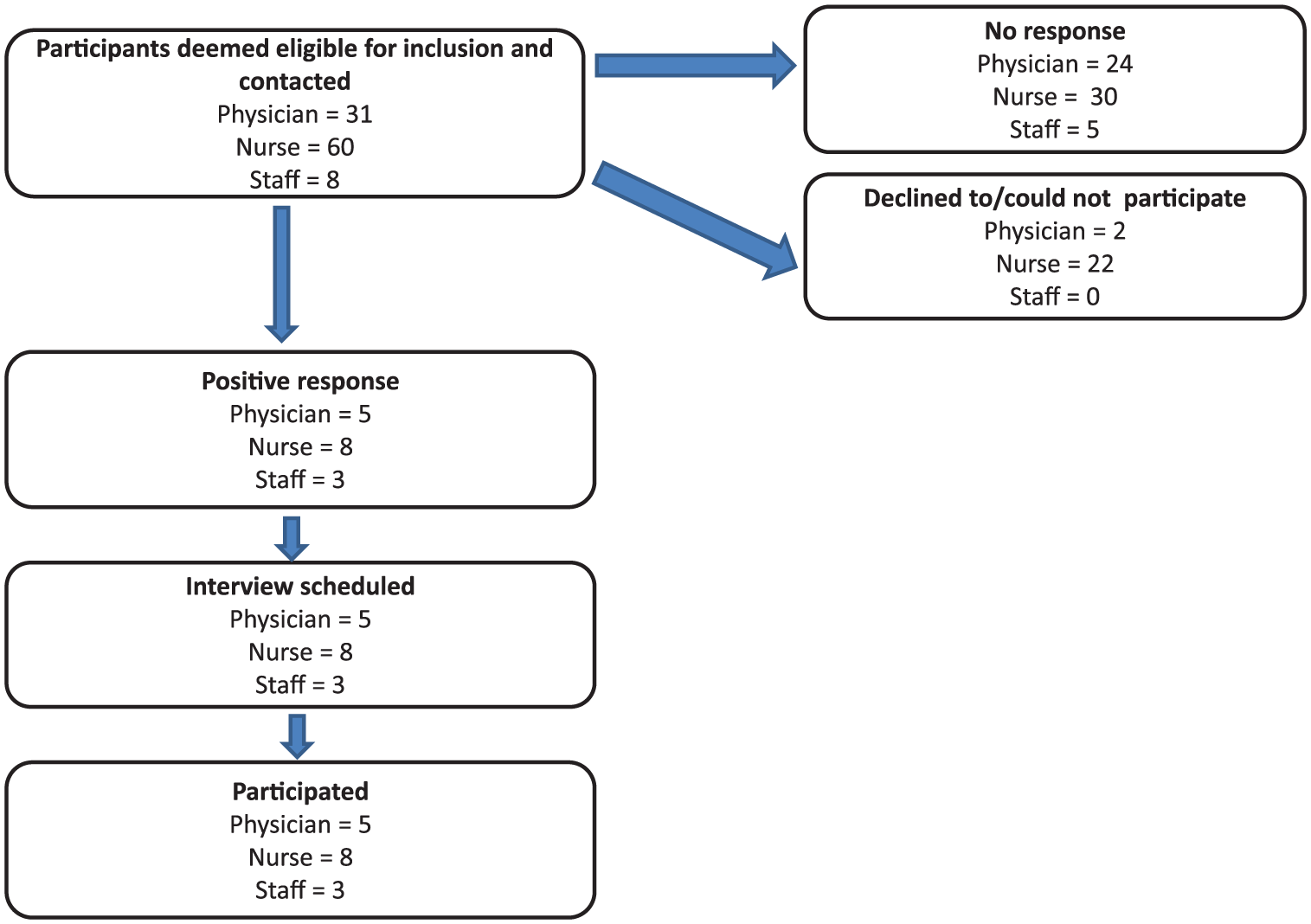
Consort diagram of recruitment process of participants per province.
This study was approved by the local institutional review board and written consent was obtained from all participants; participation was voluntary. Participant information procured was coded and de-identified by order of interview and province of work. The qualitative researcher (K.C.) who conducted the interviews labeled the interview tape with a code number and transcribed it. Any information in the transcript that identified the participant was removed. Upon receiving the transcript, the audio recording was destroyed. The study files were kept in paper or electronic format in secure and locked filing cabinets.
Data Collection
We conducted 16 semistructured telephone interviews with participants working in three Canadian provinces: 8 in QC, 4 in ON, and 4 in BC. All interviews were audio recorded, transcribed verbatim, and conducted between October 2017 and March 2018. Recordings lasted between 30 and 45 minutes. All transcriptions were verified for accuracy by directly comparing voice and transcription files. Only 1 interview was repeated, as per the participant’s request. Interviews were conducted over the telephone usually in the office setting by a senior qualitative researcher (K.C.). On the basis of aspects of the initial analytical framework as well as a review of the literature, an interview guide was developed and covered the following topics: (1) familiarity, knowledge, and interest with LDKT; (2) potential biases surrounding patients and LDKT; (3) participants’ involvement and comfort level with LDKT; and (4) final thoughts regarding LDKT.
Data Analysis
Thematic analysis66,67 was used to analyze the data stemming from interviews using an inductive approach. 68 To do this, potential and emerging themes were contrasted with the preliminary framework to develop an explanatory framework around the barriers to discussion about LDKT in the following manner: the coding process comprised a deductive and inductive approach and was accompanied by the development of a preliminary codebook informed by elements of the interview data, the preliminary framework, and a review of the literature. Codes that emerged from the data were then added to the codebook.
The coding process involved the use of a qualitative analysis software (NVivo 11). Following the coding process, codes were clustered to develop initial themes, which were then refined so as to ensure their internal and external heterogeneity. 69 Memoing throughout the coding process served to facilitate the clustering of codes and guide theme development. 70 More specifically, memoing served to establish relationships between initial ideas stemming from the coding process as to how various barriers impede discussions to occur between patients and HPs. Narrative summaries for each interview were also developed and accompanied the coding process as well as guided theme development.
Once coding was completed, codes were then grouped into categories. This took shape as codes were clustered such that they shared common ground in relation to the research question, the phenomenon under study, and aspects of the preliminary framework that is perceived facilitators and impediments to discussing LDKT with patients. This enabled theme development. Thus, theme identification and development followed the stages as laid out by Vaismoradi and colleagues. 67 These stages included (1) classification or typification (the classifying of codes that share typical similarities); (2) comparison and revision of codes; and (3) the sorting of codes under labels (taken from the content of the transcript but which entailed more abstraction than the classification phase). Data were coded by a qualitative researcher (K.C.) and subsequently verified by a second senior researcher (J.F.F.).
Interviews were conducted until thematic saturation was obtained. Francis et al’s 71 approach was drawn upon to assess thematic saturation. An initial sample of 10 interviews was established. Additional interviews were conducted until saturation was achieved, that is until no new significant changes were made to the codebook (Supplementary Table 1). 72 A saturation table or grid was designed around the codebook as a way of keeping track of changes to the codebook. 73 This procedure was followed in accordance with the quota sampling strategy to ensure the representativeness of certain characteristics. Tong et al’s 74 consolidated criteria for reporting qualitative research were drawn upon to ensure the quality of the methods used for this study were robust.
Results
Overall, 81% of the participants were female, 31% were physicians, 50% were nurses, and 19% described themselves as other staff (Table 3).
Themes
Six predominant themes emerged from what HP identified as barriers to discussing LDKT with their patients (Figure 2). Table 4 describes specific quotes supporting each theme.

Themes and subthemes around health professional (HP)-level barriers to discussions about living donor kidney transplantation (LDKT) with patients.
Illustrative Quotes for the Themes Identified in This Study of Health Professional–Identified Barriers to Living Donor Kidney Transplantation by Province (Efforts Implemented to Alleviate Some Recognized Barriers Are Highlighted).

Lack of communication between transplant and dialysis teams
Certain organizational characteristics were thought to impede early discussions with patients about LDKT. Dialysis and transplant teams were viewed as separate entities. Communication between them was deemed as sporadic and insufficient, and to only occur during a crisis situation. HPs working in dialysis felt not being sufficiently updated on the progression of recipient’s and donor’s evaluation. The transplant team was likened by 1 participant to a “black box” of which the dialysis team was excluded (14-QC). This hindered the possibility for HPs in the referral center to engage in discussions about LDKT. In addition, establishing the donor evaluating team as a separate entity was viewed as problematic, especially when a majority of donors that initiate the process have an excellent relationship with the recipient (08-ON).
Participants from ON and BC mentioned efforts being made to alleviate this separation via coordinators and protocols, and that this translated into improved communication. Yet even in the midst of such efforts, the transplant team and the transplant coordinator remained perceived as being best suited to engage in detailed conversations about LDKT, while more general conversation are left to the referral team. Thus, the difficulty in attenuating dialysis and transplant teams/centers as separate entities hinders the possibility for HPs in the dialysis centers to become part of the process of pursuing a LDKT.
Absence of referral guidelines
The current referral process surrounding LDKT was deemed as encumbered by numerous tests and delays. Some felt that if these tests are done ahead of time it delays the referral. Disorganization was another characteristic used to describe the referral process, as many pointed to variability in the cutoff and tests required prior to referral for transplantation. Part of this is deemed attributive to dialysis and transplant teams remaining separate entities. All this contributes to confusion and decreased early discussion with patients about LDKT.
As efforts to alleviate this, many mentioned that the focus should be on establishment of referral guidelines at the provincial level to streamline the referral process. In the absence of such guidelines, the potential for early discussions about LDKT is curtailed on account of the confusion that characterizes the referral for transplantation; a confusion stemming from persistent variations among centers. In ON this constitutes a core effort to facilitate LDKT. Some said that variations will remain in the application of these guidelines, but as one participant said, “You can never . . . I don’t think you can ever fully standardize something where human beings are involved in making decisions but you can still . . . there’s definitely room there” (08-ON). Another option put forth was early referral of the patient to the transplant center, thus situating the role of early discussions with patients about LDKT to the transplant team.
Role perception and lack of multidisciplinary involvement
The manner in which some participants perceived their role and that of others represented another barrier. Many HPs did not consider it to be their role to discuss LDKT with patients, but rather that of the transplant team or the nephrologist. Thus, they forego this discussion as they perceived limits to the appropriateness of initiating a LDKT discussion, given their expertise, ability, and role expectations. Some participants nonetheless considered it necessary to raise the issue of LDKT with patients whenever possible.
The extent to which multidisciplinary teamwork invites frontline workers to alter their role perception was deemed crucial to engage in discussions about LDKT with patients. This is to say whether HPs viewed discussions with patients about LDKT as outside their role to one in which such discussions were thought of as key to their role. Participants from BC alluded to teamwork and opportunities for informal discussions by frontline staff as central to facilitating LDKT. This was accompanied by a change in role perception and increased familiarity and comfort in raising this topic with patients by every member of the team. The notion of a nephrologist working alongside other HPs, while retaining a central role, was viewed as conducive to facilitating discussions about LDKT.
HP’s lack of information and training
HP lack of comfort in communicating the risks and benefits of LDKT to patients emerged as a barrier, particularly in QC. This was attributed to lack of training and knowledge regarding LDKT, and lack of resources and up to date information. A living donor coordinator working in QC pointed out that the existence of strict criteria for donor assessment tends to be inflated among HP in dialysis centers due to the lack of knowledge and comfort (02-QC). HPs at the predialysis phase lack the necessary information and knowledge to address patients’ concerns, which were said to revolve around the risks for the donors. Some participants indeed admitted to feeling discomfort discussing LDKT with patients, in particular issues surrounding finding a donor. Also, the existence of strict criteria for donor assessment tends to be inflated among HPs at dialysis centers. Thus, in overestimating the risks of LDKT and compounded by their own sense of lacking the information necessary to address patients’ concerns, HPs refrain from engaging in this conversation.
On the contrary, in ON and BC participants reported that discussions with patients not only occur earlier but are characterized by presenting patients with the evidence surrounding LDKT, dispelling any myths they may have had and offering support. Such discussions become integral to the referral process as the patient’s willingness to get a transplant becomes thought of as paramount to that process. At the same time, it is important to note that this lack of comfort and knowledge discussing LDKT with patients was mentioned by one participant in ON (16-ON). Also, the need for continued education, frequent discussions, and review of data was mentioned to continue to reinforce the benefits of LDKT, especially when there is a rare occurrence of a bad donor outcome (06-BC). A participant from QC reiterated this interest in increasing training in how to discuss LDKT with patients; even expressing willingness on their part to organize such a session themselves (07-QC).
Negative attitudes of some HPs toward LDKT
Participants interviewed in this study expressed enthusiasm for LDKT, although a few participants, most notably in QC, mentioned some HPs’, in particular nephrologists’, attitude against LDKT as an impediment. One participant said, And we have doctors who do not believe in transplantation, in general. Then we’re going to have a lot more trouble getting live donors to patients in those centers. . . . I think it has a lot to do with the mentality among some doctors, whether they are old school or of the new school. The new school is more . . . younger doctors are more proactive in terms of encouraging living donation. The old guard, maybe a little less. (03-QC)
The positive attitude toward LDKT in ON and BC, both among nephrologists as well as other HPs, was propelled by efforts to widen the eligibility of patients, which has led to increased emphasis on early discussion and referral. Participants attributed this to an aggressive “culture change” with the aim of rendering transplant, in particular LDKT, as the gold standard in treatment of patients with renal disease. In ON, potential recipients were described as being identified upon the slightest possibility as to their eligibility for LDKT. In BC, discussions with patients’ occurred earlier and centered on presenting evidence and offering support.
Patient-level barriers as defined by HPs
HPs’ own accounts of encounters with patients reflected a propensity to pinpoint patients’ attitudes and characteristics as the main barrier to discussions about LDKT. This was noted in all provinces. HPs mentioned barriers with respect to cultural background, psychosocial issues, language barriers, belief systems, and age. These rendered discussions with patients difficult. Many described that there is more willingness to convince younger patients to resort to living donation. Education sessions tailored to specific cultural groups were said to have been developed. Also an increasingly heterogeneous patient population was viewed as adding difficulty to efforts aimed at standardizing discussions with patients. Some mentioned that patients who are overenthusiastic as a problem due to engendering unrealistic expectations, and sometimes leading to a potential loss of motivation in pursuing LDKT. In another instance, some participants went so far as to wonder if an increase in deceased donors served as a disincentive for patients to find a living donor (01-BC; 02-QC).
Most mentioned placing the bulk of the responsibility on patients. Patients were portrayed as fearing to approach potential donors and not knowing how to formulate their request. Some described instances where patients did not inform family and friends of their renal disease, even though they are being called upon to act as spokespersons or advocates on behalf of the patient. Participants mentioned that patients are oriented toward tools aimed at helping them find a donor and provided support, but they do not play a direct role in the process of finding a donor.
Potential Causes of Disparity in LDKT Rates
Although not recognized by HPs, we noted significant interprovincial variations in efforts to increase LDKT (Table 5). Participants from regions with moderate and high rates of LDKT repeatedly mentioned multiple initiatives in their regions (comments in bold in Table 4). HPs from ON mentioned strategies that center on the core principles of provincial-level standardization, while those from BC center on engaging the entire multidisciplinary team and improved role perception. In addition, HPs mentioned several efforts to improve communication between treating teams and continued education of frontline staff. The efforts in BC are so immense that one participant said, “I’m not really sure how much more we need because over all at this program, everybody’s really very involved and we all believe in the process so, it’s not a hard sell for us” (06-BC). We noted a dearth of such efforts in QC. One participant mentioned the ongoing nursing crisis, 75 “The transplant nurses feel very stressed and overwhelmed with the volume of their work” (14-QC). However, efforts around education and promotion, while tentative, have emerged.
Efforts Mentioned by Health Professionals Being Undertaken to Improve Living Donor Kidney Transplantation.

Discussion
In this qualitative analysis, we have identified several themes that HPs perceive as barriers to discussion about LDKT. These include lack of communication between treating teams, absence of referral guidelines, lack of multidisciplinary involvement, poor role perception of frontline staff, and lack of information and training leading to discomfort. One concerning theme pertaining to poor attitudes of some referring centers toward LDKT also emerged. A final theme pertained to HP’s perception of several patient-level barriers, which renders discussions about LDKT challenging.
Previous work has examined system- and center-level barriers to LDKT on a macroscopic level and predominantly in the United States.56,76-78 Three studies have asked physician’s input on this subject42,55,57; of these, only one was a qualitative study. 42 By including other members of the team involved in transplant referral and coordination in our study, we have identified some important and modifiable barriers. The first 4 themes are easily modifiable. There are several ways to increase communication between treating teams and education of those involved in this process; some are outlined in Table 5. Centers ought to engage the entire multidisciplinary team in early discussions with patients related to LDKT. This will empower all HPs, improve their role perception, and enhance their knowledge, skills, and competencies.34,42,50,51 This is being done quite effectively in BC. Standardizing the referral process is a bit challenging as there is considerable amount of heterogeneity in the ideologies and preferences of centers and physicians.42,79,80 It is known that even when policies are created, transplant professionals will deviate. 79 However, some level of standardization should be implemented to guide referring centers.
The last 2 identified themes merit further discussion. HPs poor attitudes toward LDKT are likely compounded by their beliefs and recent literature of increased long-term medical risks post donation. 81 Hindsight bias after witnessing poor outcomes in some patients may contribute to this barrier. 82 Some have suggested that hindsight bias can be alleviated using the adaptive learning approach, continuously updating knowledge structures and prospectively experiencing the success of LDKT in different types of individuals. 82 Last, the propensity of the HP to locate the problem with the patient is a universally described barrier in the field of transplantation.36,42,43,48,52,54-56 This contributes to disparities and inequities in LDKT among vulnerable groups of patients and this theme was identified even by participants from ON and BC. Measures to address these are needed to ensure equity in LDKT.
The biggest strength of our study was that we conducted it in 3 different provinces of Canada with variable rates of LDKT and included the input of key frontline personnel that has not been previously captured. We identified that HPs perceive barriers to LDKT discussion even in regions with high rates of LDKT. The qualitative approach adopted in this study enabled a detailed and granular examination of HPs’ opinions compared with that offered by a quantitative approach. We used robust methodology and the interviews were conducted by a senior qualitative researcher with limited background in transplantation reducing the potential for moderator bias. The following limitations, however, need to be acknowledged. Our analysis may not be applicable to all provinces; although, QC, ON, and BC together comprise 75% of Canada’s population, and performance in these provinces significantly influences the country’s overall transplant results. 4 Our study may be limited by social desirability and selection bias. It is likely that only those interested in LDKT would have agreed to participate. We did not pilot test the interview; however, after encountering problems with interviewing one participant, we made appropriate changes to the interview guide. It is possible that other relevant barriers considered unfit to the framework were inadvertently missed out. We did not perform member-checking, although this has been criticized for jeopardizing the internal validity of the study given the risk of participants changing their perspective following the interview.83,84
Despite this, our findings are relevant and have important implications for policy makers and organ procurement organizations in Canada. There is poor understanding of what HPs perceive as barriers and lack of evidence to ensure they are alleviated. We note predominance of these barriers in the province with the lowest rates of LDKT and likely directly contributing to this imbalance, although a quantitative study is indicated and is our next step. We believe that quantifying these themes will inform targeted and effective interventions to address barriers to LDKT at the level of the HP, and perhaps the health-delivery systems as well.
In conclusion, we have identified 6 important themes that HPs perceive as barriers to LDKT discussion with their patients. These themes were noted across 3 different provinces in Canada at variable rates, with differential efforts implemented to address them that appear to correlate with the rates of LDKT in the respective province. HPs involved with the referral and coordination of transplantation play a major role in access to LDKT. They have unique challenges that warrant further assessment and research to inform policy change and interventions.
Supplemental Material
Supplementary_Appendix_1_Codebook-LDKT – Supplemental material for Health Professional–Identified Barriers to Living Donor Kidney Transplantation: A Qualitative Study
Supplemental material, Supplementary_Appendix_1_Codebook-LDKT for Health Professional–Identified Barriers to Living Donor Kidney Transplantation: A Qualitative Study by Shaifali Sandal, Kathleen Charlebois, Julio F. Fiore, David Kenneth Wright, Marie-Chantal Fortin, Liane S. Feldman, Ahsan Alam and Catherine Weber in Canadian Journal of Kidney Health and Disease
Footnotes
Acknowledgements
The authors would like to sincerely thank the 16 individuals who participated in this study.
Ethics Approval and Consent to Participate
This study was approved by the local institutional review board (McGill University Health Center Research Ethics Board and the CIUSSS-OMTL).
Consent for Publication
All authors reviewed the final manuscript and provided consent for publication.
Availability of Data and Materials
Data and materials may be made available upon written request to the corresponding author.
Author Contributions
Sandal: Involved in study conception and design, analyzed and interpreted data; drafted and revised the article; provided intellectual content of critical importance; and approved the final version. Charlebois: Involved in study design, conducted the interviews, analyzed and interpreted data; drafted and revised the article; provided intellectual content of critical importance; and approved the final version. Fiore: Involved in study design, analyzed and interpreted data; revised the article; provided intellectual content of critical importance; and approved the final version. Wright: Involved in study design; revised the article; provided intellectual content of critical importance; and approved the final version. Fortin: Analyzed and interpreted data; revised the article; provided intellectual content of critical importance; and approved the final version. Feldman, Alam, and Weber: Involved in study conception and design; revised the article; provided intellectual content of critical importance; and approved the final version. All authors have participated sufficiently in the work to take public responsibility for appropriate portions of the content.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported using an education grant from Amgen Canada to promote efforts to increase living donor kidney transplantation. The funding organizations had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; and preparation, writing, review, or approval of the manuscript.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.