
Abstract
Purpose of review:
Primary focal segmental glomerulosclerosis (FSGS) is the most common cause of nephrotic syndrome in adults. Glucocorticoids have been evaluated in the treatment of primary FSGS in numerous retrospective studies. Evidence suggesting a role for including calcineurin inhibitors (CNIs) in early therapy remains limited. The aim of this study was to systematically review the literature examining the efficacy of CNIs in the treatment of primary FSGS both as first-line therapy and as an adjunctive agent in steroid-resistant patients, with respect to remission in proteinuria and renal survival.
Sources of information:
PubMed and EMBASE were searched from inception to August 2014 for prospective controlled trials, and case-control and cohort studies.
Findings:
After systematically applying our inclusion criteria, a total of 152 titles and abstracts were identified. Six randomized controlled trials and 2 cohort studies were reviewed. Three randomized controlled trials compared CNIs with placebo or supportive therapy. The pooled relative “risk” of proteinuria remission associated with cyclosporine was 7.0 (95% confidence interval, 2.9-16.8) compared with placebo/supportive therapy. There was very low heterogeneity among these studies with an I-squared of 0%. Three studies compared CNIs with another immunosuppressive agent. All prospective trials were conducted in patients with primary FSGS deemed steroid-resistant.
Limitations:
The relatively small number of included studies and their heterogeneity with respect to treatment protocols, and possible publication bias, limit conclusions drawn from this systematic review.
Implications:
The efficacy of CNIs has been evaluated in steroid-resistant primary FSGS patients. There is no evidence supporting their role as first-line therapy. Further studies are needed to determine this role.
What was known before
CNIs in combination with glucocorticoids may increase the likelihood of complete or partial remission of proteinuria among individuals with steroid-resistant idiopathic FSGS.
What this adds
This study highlights the current gaps in the FSGS literature regarding first-line treatment. This review is the first to include a meta-analysis pooling the available evidence in steroid-resistant primary FSGS comparing cyclosporine to supportive therapy or placebo.
Why is this review important
This review provides a comprehensive summary of the existing literature on the immunosuppressive treatment for primary focal segmental glomerulosclerosis. This review is the first to include a meta-analysis pooling the available evidence comparing cyclosporine with supportive therapy or placebo. This study also includes a systematic critical appraisal of the internal and external validities of each reported study using recognized tools.
What are the key messages
There are important knowledge gaps pertaining to the treatment of primary focal segmental glomerulosclerosis. The existing evidence suggests that calcineurin inhibitors in combination with glucocorticoids may increase the likelihood of complete or partial remission of proteinuria among individuals with steroid-resistant primary focal segmental glomerulosclerosis.
Implications for future research
Further studies are needed to determine the role of calcineurin inhibitors as first-line therapy in primary focal segmental glomerulosclerosis. Good quality observational studies would be particularly suitable to measure the effect of calcineurin inhibitors on renal survival in steroid-naive focal segmental glomerulosclerosis population.
Introduction
Idiopathic focal segmental glomerulosclerosis (FSGS) is one of the most common causes of the nephrotic syndrome in adults, with an increased incidence over the last 3 decades, especially in African Americans. 1 FSGS lesions have been reported in up to 35% of patients who have undergone a kidney biopsy for nephrotic syndrome. 2 Primary FSGS represents 2.3% of patients with end-stage kidney disease (ESKD) in North America. 3
Patients with FSGS may benefit from immunosuppressive therapy. Current Kidney Disease: Improving Global Outcomes (KDIGO) guidelines suggest immunosuppression with high-dose prednisone as first-line therapy in patients with clinical features of the nephrotic syndrome, with low quality of evidence. 4 Indeed, glucocorticoids were evaluated several decades ago in primary FSGS in observational studies; the evidence supporting glucocorticoid therapy in FSGS is based on small observational cohorts of patients (n < 100) with inadequate statistical power for adjustment for potential confounders.5-8 Calcineurin inhibitors (CNIs) have been studied more recently in steroid-resistant primary FSGS, 9 but the evidence supporting their use in the initial therapy for FSGS is of very low quality, and mainly based on small observation cohorts.10,11 A Cochrane systematic review performed in 2008 concluded, based on the results of 3 randomized controlled trials, that adult patients with primary FSGS treated with cyclosporine in combination with low-dose oral prednisolone are more likely to achieve partial remission than patients treated with symptomatic treatment or prednisolone alone. 12 A pooled meta-analysis of data was not performed in this review. Braun and colleagues 12 highlighted the small number of patients treated in trials pertaining to primary FSGS.
The purpose of this systematic review was to summarize the existing evidence regarding the effectiveness of CNIs for the treatment of primary FSGS, both as first-line therapy and as an adjunctive agent in steroid-resistant patients. The search strategy focused initially on the most relevant renal outcome, renal failure; however, articles describing the effectiveness of CNIs in achieving remission in proteinuria were also reviewed.
Methods
Data Sources and Searches
EMBASE and PubMed were electronically searched from their inception dates (EMBASE from 1974 and PubMed from 1966) to August 2014. We initially searched each database for “glomerulosclerosis, focal segmental” AND (“cyclosporine” OR “tacrolimus”) AND (“renal insufficiency” OR “kidney failure, chronic”). These terms were selected using the PICO (Population Intervention/exposure Comparison Outcome) strategy. We then broadened the search strategy by searching for “glomerulosclerosis, focal segmental” AND (“cyclosporine” OR “tacrolimus”) due to a low number of potentially relevant citations identified in PubMed. The Cochrane Library was also searched for the presence of systematic reviews on primary FSGS, and results were compared with our searches. We also reviewed related articles and bibliographies of relevant articles.
Inclusion Criteria
Inclusion and exclusion criteria
Studies that described use of CNIs in patients with primary FSGS, including randomized and/or controlled trials, case-control studies, and cohort studies, were included. Case reports or case series were excluded due to absence of a control or comparison group. Editorials, clinical guidelines, commentary, letters to the editor, and meeting reports were also excluded. We restricted results to human studies published in English. A single individual (L.-P.L.) performed the literature searches and the study selection.
Comparison groups had to include any of the following: a control group receiving supportive treatment (ie, no immunosuppression), placebo or no treatment group, or a group receiving another agent of interest (eg, if the intervention was a CNI, the comparison might be mycophenolate mofetil [MMF]). The outcome of interest for an article retained to be reviewed was clinical efficacy of the immunomodulatory treatment; this could be measured or defined in several ways: mortality, renal survival (or time to ESKD), proteinuria remission rate (partial and complete), and renal function (estimated glomerular filtration rate [eGFR]).
Randomized controlled trials were reviewed and their methodology critically appraised using the Cochrane Collaboration’s tool for assessing risk of bias. 13 This risk of bias tool comprises 6 categories of bias: selection bias (random sequence allocation/concealment of allocation), performance bias (blinding of clinicians and participants), detection bias (blinding of participants and outcome assessors), attrition bias (intention-to-treat analysis), reporting bias (selective outcome reporting), and other bias. All categories focus on the internal validity of the study. External validity (generalizability) and precision (free of random error) were separately assessed. Retrospective studies were reviewed and their methodology critically appraised using the Newcastle-Ottawa quality assessment scale. 14 This tool was developed to assess the quality of nonrandomized studies in meta-analyses (case-control and cohort studies). It focuses on 3 domains to assess study internal validity: the selection of the study groups, the comparability of the groups, and ascertainment of exposure/outcome. External validity and precision were also separately assessed in retrospective studies.
Meta-analysis
A meta-analysis was performed for studies analyzing the efficacy of CNIs (with or without low-dose prednisone) versus placebo or supportive therapy.9,15,16 For each study, we estimated the risk ratio comparing CNI treatment with controls. The primary outcome was presence of partial or complete remission at 6 months of active therapy to use data of all studies (results at 1 year were not available for all studies). We then performed a meta-analysis to pool relative risks of remission across all 3 studies. Of note, the definition of complete remission was very similar in all studies, whereas definitions of partial remission had variability between studies but implied a reduction in proteinuria. We used a random effects model which accounts for random error and interstudy variability to estimate the pooled effect measures with 95% confidence intervals. We calculated the Higgins I-squared statistic that provided a percentage of variance between studies that is attributable to heterogeneity (ie, not to chance).
Results
Search Results
Our literature search with appropriate filters yielded 152 citations. We excluded 136 citations because screening of title/abstract did not meet our inclusion criteria, or satisfied one of our exclusion criteria. Two articles17,18 were further excluded because they were unable to be retrieved by our librarian (Figure 1): the first article was an open randomized controlled trial from India comparing treatment with cyclosporine plus oral prednisolone with intravenous (IV) methylprednisolone, and the second article was an open randomized controlled trial from Italy comparing IV methylprednisolone/oral prednisolone plus chlorambucil with no specific treatment. A total of 14 articles were reviewed in detail. Of these, 6 were excluded because they did not meet inclusion criteria on closer examination and 8 articles were reviewed for quality assessment and included in this systematic review.

Flowchart for literature search and article selection.
Study Characteristics
Table 1 summarizes the characteristics of all included studies. There were 6 randomized controlled trials and 2 retrospective cohort studies. Studies were of varying sizes, ranging from 28 to 138 patients. All studies included patients with biopsy-proven FSGS, but 2 also included patients with minimal change disease. Most studies included patients with any degree of proteinuria; only 2 studies used the more stringent entry criterion of nephrotic syndrome, which includes hypoalbuminemia, hyperlipidemia, and presence of edema. Most studies excluded patients with substantial renal insufficiency (eGFR < 45 mL/min/1.73 m2); only 1 retrospective study included patients with any eGFR at baseline. The studies varied considerably in the demographics of the patients included, especially with respect to age; 1 study included exclusively children and 3 studies exclusively adults. Similarly, the definition of steroid resistance for inclusion in the clinical studies varied from a minimum of 2 to 12 weeks of treatment. The most frequent outcome examined was reduction in proteinuria (complete or partial remission). Table 1 summarizes the various definitions used for complete and partial remission. Complete remission was defined in a fairly similar way across studies, whereas there was significant variability in the definitions of partial remission. Our quality assessment focused on internal validity (using the Cochrane Collaboration’s tool for assessing risk of bias and the Newcastle-Ottawa quality assessment scale), external validity, and precision and is summarized in Tables 2 to 5.
Characteristics of Reviewed Studies.

Note. ASA= amino-salicylic acid; FSGS = focal segmental glomerulosclerosis; MCD = minimal change disease; CrCl = creatinine clearance; RAAS = renin-angiotensin-aldosterone system; RCT = randomized controlled trial; Up/c = urinary protein-to-creatinine ratio; BP = blood pressure; ESKD = end-stage kidney disease; MMF = mycophenolate mofetil; IV = intravenous; eGFR = estimated glomerular filtration rate; ASA, amino-salicylic acid.
Visual Assessment of Internal Validity of Randomized Controlled Trials.

 Low risk of bias
Low risk of bias
 High risk of bias
High risk of bias
 Unclear
Unclear
Quality Assessment of Randomized Controlled Trials (Internal Validity).

Note. CSA = cyclosporine A.
Quality Assessment of Randomized Controlled Trials (External Validity).
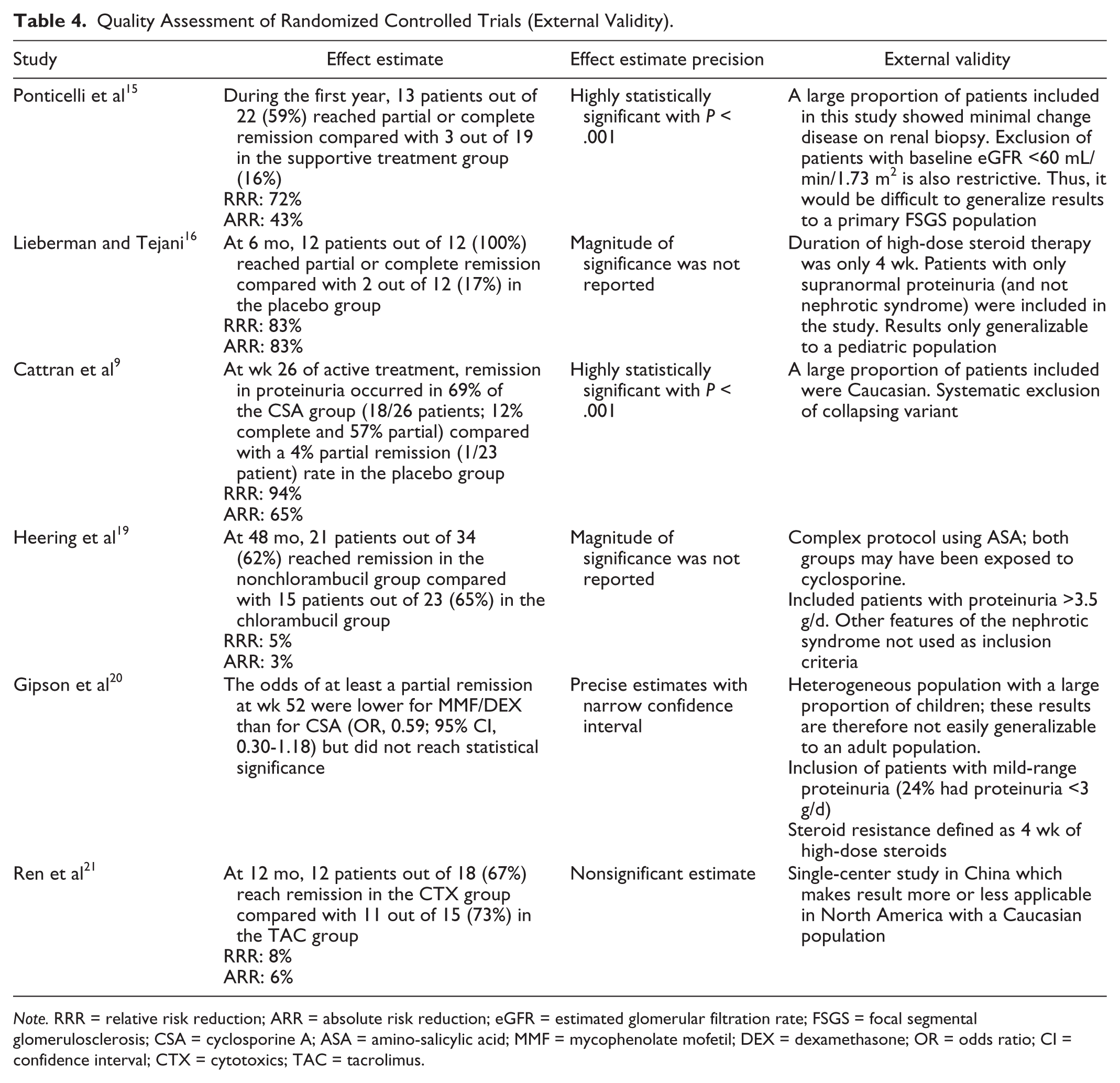
Note. RRR = relative risk reduction; ARR = absolute risk reduction; eGFR = estimated glomerular filtration rate; FSGS = focal segmental glomerulosclerosis; CSA = cyclosporine A; ASA = amino-salicylic acid; MMF = mycophenolate mofetil; DEX = dexamethasone; OR = odds ratio; CI = confidence interval; CTX = cytotoxics; TAC = tacrolimus.
Quality Assessment of Cohort Studies.

Note. FSGS = focal segmental glomerulosclerosis; IV = intravenous.
Findings
First-line therapy
The use of CNIs as first-line therapy has not been studied prospectively. Remission in proteinuria and renal failure (50% increase in serum creatinine) were evaluated in a retrospective study only. 10 Mortality and time to ESKD have not been examined in this literature.
A retrospective cohort study by Goumenos et al 10 compared renal outcomes associated with immunosuppressive therapy (prednisone alone, prednisone and azathioprine, or prednisone and cyclosporine) with those associated with supportive care. A higher proportion of patients treated with immunosuppressives than supportive care achieved complete or partial remission in proteinuria within the first year of follow-up. The mean duration of therapy was 20 ± 6 months. Treated patients also showed better renal survival using the end point of 50% increase in serum creatinine over 5 years of follow-up. However, this study did not adjust for factors influencing decision to treat or choice of treatment such as baseline proteinuria. The multivariate analysis only included presence of glomerulosclerosis at initial kidney biopsy and baseline serum creatinine. Moreover, patients treated with immunosuppression presented with a significantly lower serum albumin than those treated with supportive care (28 vs 34 g/L), which could bias toward an underestimation of treatment effect. This study was characterized by a heterogeneous treatment group, with a small number of patients treated with each immunosuppressive regime. Only 7 patients were treated with prednisolone and cyclosporine. Therefore, treatment with prednisolone alone could not be compared with treatment with cyclosporine and prednisolone due to a lack of statistical power.
Second-line therapy
Prospective trials in primary FSGS were designed to test the efficacy of steroid-sparing agents in a steroid-resistant FSGS population. Considering the long disease duration to reach clinically meaningful outcomes, remission in proteinuria was used as the main outcome in all reviewed studies. Mortality, renal survival, and renal function were rarely analyzed, and mostly as secondary outcomes when described.
Calcineurin inhibitors versus control
Three randomized controlled trials compared cyclosporine with placebo (with or without low-dose prednisone) or supportive treatment in a steroid-resistant population.9,15,16 The duration of glucocorticoid therapy used to define steroid resistance was different between studies, ranging from 4 to 8 weeks. All 3 studies showed a higher proportion of patients treated with CNIs achieving partial or complete remission than the comparison group. However, these studies were of relatively short duration (26-200 weeks); as such, change in serum creatinine was analyzed as a secondary outcome.
Ponticelli et al 15 conducted an open randomized trial comparing cyclosporine without glucocorticoids with supportive treatment. The study was not limited to patients with biopsy-proven FSGS. There were 14 patients with biopsy-proven FSGS in each arm, and an additional 8 patients in the cyclosporine group and 5 in the supportive treatment group with minimal change disease on biopsy. A “rescue treatment” with glucocorticoids was allowed in the supportive treatment group if patients experienced “rapidly progressive renal failure or very severe nephrotic syndrome” (although neither was clearly defined). During the first year of active treatment, the cyclosporine group had a significantly higher proportion of patients in remission (36% complete; 27% partial) compared with the control group (16% partial). Among patients with biopsy-proven FSGS, 8 in the cyclosporine group achieved remission within the first year (3 complete; 5 partial); the proportion in the supportive care group who achieved remission was not reported. The randomized treatment allocation helped minimize the risk of bias. However, the sample was small, and the groups were not balanced on some important potential confounders. For example, a greater proportion of patients in the cyclosporine group (36%) than in the supportive care group (26%) had minimal change disease on biopsy, conceivably biasing toward greater response in the cyclosporine group. In addition, 46% in the cyclosporine group were children compared with 37% in the supportive care group. The lack of blinding also opened the possibility of biased outcome ascertainment. Furthermore, the generalizability of study results to an exclusively adult or pediatric primary FSGS population is questionable given the heterogeneity of the study population. Another significant limitation is the exclusion of patients with eGFR <80 mL/min/1.73 m2 (children) or <60 mL/min/1.73 m2 (adults) at baseline.
In a randomized trial including patients aged 6 months to 21 years old, Lieberman and Tejani 16 compared cyclosporine without glucocorticoids (n = 16) with placebo (n = 15). Patients were treated with study drug, without concomitant prednisone. Among those who completed 6 months of active treatment, all patients in the cyclosporine group achieved remission (33% complete; 67% partial) compared with only 17% in the placebo group (100% partial) by 6 months. However, the definitions of partial and complete remission were unclear. Complete remission was defined as a decline in proteinuria to the normal range, with no mention of a requirement for stability in renal function. Partial remission was defined as a “reduction in proteinuria,” where the level of proteinuria still remained in the “supranormal” range, with no mention of the magnitude of the reduction or a threshold goal in proteinuria. In addition, sequence generation and allocation concealment were not clearly explained, but randomized groups were well balanced. Generalizability was limited by the inclusion of patients with “supranormal” proteinuria, rather than those meeting the criteria for nephrotic syndrome.
The randomized controlled trial by Cattran et al 9 is considered a landmark study. Both groups were treated with low-dose prednisone. At 26 weeks of active treatment, the proportion of subjects reaching complete or partial remission was significantly higher in the cyclosporine arm (12% complete; 57% partial) than in the placebo arm (4% partial). By week 78 (48 weeks after discontinuation of therapy), relapse in proteinuria occurred in 60% of those who attained a remission. By week 104 (74 weeks after discontinuation of therapy), 8% of patients were in partial remission in the placebo group compared with 32% in remission in the cyclosporine group (4% complete; 28% partial). Strengths of this study include a design minimizing bias and confounding, and a larger number of patients than in previous studies (n = 49). Although randomization procedures were appropriate, the placebo group had a higher proportion of males (74% vs 65%) and African Americans (14% vs 4%) and heavier proteinuria at presentation (8.7 vs 6.9 g/d) than the cyclosporine group. The generalizability of this study is somewhat limited by the relatively small proportion of African Americans and the explicit exclusion of patients with collapsing variant.
All 3 randomized controlled trials comparing cyclosporine with placebo or supportive treatment (with or without glucocorticoids) pointed toward a better chance of partial or complete remission with CNIs after 6 to 12 months of active therapy. As illustrated in Figure 2, the pooled relative “risk” of proteinuria remission associated with cyclosporine was 7.0 (95% confidence interval, 2.9-16.8) compared with placebo/supportive therapy. There was very low heterogeneity among these studies with an I-squared of 0%.

Meta-analysis of remission with calcineurin inhibitors in steroid-resistant focal segmental glomerulosclerosis.
Calcineurin inhibitors versus mycophenolate mofetil
Only 1 randomized controlled trial compared the efficacy of MMF and dexamethasone pulses (n = 66) with cyclosporine (n = 72) in steroid-resistant primary FSGS. 20 Both groups received low-dose prednisone for 6 months. The primary outcome was remission of proteinuria, which was classified into one of 6 categories. At week 52, on active treatment, the odds of at least partial remission were lower for the MMF/dexamethasone group, but the difference did not reach statistical significance. Among those who achieved at least partial remission at week 52, 33% in the cyclosporine group relapsed at week 78 (26 weeks after discontinuation of therapy) compared with 18% in the MMF/dexamethasone group. Better preservation of eGFR was seen in the MMF/dexamethasone arm. This randomized controlled trial was generally well designed. However, the treatment group was not blinded, opening the possibility of bias in outcome ascertainment. The study groups were well balanced at baseline. Generalizability was limited by the inclusion of patients with mild proteinuria (24% had proteinuria <3 g/d [urinary protein-to-creatinine ratio <2 g/g]), and the fact that patients with no remission after only 4 weeks of treatment with high-dose glucocorticoids were qualified as glucocorticoid-resistant.
Calcineurin inhibitors versus alkylating agents
Two randomized controlled trials compared use of an alkylating agent with CNIs in steroid-resistant idiopathic FSGS. In both studies, there was no difference between treatment groups in the proportion of patients who achieved remission in proteinuria.
The first study was characterized by a complex treatment regimen, including several different immunosuppressives in each study arm. 19 The cyclosporine group (n = 34) was initially treated with salicylic acid and prednisolone and, if no remission occurred, switched to cyclosporine alone. The chlorambucil group (n = 23) was initially treated with prednisolone alone, and if no remission occurred, chlorambucil was added. Then, if no remission occurred, patients were finally treated with cyclosporine alone (n = 10). The proportion of patients achieving remission within 48 months of follow-up was similar in the 2 study arms (62% in the cyclosporine group vs 65% in the chlorambucil group). Specifically, for the cyclosporine-treated, complete remission occurred in 23% and partial remission occurred in 38% of patients, with a mean duration of administration of 23 ± 16.5 months. Among the chlorambucil-treated over 6 to 12 weeks, complete remission occurred in 17% and partial remission occurred in 48% of patients within 48 months of follow-up. Renal survival was 83% for both groups after 4 years of follow-up. Although the study arms were well balanced at baseline, this study had several important limitations. First, random sequence generation was inadequate, allocation concealment was undefined, and there was no blinding. Furthermore, the complexity of the treatment regimen, and the fact that patients from both groups may have received cyclosporine, make the superiority of one drug over the other difficult to ascertain. Also, the definition of remission did not include a magnitude of reduction in proteinuria over time (eg, 50% as described in the 2012 KDIGO guideline).
A small study from China compared proteinuria remission among patients with steroid resistance or steroid dependence randomized to IV cyclophosphamide (n = 18) or tacrolimus (n = 15). 21 Both groups were treated with glucocorticoids, and patients with no response after 6 months were randomized. After 12 months of therapy, there was no significant difference in remission between the 2 groups: 66.7% in the cyclophosphamide group (50% complete; 16.7% partial) and 73.3% in the tacrolimus group (40% complete; 33.3% partial). The 12-month relapse rate was similar between the 2 groups (27.8% for cyclophosphamide-treated vs 26.7% for tacrolimus-treated). Patients treated with cyclophosphamide had poorer renal function at baseline. One patient was withdrawn from the study due to ESKD (cyclophosphamide-treated). The study had several limitations. Sequence generation and allocation concealment were not clearly defined. This study was small and was conducted in a single center in China, which hamper its generalizability to other countries.
Additional cohort study including calcineurin inhibitors
A study by Ehrich et al 22 was conducted to examine the potential benefit of adding IV methylprednisolone to cyclosporine and prednisolone in the treatment of steroid-resistant FSGS in 52 children. Compared with those untreated with IV methylprednisolone, significantly more patients treated with IV methylprednisolone (84% vs 64%) had cumulative sustained remission (complete or partial). This study had some weaknesses. The untreated cohort was selected from a different patient population (different time period) than the IV methylprednisolone group, and there was no control for important confounding factors (eg, baseline proteinuria or estimated glomerular filtration) in the analysis. The generalizability of this study to adults is also limited because the study population was primarily pediatric.
Discussion
The bulk of existing evidence suggests that CNIs in combination with glucocorticoids may increase the likelihood of complete or partial remission of proteinuria among individuals with steroid-resistant idiopathic FSGS. In this population, only cyclosporine has been evaluated in prospective trials with comparison against supportive therapy or placebo (with or without low-dose glucocorticoids). Cyclosporine appears effective in inducing remission but is associated with high relapse rates following discontinuation. Two studies comparing CNIs with supportive therapy/placebo had adequate internal validity with a well-executed randomized design and established CNIs as effective in achieving remission in proteinuria.7,9 Subsequent prospective studies compared CNIs with other active agents in a steroid-resistant primary FSGS population. The evidence supporting alkylating agents in steroid-resistant FSGS is not convincing, and CNIs appear to be more effective than MMF.
The efficacy of CNIs as a first-line agent remains undefined given the available evidence. The current evidence pertaining to steroid-resistant primary FSGS cannot be applied to a steroid-naive population because they represent distinct patient populations or disease entities. Only 1 retrospective study addressed the efficacy of CNIs as a first-line treatment for FSGS. 10 This study was small, and there was no direct comparison with other immunosuppressive agents. We recently reported an association between immunosuppressive therapy (glucocorticoids and/or CNIs) and better renal survival in a retrospective cohort of patients with primary FSGS. 23 However, this study was not able to delineate the difference in efficacy between early use of glucocorticoids and early use of CNIs, and was not designed to clearly assess the efficacy of CNIs in a steroid-naive primary FSGS population. In contrast, MMF has been evaluated as a steroid-sparing agent in first-line therapy of primary FSGS. A small prospective study (n = 33) compared MMF (1 g twice daily for 6 months) combined with low-dose glucocorticoids with high-dose glucocorticoids alone for 3 to 6 months. 24 Outcomes were similar for both groups, with 70% of patients in remission in the MMF group compared with 69% in the high-dose glucocorticoid group. Current KDIGO recommendations suggest, however, CNI use as first-line therapy in patients with relative contraindications or intolerance to high-dose glucocorticoids (eg. uncontrolled diabetes, psychiatric conditions, severe osteoporosis). CNI use would require the absence of significant renal dysfunction at initiation. In the current KDIGO guideline, CNIs were preferred given the evidence derived from prospective studies in the steroid-resistant primary FSGS population.
The clinical trials summarized in this review were of relatively short duration and included fairly small numbers of patients. As a result, they were not able to assess the impact of immunosuppressive therapy on renal or patient survival. Hard end points such as ESKD and mortality are infrequent and require many years of follow-up. Furthermore, the relatively small number of included studies and their heterogeneity with respect to treatment protocols, and possible publication bias, limit conclusions drawn from this systematic review.
This systematic review is distinguished from the KDIGO guideline 4 by its inclusion of more recent studies, and a systematic critical appraisal of the internal validity of each study using recognized tools (Cochrane Collaboration’s tool for assessing risk of bias and Newcastle-Ottawa quality assessment scale), but supports the same recommendation of CNI use in steroid-resistant primary FSGS patients. This study also includes a meta-analysis of the evidence comparing cyclosporine with supportive therapy and placebo (with and without glucocorticoids) in steroid-resistant primary FSGS. This provides a more precise weighted effect estimate of the association between cyclosporine therapy and remission in proteinuria than individual studies. However, it was not possible to perform other analyses for subgroups of interest (eg, children) due to paucity of data and heterogeneity in treatment regimens. This review is also distinguished from the Cochrane review 12 by the inclusion of 4 more randomized controlled trials (2 after 2008) and by the pooled analysis of the trials comparing cyclosporine with placebo. Moreover, this study highlights the current knowledge gaps in the treatment of primary FSGS: the absence of high-quality evidence on commonly used first-line therapies (glucocorticoids and CNIs) and the use of intermediate outcomes for renal survival in studies on the role of CNIs in steroid-resistant primary FSGS patients.
In conclusion, further research is needed to assess effectiveness of CNIs as first-line therapy in primary FSGS. A large randomized trial would be challenging with potential issues in recruitment and retention because glucocorticoids have been used as a first-line treatment for decades and primary FSGS can be considered as a rare disease. Such trial would also require a long follow-up time to reach significant renal outcomes. Good quality observational studies would be particularly suitable to measure the effect of CNIs on renal survival in steroid-naive FSGS population.
Footnotes
Acknowledgements
L.-P.L. received salary support from Hôpital Maisonneuve-Rosemont Scholarship of Improvement Program, Société Québécoise de Néphrologie, and Department of Medicine, Université de Montréal.
List of Abbreviations
ARR = absolute risk reduction; ASA = amino-salicylic acid; BP = blood pressure; CNIs = calcineurin inhibitors; CrCl = creatinine clearance; CSA = cyclosporine A; CTX = cytotoxics; DEX = dexamethasone; eGFR = estimated glomerular filtration rate; ESKD = end-stage kidney disease; FSGS = focal segmental glomerulosclerosis; IV = intravenous; KDIGO = Kidney Disease: Improving Global Outcomes; MCD = minimal change disease; MMF = mycophenolate mofetil; PICO = Population Intervention/exposure Comparison Outcome; RAAS = renin-angiotensin-aldosterone system; RCT = randomized controlled trial; RRR = relative risk reduction; TAC = tacrolimus; Up/c = urinary protein-to-creatinine ratio.
Ethics Approval and Consent to Participate
This was not applicable.
Consent for Publication
This was not applicable.
Availability of Data and Supporting Materials
This was not applicable.
Author Contributions
L.-P.L. and B.J.F. contributed to the conception and design of the study, analysis and interpretation of data, and drafting the article; P.H.N. contributed to the analysis and interpretation of the data and revising the manuscript for important intellectual content.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.