
Abstract
Summary
Systemic lupus erythematosus (SLE) usually affects young females and its presentation with haemorrhage is unusual. Intracerebral bleed (ICB) has been described in a few case reports, but massive haematuria has not been reported in the literature so far. Here, we present a case of a 56 year-old-lady who presented with expanding lobar bleed and massive haematuria as the first presentation of SLE secondary to vasculitis. Lupus vasculitis usually presents with thrombosis-related complications and although bleeding in this context is rare, it can lead to catastrophic consequences. Hence, vasculitis-related bleeding should be taken under consideration in a challenging situation like ours.
Case report
A 56-year-old female presented to emergency department with a sudden loss of consciousness for 1 hour. There was no history of fever, fits, fall, vertigo before it. She was vitally stable, glasgow coma scale 10/15 with left hemiparesis. Her Computed tomography Head scan head showed right lobar bleed in frontoparietal area with surrounding oedema but no midline shift. Computed tomography angiogram was normal. Her admission labs showed haemoglobin of 9.8 g/dL (normocytic normochromic) while total leukocyte count and platelets were within normal range. ESR was 64 and coagulation profile was normal. Renal and liver profiles were normal. Urine routine examination showed +2 protein and red cell casts. Her past history was significant for an episode of haematuria 1 year back that was self-limiting. Workup that was done at that time revealed bicytopenia (hemoglobin: 9.1, mean corpuscular volume: 84, total leukocyte count: 3.1) and ultrasonogram abdomen and pelvis showed minimal ascites. She also had a history of lymphocytic exudative pleural effusion 1.5 years back that settled within a month. However, no history of fever, photosensitivity, rash or joint pain was there.
On the second day of admission, she developed gross haematuria. Computed tomography scan pelvis didn't reveal structural abnormality in the urinary tract. On cystoscopy, there were multiple clots in the urinary bladder, however, no source of bleed was identified. Patient's urinary bladder was kept clot free by continuous three-way irrigation. To elaborate on the cause of spontaneous bleed from two major organs without any structural lesion, her blood peripheral smear was reviewed by haematologist and reported normal cells morphology with adequate platelets exhibiting clumping. Prothrombin time, activated partial thrombin time, bleeding time, clotting time, fibrinogen degradation products, fibrinogen, factor XIII, Coombs test and lactate dehydrogenase were normal.
Keeping in view the history of polyserositis, cytopenia in the past and present history of bleeding from multiple sites without any haematological abnormality, presence of cast and protein in urine and high erythrocyte sedimentation rate, suspicion of systemic lupus erythematosus (SLE) was raised and relevant workup was advised. Patient's anti-double stranded DNA, antinuclear antibodies, anti-nucleosome antibodies came out to be strongly positive, whereas complement 3 and complement 4 levels were significantly below the normal range. Her anti-smith, anti-myeloperoxidase antibodies, anti-proteinase-3, anti-glomerular basement membrane antibody, antiphospholipid antibodies profile were negative. Clinical and lab evidence supported the diagnosis of systemic lupus erythematosus, thus she was started on intravenous steroid pulse therapy.
On the third day of admission, her glasgow coma scale was dropped, and repeat computed tomography head showed haematoma expansion with significant mass effect and midline shift. She underwent craniotomy for haematoma evacuation. Serial computed tomography head scan head of patient can be seen in the figures below (Figure 1).
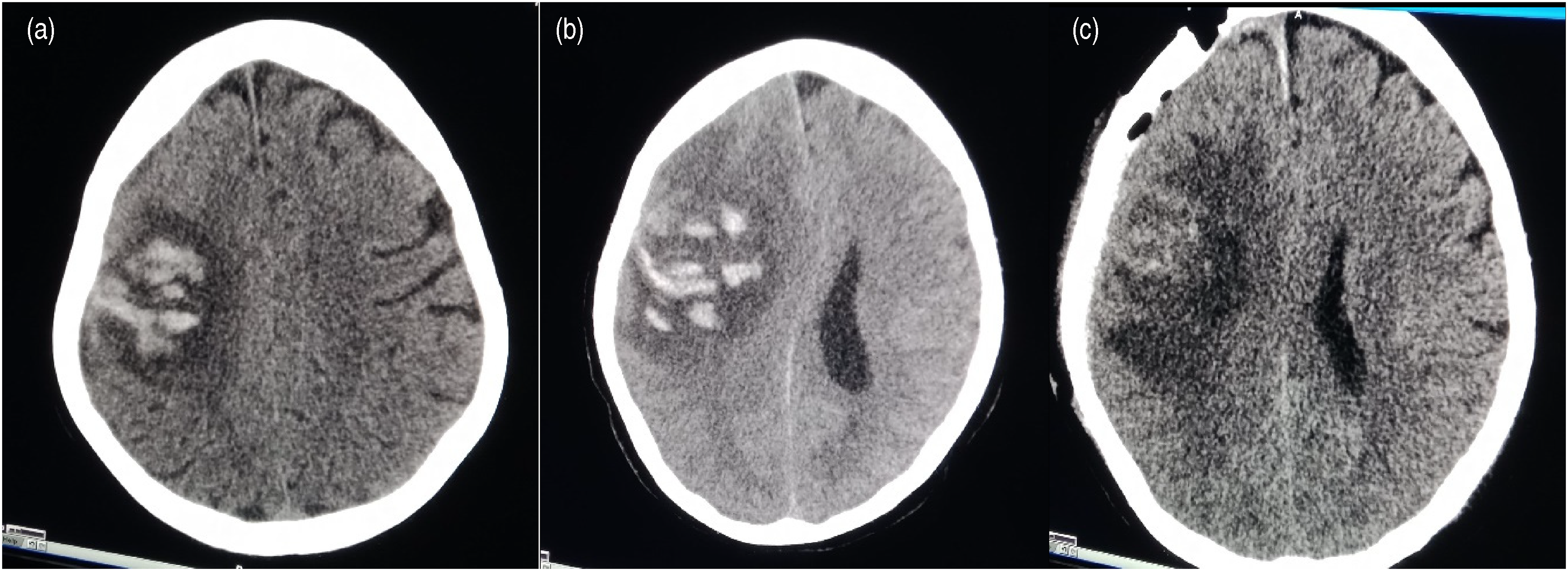
(a–c) Day 1, Day 3 and post-craniotomy CT scan head.
Blood vessel biopsy from the brain was taken preoperatively and sent for histopathology that showed acute necrotising vasculitis (Figure 2(a) and 2(b)).

(a) 10X magnification: Intima is irregular and partly eroded with thrombin deposition. Media shows haemorrhages. (b) 40X magnification: Media shows scattered mononuclear infiltrate along with a small collection of neutrophils. The adventitia shows acute on chronic cell infiltrate. Calcification can also be appreciated in this image.
On the fifth day of admission, she developed widespread palpable purpura on thighs and flanks and expanded to the lower abdomen and back with patchy skin necrosis. She also started bleeding from mucosal membranes (oral cavity and nose). Lab parameters including complete blood count including peripheral blood smear, reticulocyte count, Serum bilirubin, Coombs test (indirect and direct), prothrombin time / activated partial thromboplastin time were repeated again. Except for drop in Hb no abnormality was found. Multiple blood transfusions were already being done in view of ongoing haemorrhage. In this catastrophic stage, intravenous immunoglobulins were considered but the patient deteriorated rapidly and couldn't be saved. She died on the sixth day of admission.
Discussion
Haemorrhage from different sites has been reported in systemic lupus erythematosus in the form of case reports.1–5 Hypertension, hypercholesterolaemia, corticosteroids, thrombocytopenia and vasculitic process increase the risk of bleeding in any organ including Central Nervous System.1,2 Moreover, coagulation factors deficiency or the presence of antibodies against them can be a cause of profuse bleeding; prolonged activated partial thromboplastin time in the context of lupus anticoagulant systemic lupus erythematosus is also considered a risk for haemorrhage. 6
Intracerebral bleed (ICB) in the systemic lupus erythematosus secondary to vasculitis is rarely reported in the literature.7–8 Massive haematuria in systemic lupus erythematosus hasn't been documented in literature before in this regard. Moreover mucosal and subcutaneous bleeding are also rare to find in the literature.
Multiple cases of bleeding from different sites have been reported in the forms of case reports in literature but there are some peculiar features that distinguish our case.
First, it was, unusually, a delayed presentation: our patient developed symptoms at the age of 56 years, and she remained undiagnosed for around 2 years prior to admission to us.
Second, bleeding per se is an unusual feature of systemic lupus erythematosus, and vasculitis-related haemorrhage is more rare. systemic lupus erythematosus usually presents with vasculitis-related infarct. Few cases of intracerebral bleed have been reported in previously diagnosed patients of systemic lupus erythematosus who had haematological disturbances related to systemic lupus erythematosus. In our case, intra-cerebral bleed was the first presentation that led to systemic lupus erythematosus diagnosis and the cause of bleeding was necrotising vasculitis supported by histopathology. In one case of systemic lupus erythematosus-related central nervous system haemorrhage, non-specific inflammation of intracranial arteries was reported. Arinuma et al. described necrotising vasculitis in antiphospholipid antibodies profile-related systemic lupus erythematosus. 7 In our case antiphospholipid antibodies profile was negative.
Third, our case report takes the credit of being amongst the few cases that have described biopsy features of systemic lupus erythematosus vasculitis presented with haemorrhage.
Fourth, to our knowledge, gross haematuria in systemic lupus erythematosus causing haemodynamic compromise has not been described in literature before in the absence of renal or haematological abnormality. It makes our case the first ever reported case of systemic lupus erythematosus-related vasculitis causing massive haematuria. Moreover, subsequent bleed from the mucosal surface and subcutaneous tissue along with skin necrosis is the unique feature of our case.
Finally, rapid fulminant course of disease along with no response to steroid pulse therapy, although not unusual in systemic lupus erythematosus, led to serial catastrophic consequences. In this situation, plasma exchange or intravenous immunoglobulins could have been the game changer but by the time histopathology report was confirmed, vasculitis patients have gone into an irreversible state of damage.
Treatment stay of systemic lupus erythematosus vasculitis is pulse steroid followed by cytotoxic drugs, plasma exchange or intravenous immunoglobulins. Overall, prognosis depends upon patient’s response and disease severity. Modifying cytokine response, manipulation of toll-like receptors, chemokines and specific B cell therapies can serve as potential emerging treatment. 9
Conclusion
Bleeding in systemic lupus erythematosus is rare but can lead to catastrophic consequences. Early recognition of underlying pathophysiology is important to halt the ongoing insult.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.