
Abstract
A pair of middle-aged sisters is presented who experienced episodes of spontaneous, relatively atraumatic, acute onset, painful sub-cutaneous bleeding into the digits of their hands over a number of preceding years. A literature search revealed they had Achenbach’s syndrome, which is a benign and self-limiting condition that resolves completely within 2–4 days. However, a hitherto unreported association between Achenbach’s syndrome and joint hypermobility with its abnormal collagen is made, along with a tentative causality hypothesis that perhaps in the presence of atypical connective tissue, the architecture and integrity of the peripheral capillary bed of the hand could be adversely affected and therefore predispose towards paroxysmal palm and/or finger bleeds.
Introduction
The condition of either a palm or a proximal/middle finger phalange experiencing a sudden sharp pain, followed by volar, sub-cutaneous bleeding and blue-black discolouration with swelling and numbness that develops over a few minutes, was first described by Achenbach in 1957. 1
Other cases have since been published,2–9 involving restricted finger bending, 8 digital swelling in 60% of cases and paraesthesia and or itching in 25% of cases. 3
As the haematoma enlarges, it spreads into the adjacent phalanges and the palm of the hand with ensuing pain relief, 2 but characteristically never into the fingernail or fingertip.2,7
The haematomas take a median of four days to disappear 3 and occur without the prolonged colour changes that are associated with an ecchymosis. 5
The syndrome is characterised by recurrent episodes and while a third of cases arise from simple, every-day manual activities, most develop spontaneously and without any abnormal coagulation variables.3,6
In Britain, the female to male predilection is 6:17 with a median presentation age of 50 years, 3 but at present, there seem to be neither prevalence nor incidence data published for this condition, nor any aetiological explanations.
First case presentation
A non-smoking, 64-year-old female dental hygienist presented with a bruised and swollen right index finger, which arose spontaneously as a sudden pain on the volar-lateral aspect of the right index finger’s proximal phalange. Within an hour, the bruising and swelling extended distally into the second phalange, but not into the fingertip (Figure 1(a)). It then progressed proximally into the palm of the hand (Figure 1(b)) with ensuing pain alleviation. Over the following three days, the discolouration, discomfort and swelling subsided and the finger’s mobility normalised.
(a) Subcutaneous bruising and oedema of the hygienist’s right index finger, with sparing of the fingertip. (b) Bruising extending into the palm of the hygienist’s hand.
She gave a history of approximately a dozen similar episodes over the preceding few years, but never with thumb or little finger involvement.
On each occasion, her manual dexterity and clinical practice were diminished for several days.
The Brighton Major and Minor Criteria used to determine the joint hypermobility scores for the two siblings.

Of her minor Brighton criteria, she had suffered with intermittent joint pain in her right hip for three months (radiographic absence of trauma, neoplasia or degenerative osteoarthritis) and she had had blepharoplasties to correct droopy eyelids, which had obstructed her vision.
A full blood count, clotting screening and a tourniquet capillary resistance test of Hess were all normal.
Second case presentation
The hygienist’s 59 year-old non-smoking retired bank manager sister confirmed that her paroxysmal haematomas began in her mid-fifties, with the involvement of the fingers of both hands, but predominantly those in her dominant right hand. She reported only one episode in the palm of her hand (Figure 2(a)), but never any in either her thumb or little finger. She displayed similar signs and symptoms to her sister, and reported that (i) the bleeds are always associated with activities such as carrying shopping or opening a stiff glass jar, (ii) the pain feels like a needle is being stuck into the finger and it looks like a blood vessel has burst, (iii) with volar bruising that spreads 3–4 mm beyond, but never with any swelling, and (iv) they always completely resolve within 24 h (Figure 2(b)). She responded affirmatively to one major and one minor Brighton criteria, but with a positive response to all of the Beighton scores, indicating a similar, probable involvement with joint hypermobility syndrome (Table 1).
(a) Spontaneous haematoma in the palm of the sibling’s hand. (b) Complete resolution of the palm haematoma 24 h later.
Her medical history only involved two isolated grand mal episodes in the preceding six years, for which no cause could be found.
Discussion
The similar and differentiating features between Achenbach’s syndrome and two other major vascular disorders with digital presentations.
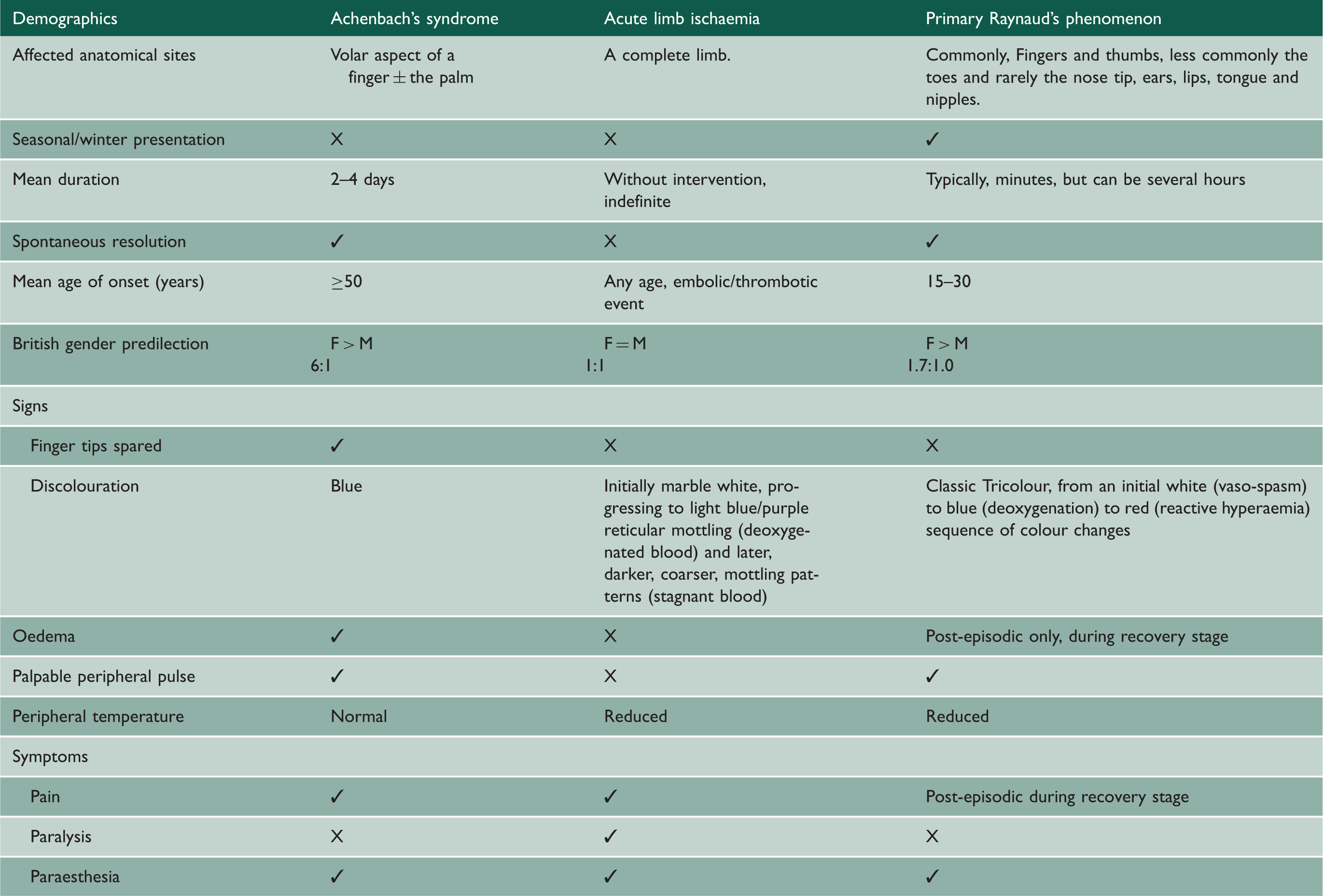
The application of either a circulatory disease algorithm, 3 or a sieve, 7 duplex sonography and or peripheral angiography may be used to exclude ischaemic conditions. 2
However, given the characteristic presentations, the two- to four-day spontaneous regressions and the fact that Achenbach’s syndrome has no association with serious bleeds into other organs,2,3 the need for any invasive diagnostics is usually precluded,2,5–7 just simply the delivery of some simple reassurance.2,3
Similar comorbidities that were present in the hygienist have been previously reported in other Achenbach patients, but no pathogenic connections have ever been established. 2
For both cases, an association with joint hypermobility syndrome was apparent and a causal relationship is therefore tentatively hypothesised; namely, that the abnormal collagen could perhaps adversely affect the architecture and integrity of the peripheral capillary bed of the hand, thereby resulting in spontaneous paroxysmal palm or finger bleeds, in a similar conceptual way to how the abnormal extracellular matrix fibrillin in Marfan’s syndrome predisposes these patients towards dissecting aortic aneurysms.
However, with just two cases demonstrating an association between Achenbach’s syndrome and joint hypermobility, the credibility of a possible causal link can only be improved by the identification of more cases.
Conclusion
While Achenbach’s syndrome is uncommon, the reported association with joint hypermobility syndrome that this case series illustrates should alert clinicians to become more vigilant in looking for comorbidity prevalence in other similar patients. As a consequence, in addition to haematological investigations, capillary fragility and coagulation blood tests for Achenbach syndrome patients, they should also be screened for joint hypermobility using the Brighton criteria questionnaire,10–12 with referral to a rheumatologist or a specialist in connective tissue disorders, as appropriate. If joint hypermobility is found to co-exist more widely, this could stimulate further research into the role that abnormal collagen may have in compromising the architecture and integrity of the peripheral capillary bed of the hand.
Supplemental Material
sj-pdf-1-shr-10.1177_20542704211023162 - Supplemental material for Achenbach’s hand and digital paroxysmal haematomas: a possible association with joint hypermobility syndrome in two sibling cases
Supplemental material, sj-pdf-1-shr-10.1177_20542704211023162 for Achenbach’s hand and digital paroxysmal haematomas: a possible association with joint hypermobility syndrome in two sibling cases by Robert Anthony Clive Chate in JRSM Open
Supplemental Material
sj-pdf-2-shr-10.1177_20542704211023162 - Supplemental material for Achenbach’s hand and digital paroxysmal haematomas: a possible association with joint hypermobility syndrome in two sibling cases
Supplemental material, sj-pdf-2-shr-10.1177_20542704211023162 for Achenbach’s hand and digital paroxysmal haematomas: a possible association with joint hypermobility syndrome in two sibling cases by Robert Anthony Clive Chate in JRSM Open
Supplemental Material
sj-pdf-3-shr-10.1177_20542704211023162 - Supplemental material for Achenbach’s hand and digital paroxysmal haematomas: a possible association with joint hypermobility syndrome in two sibling cases
Supplemental material, sj-pdf-3-shr-10.1177_20542704211023162 for Achenbach’s hand and digital paroxysmal haematomas: a possible association with joint hypermobility syndrome in two sibling cases by Robert Anthony Clive Chate in JRSM Open
Footnotes
Declarations
Competing Interests
None declared.
Funding
None declared.
Ethics approval
Not applicable.
Guarantor
Robert Anthony Clive Chate
Contributorship
Sole author.
Acknowledgements
I used the CARE checklist 13 when writing this paper.
Provenance
Not commissioned; peer-reviewed by JRSM Open Referee.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.