
Abstract
Objective
To model cost and benefit of a national community health worker workforce.
Design
Modelling exercise based on all general practices in England.
Setting
United Kingdom National Health Service Primary Care.
Participants
Not applicable.
Data sources
Publicly available data on general practice demographics, population density, household size, salary scales and screening and immunisation uptake.
Main outcome measures
We estimated numbers of community health workers needed, anticipated workload and likely benefits to patients.
Results
Conservative modelling suggests that 110,585 community health workers would be needed to cover the general practice registered population in England, costing £2.22bn annually. Assuming community health workerss could engage with and successfully refer 20% of eligible unscreened or unimmunised individuals, an additional 753,592 cervical cancer screenings, 365,166 breast cancer screenings and 482,924 bowel cancer screenings could be expected within respective review periods. A total of 16,398 additional children annually could receive their MMR1 at 12 months and 24,716 their MMR2 at five years of age. Community health workerss would also provide home-based health promotion and lifestyle support to patients with chronic disease.
Conclusion
A scaled community health worker workforce integrated into primary care may be a valuable policy alternative. Pilot studies are required to establish feasibility and impact in NHS primary care.
Keywords
Introduction
Increasing workload, a reduced percentage of the budget and workforce retention and recruitment problems challenge the capacity of available general practitioners in the UK NHS. 1 Consequently, patients’ ability to obtain general practitioner appointments has declined. 2 Political pressure to improve access 3 has been accompanied by promises of increased general practitioner numbers, 4 but with a reported fall in 2016–2017, 5 it remains unclear how this will be achieved. Meanwhile, financial constraints have also led to the loss of some community-based health services, such as district nursing 6 and fragmentation of others. 7
Community health workers
In the 1960s, programmes in the US funded members of the community to provide a bridge between patients and healthcare providers. 8 Facilitating appointment-keeping and increasing compliance with medications, community health workers improved access to and quality of healthcare, while reducing costs. Growing evidence now supports building primary care services with community health workers. 9 In the UK, NHS lay health trainers support patients with smoking cessation, breastfeeding, physical activity and weight loss. However, focus on single areas of health and lack of integration with primary care increases system complexity and leads to missed opportunities and duplication. 10
Some low- and middle-income countries, such as Ethiopia, Pakistan and Nigeria, have taken a much more systematic approach to community health workers in healthcare system design. 10 An example is Brazil’s Family Health Strategy, a publicly funded, free-at-point-of-use primary care system, founded in 1988 and now providing services to 70% of the country’s 200 million inhabitants. 11
Community health workers in Brazil have basic training in disease identification and monitoring, immunisation, and screening support and health promotion. Their skillset includes supporting patients with medication adherence and healthcare system navigation, monitoring chronic disease and identifying new symptoms. Each is responsible for around 150 households, in a defined catchment area, which they visit at least once per month. 12 Community health workers gain detailed knowledge of all members of these households and liaise proactively with general practitioners and practice nurses to avoid crises and complications. 12
Having previously explored the complex landscape of community care, 13 we argue that systematic deployment of community health workers in the NHS has the potential to address current problems of fragmentation and inefficiency, while improving clinical outcomes through improved uptake of appropriate services. 14 This study builds the case for a scaled community health worker workforce by estimating likely costs and key benefits of their deployment throughout NHS primary care in England, following the Brazilian Family Health Strategy model.
Methods
We used published NHS quality data and national demographic census data to model several scenarios, estimating the number of community health workers likely to be required to cover the population of England and their potential impact.
Estimating the number of community health workers required
A community health worker in Brazil typically serves 100–200 households, depending on whether in a rural or urban area. With the average household size of 3.3 persons in Brazil
15
and 2.4 persons in England,
16
we calculated the number of households a community health worker could expect to serve in England
We then estimated the number of households served by a given general practice, for each practice in England, using published general practice data from the Quality and Outcomes Framework
17
and Local Authority District,
18
with each general practice assigned to their corresponding Local Authority District

The number of community health workers that would be allocated to each general practice, accounting for regional variation in household size, was then estimated as follows
We considered a population density of one person per hectare to mark the threshold, where a community health worker would spend more time travelling than visiting. Using published population density data for Local Authority Districts and estimated travel times to key services, 19 we identified 359 general practices in Local Authority Districts with this population density or less, which we excluded from subsequent modelling. Figures for community health workers required for the remaining general practices were aggregated to give the number required across England.
We also estimated the number of visits community health workers would be able to make to each of their allocated households per year. There were 253 working days in 2018 in England, and newly appointed NHS staff are entitled to 27 days annual leave,
20
leaving 226 days available per community health workers. NHS District Nurses in the UK, whose visits are likely to be of greater complexity, routinely carry out eight visits within a 5-h daily visiting period.
21
If community health workers carry out a similar number, this would amount to 1808 visits per community health worker annually. Number of visits per household per year was calculated as follows
We estimated the annual cost of introducing community health workers in England using published salary figures,
22
with the Band 2 bracket chosen to reflect their responsibilities.
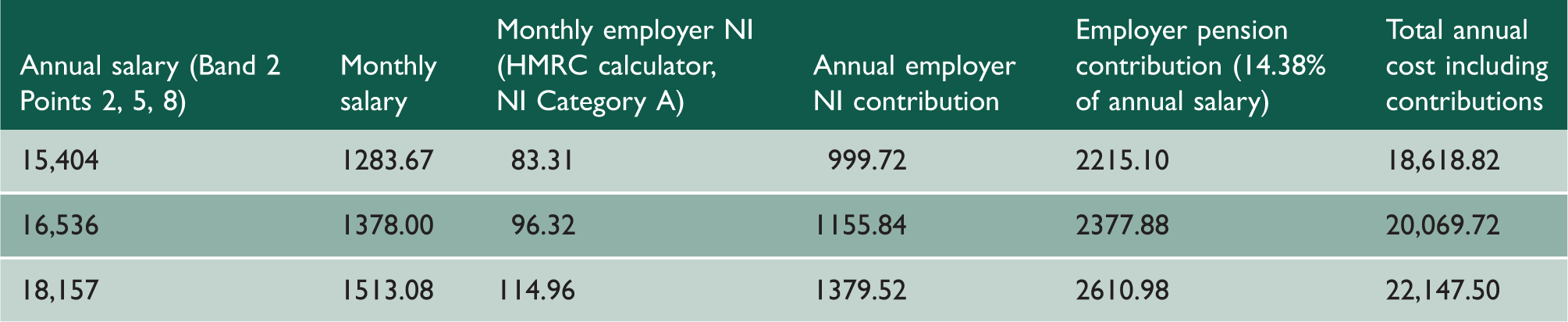
Salaries were calculated using three possible Band 2 salary points (Point 2, 5 and 8 – equivalent to salaries of £15,404, £16,536 or £18,157), corresponding to the level of Healthcare Assistant. We also considered other regular employment costs: employer National Insurance contributions were estimated using HMRC’s online calculator, 23 while employer pension contributions were calculated at the 14.38% rate required of NHS employers. 24 Initial training and administration costs were considered to be negligible in annual cost calculations.
Modelling the clinical impact of community health workers
Evidence suggests the impact of community health workers on a variety of aspects of primary care including chronic disease management and immunisation and cancer screening uptake.9,25,26 We have previously estimated that 88% of households in England and Wales have at least one person eligible for a service where community health worker intervention may provide benefit. 27 Consequently we modelled the potential impact of their integration in UK primary care in the following areas.
Chronic disease management
We selected five chronic diseases to model the patients community health workers would support. Asthma, chronic obstructive pulmonary disease, dementia, diabetes and hypertension were chosen based on their high prevalence and the likelihood of their management being improved through community health worker visits. Using published Quality and Outcomes Framework prevalence data for each general practice,
17
we estimated the number of patients with each condition that a community health worker would manage in each practice.
Cancer screening and immunisation uptake
We also modelled the impact of community health workers on cancer screening and childhood immunisation uptake rates. Estimates of the impact of community health workers in these areas vary,9,26 so we calculated rates assuming that community health workers could successfully refer either 10%, 20% or 30% of eligible individuals who had missed the opportunity to be screened or vaccinated.
Data for cancer screening were obtained from the National Health Application Infrastructure Services via the Open Exeter system. 28 Since routine cancer screenings have various time intervals, the screening programmes use differing review periods; we followed these to estimate the impact of community health workers on screening uptake rates for each cancer. Women aged 25–49 years are invited for cervical cancer screening every three years, while women aged 50–64 are invited every five years. A combined period (3.5 and 5.5 years) is used to determine screening coverage, which we followed to estimate the number of additional people screened through community health worker intervention. Women aged 50–71 years are invited for breast screening every three years; the screening programme uses a three-year screening coverage period. Bowel cancer screening is offered to all men and women aged 60–74 every two years; screening uptake is calculated over 2.5 years. Impact on MMR 1 and MMR 2 immunisation uptake was calculated in terms of additional children immunised annually based on NHS England data on immunisation rates. 29
Results
In Brazil, community health workers are responsible for between 100 and 200 households corresponding to 137.5–275 households in England. We additionally modelled a mid-point (206.25 households).
Assuming 226 working days per community health worker per year and visiting of eight households daily, 21 if community health workers each had responsibility for 137.5 households, they would visit each household 13.1 times per year. With a case load of 206.25 households, they would visit 8.8 times per year; if managing 275 households, they would visit 6.6 times per year.
NHS employment costs per community health worker.
Number and expected cost of CHWs required to serve NHS England and chronic disease patient load.
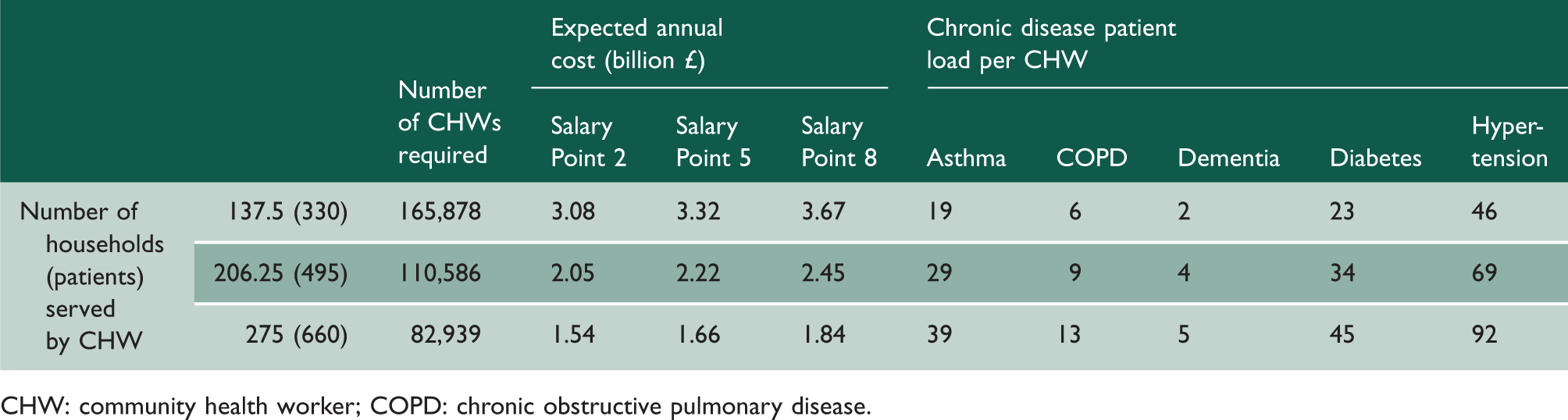
CHW: community health worker; COPD: chronic obstructive pulmonary disease.
Impact of CHWs on cancer screening and MMR immunisation uptake.
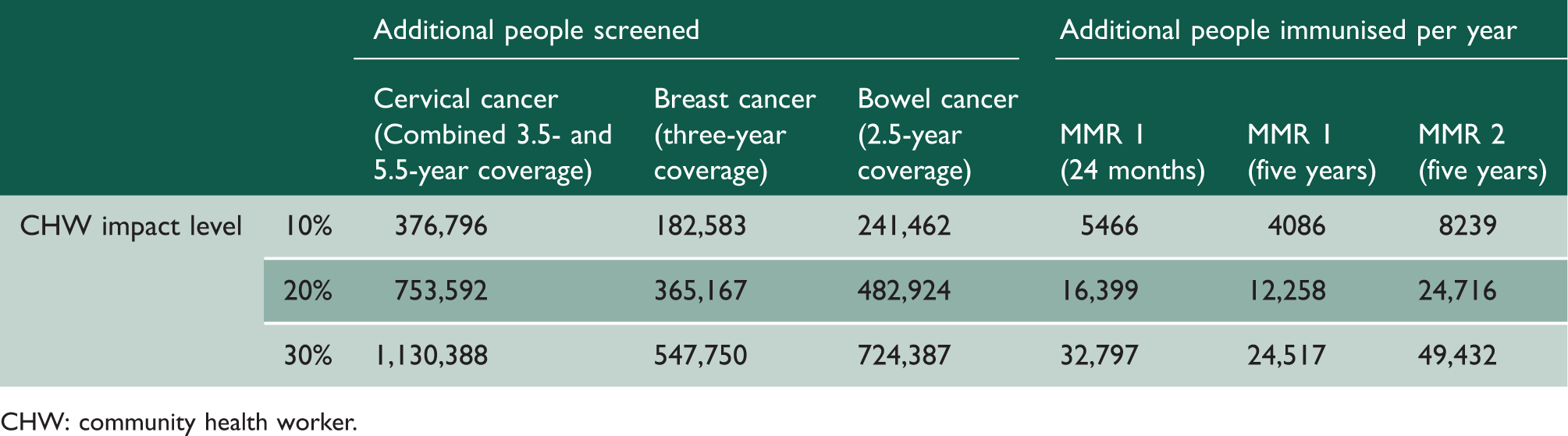
CHW: community health worker.
If community health workers led to successful screening of 20% of previously missed individuals, this would equate to an additional 753,592 new cervical cancer screenings nationally, with 365,166 new breast cancer screenings and 482,924 bowel cancer screenings, during the relevant time periods for each programme. Successful referral of 20% of children who had missed immunisations would mean that each year a further 16,398 children would receive MMR1 at 12 months and 24,716 children would receive MMR2 at five years of age.
Discussion
Summary
Our mid-range estimate of households per community health worker, with each household visited at least every six weeks, requires a workforce of 110,585, costing the NHS £2.22bn annually. If community health workers resulted in 20% of individuals who had missed immunisation or cancer screening taking up these opportunities, we could expect an additional 753,592 cervical cancer screenings, 365,166 breast cancer screenings and 482,924 bowel cancer screenings during their respective time periods. An additional 16,398 children per year would receive their MMR1 at 12 months and 24,716 children would receive their MMR2 at five years of age. All patients with chronic diseases would have regular health promotion, and individuals would be proactively identified for emerging physical health, mental health or social care issues.
Strengths and limitations
Brazil is an example of a country where community health workers have been integrated in a systematic manner in primary care. The Brazilian health system differs from that in the UK, and the impact of community health workers in the UK may be smaller overall, given differences in baseline health provision, health needs, health inequalities and health literacy. However, evidence does exist for community health workers in high-income countries. While this generally focuses on low-income and minority populations, 9 community health workers’ potential merits are significant in any population where there are missed opportunities to immunise, screen, actively case find and promote health. In the US, there is a growing belief that the community health worker model can inform community-based healthcare services. 30
As in any modelling exercise, this study is limited by assumptions such as average household size and the number of households that community health workers have responsibility for. We took measures to minimise the effect of these by using published data on general practice list size, population characteristics, population density, disease prevalence and screening and immunisation uptake, and by modelling a variety of different scenarios.
We excluded general practices in sparsely populated areas because we considered community health workers unlikely to be effective in these areas. In reality, alternative arrangements would have to be made for these areas either through additional support for general practitioner provision or with the introduction of more novel interventions, such as telemedicine services, to avoid inequalities.
Modelling impact of community health workers on cancer screening and immunisation uptake required assumptions as to possible effect size. Wide variation exists in reported effect size of community health worker interventions, ranging in immunisation uptake from no effect to 36% relative increase in immunisations. 9 We opted therefore to provide alternative models assuming community health workers facilitate uptake by 10%, 20% or 30% of eligible but unscreened or unimmunised individuals.
Mixed evidence for the impact of community health workers on chronic disease management meant that it was not possible to estimate impact in terms of clinical outcomes. Consequently, we selected five chronic diseases common in UK primary care, and used published prevalence data to illustrate the numbers of patients with these conditions that community health workers might provide with home-based support, thus indicating the possible benefit to general practices in additional chronic disease management.
Comparison with existing literature
Increasing evidence supports the effectiveness of the community health worker model, which has in Brazil been associated with a remarkable decline in infant mortality 31 and cardiovascular and cerebrovascular disease mortality, 32 reductions in hospitalisations 33 and improvements in equity of access.34,35 Although community health workers have not been shown to be singularly responsible, studies have shown a dose–response relationship between coverage with community health workers and benefits.32,33,35
Heterogeneity of interventions and outcomes in previous studies have made comparisons and translation into practice difficult. Systematic reviews of community health worker interventions9,25,26 have concluded that they have promise in improving some specific health outcomes, such as childhood immunisation and cancer screening uptake and chronic disease management, but that further research is required. Furthermore, the few studies providing economic information, and the heterogeneity of methods, mean that while there is evidence of cost effectiveness of community health workers in some settings, this is insufficient to draw broader conclusions.25,36 Nevertheless, the possibility of improvements in patient engagement in areas such as health promotion and disease prevention, 37 chronic disease management, 37 cancer screening 38 and immunisation, 9 suggest that community health workers in England could have important beneficial effects on health outcomes, particularly if deployed systematically. In addition, their ability to liaise closely with general practitioners, identifying problems early and supporting chronic disease monitoring indicates potential to reduce unnecessary workload burden on general practitioners, improving access while reducing use of acute and secondary care services. 37
To our knowledge, there has been no other attempt to date to model the feasibility of a nationally scaled community health worker workforce in primary care in England.
Implications for research and practice
The 2017 Report of the Select Committee on the Long-term Sustainability of the NHS and Adult Social Care 39 stated that the absence of any comprehensive national long-term strategy to secure an appropriately skilled and committed workforce represents the biggest internal threat to the long-term sustainability of the NHS. Several other recent high-profile reports have focused on community care and the need for streamlining of health and social care, joined up working, breaking barriers between services and reducing system complexity.7,40 Elements of care provided by community health workers in Brazil are being introduced in the NHS in the form of social prescribing, but evidence for these alone is lacking. 41 Numerous interventions and government initiatives over some 20 years have failed to result in actual system wide integrated care. 42 A scaled and integrated community health worker workforce, offering proactive, preventative and holistic community based care, may have the potential to succeed in achieving these aims where previous efforts have failed.
Large-scale implementation of NHS-funded community health workers in the UK represents a significant investment and recruitment challenge. However, this should be viewed in the context of other recent policy recommendations. For example, the Government remains committed to recruiting and funding 5000 additional NHS GPs. 4 This number of general practitioners would serve approximately 8.6 m patients assuming a practice list size of 1724 patients per general practitioner, 43 far fewer than the population served by the community health worker model. The annual salary cost would be £354.6 m and, as it costs £388,000 to train a general practitioner, including tuition, clinical supervision and salary during training, 44 the likely overall cost for 5000 general practitioners would be £1.94bn. We anticipate minimal training and support costs for community health workers, who in Brazil receive only a few weeks’ basic training. In the UK, a qualification currently exists for health trainers, costing £1250. If a similar cost applied to community health workers, 110,585 individuals could be trained for £138 m. In terms of recruitment, under far more challenging physical, environmental and public health constraints, Brazil recruited 250,000 community health workers. 14 In England, various community interventions using health trainers exist; many of these individuals could be redeployed in the proposed model. We therefore anticipate that actual numbers of new community health workers required, and consequent recruitment and additional salary costs, may be significantly less than those modelled.
However, implementation in the NHS would undoubtedly be complex, and integration with the current primary care workforce would require careful planning. While many existing community workers may be happy to take on this role, sensitivity will be needed to avoid conflict with roles of other professionals. There are other ongoing changes in the primary care workforce, including increased use of nurse practitioners, and introduction of physician associates and pharmacists in primary care. 45 This paper does not suggest replacement of these professionals. The focus of introduction of community health workers would be in the community as opposed to within general practices. In fact, community health workers are likely to help new primary care professionals, such as pharmacists and physician associates to work more effectively through improved communication, and early identification of health or social care problems.
In addition, while one of the aims of integration of community health workers is to support primary care and reduce general practitioner workload, it is possible that their proactive approach, with early alerting of general practitioners to possible problems may initially result in increased demand on general practitioners. Finally, this model of community health worker provision would require households to register with the same general practice. Although people living in the same household usually do, it might be difficult to make this a requirement.
Next steps should include pilot studies to explore acceptability and feasibility of introduction of community health workers in NHS primary care following the Brazilian model, allowing a reference case health technology assessment to be carried out. However, deployment at some scale will be necessary to see benefits in chronic disease management, immunisation and cancer screening uptake and other outcomes.
Conclusion
A traditional view of general practice emphasises relationship continuity, with patients having a general practitioner they and their families knew over many years. High workload, large practices, part-time working and access problems mean that this is not always a practical reality in the NHS. However, there may be lessons to learn from other models of primary care which provide some of the benefits of such continuity, while potentially improving access and reducing workload.
Systematic integration of community health workers at scale in NHS primary care could represent a timely and relatively rapidly implemented approach to the workload crisis. Chronic disease management, cancer screening and MMR immunisation uptake provide examples of potential benefits; there is a need for formal piloting to establish the impact of community health workers in NHS primary care.
Footnotes
Declarations
Funding
This article was supported by the Imperial NIHR Biomedical Research Centre and the NIHR CLAHRC for NW London. The views expressed are those of the authors and not those of the NIHR.