
Abstract
Objective
To report doctors’ early career preferences for emergency medicine, their eventual career destinations and factors influencing their career pathways.
Design
Self-administered questionnaire surveys.
Setting
United Kingdom.
Participants
All graduates from all UK medical schools in selected graduation years between 1993 and 2015.
Main outcome measures
Choices for preferred eventual specialty; eventual career destinations; certainty about choice of specialty; correspondence between early specialty choice for emergency medicine and eventually working in emergency medicine.
Results
Emergency medicine was chosen by 5.6% of graduates of 2015 when surveyed in 2016, and 7.1% of graduates of 2012 surveyed in 2015. These figures represent a modest increase compared with other recent cohorts, but there is no evidence of a sustained long-term trend of an increase. More men than women specified emergency medicine – in 2016 6.6% vs. 5.0%, and in 2015 7.9% vs. 6.5%. Doctors choosing emergency medicine were less certain about their choice than doctors choosing other specialties. Of graduates of 2005 who chose emergency medicine in year 1, only 18% were working in emergency medicine in year 10. Looking backwards, from destinations to early choices, 46% of 2005 graduates working in emergency medicine in 2015 had specified emergency medicine as their choice of eventual specialty in year 1.
Conclusions
There was no substantial increase across the cohorts in choices for emergency medicine. Policy should address how to encourage more doctors to choose the specialty, and to create a future UK health service environment in which those who choose emergency medicine early on do not later change their minds in large numbers.
Introduction
Emergency medicine (EM) is ‘a field of practice based on the knowledge and skills required for the prevention, diagnosis and management of acute and urgent aspects of illness and injury’. 1 Emergency physicians (EP) work in an extremely varied, time-pressured role, working in shifts in hospitals. 2
EM in the United Kingdom (UK) is currently under great staffing pressures and there are calls for a substantial increase in the number of consultants in the specialty. In 2017, the Royal College of Emergency Medicine (RCEM) wrote that emergency departments (ED) in the UK are ‘just coping’ in the face of increased demand from a rising population. 3 In the same year, a high percentage (73%) of doctors training in EM reported that the intensity of the work was ‘heavy’ or ‘very heavy’, compared with 37% of general practitioner trainees who felt the same about their work. 4 The pressures within ED may lead to staff dissatisfaction, attrition, burnout, and they also lower the attractiveness of EM as a career choice. 5 The RCEM has called for 2200 extra consultants in England and 100 extra training places each year for the next four years to achieve what it regards to be an adequate senior staffing level. 3 In 2016, according to the NHS Health Careers website, 6 there were 1586 full-time equivalent EM consultants and 1903 EM registrar trainees in England. The RCEM is therefore recommending a doubling of the number of consultants.
A previous study by us of UK-trained medical graduates, based on the graduates of 1993–2009, found that early career choices for EM were less predictive of career destinations than other specialty choices: only 26% of doctors who chose EM as a first choice one year after graduation still gave EM as a first choice five years after graduation. 7 Also, most doctors (73%) who pursued EM at five years after graduation had not given EM as their first choice of career at year one. 7
In this paper, we have updated findings from 1993–2009, and include data from new surveys of the graduates of 2012 and 2015. This paper reports doctors’ early career choices for EM, their eventual career destinations, and factors influencing their career pathways.
Methods
Our study included the medical graduates of 1993, 1996, 1999, 2000, 2002, 2005, 2008, 2009 (surveyed in their first year only), 2012 and 2015 from all medical schools in the UK. The only exclusions were the doctors whose contact details were unknown to the General Medical Council (GMC) and therefore not known by us (but note that, in order to practise medicine in the UK, doctors must by law be registered with the GMC). In all, 50,531 doctors were contacted one year after graduation. Multi-purpose questionnaires were sent towards the end of the first, third and fifth year after qualification to the doctors in, respectively, 10 cohorts (1993–2015), 8 cohorts (1993–2008 and 2012) and 7 cohorts (1993–2008). We also tracked doctors’ actual career progression in 6 cohorts (1993–2005) at 10 years after graduation. We used postal questionnaires and, more recently, also offered the option of web-based questionnaires. In each successive survey, the study population was the whole cohort as it was at qualification. Up to four reminders were sent for each survey. Further details of the methodology are available elsewhere. 8
We asked structured questions about the doctors’ preferences for future career specialty and about factors that have influenced their choice. We asked What is your choice of long-term career specialty?, inviting respondents to list up to three choices in order of preference and to indicate if any of the choices were of equal preference (which we termed ‘tied’ choices). Doctors described their specialty choices in their own words and we assigned each response to a specialty, and if necessary a subspecialty, according to a coding regime developed over many years and based on nationally recognised designation of specialties. Hospital medical specialties other than EM, whose training is managed by the Joint Royal Colleges of Physicians Training Board, were grouped together and named in this paper as ‘hospital physician specialties’ as a comparison group with EM doctors. This group included the following: General medicine, Cardiology, Dermatology, Endocrinology, Geriatrics, Nephrology, Neurology, Chest medicine, Rheumatology/Rehabilitation, Genito-urinary medicine, Gastroenterology, Vascular medicine, Tropical medicine, Clinical pharmacology, Infectious diseases and Occupational medicine.
We then asked How sure are you about the first choice given above? Respondents could rate their level of certainty about their career choice as ‘definite’, ‘probable’ or ‘uncertain’. In analysis we constructed a binary variable for certainty of choice by combining those who replied definite versus those who replied probable or uncertain.
Doctors were asked to indicate how much each of 15 factors had influenced their choice of specialty: ‘Wanting a career that fits my domestic circumstances’, ‘Wanting a career with acceptable hours/working conditions’, ‘Eventual financial prospects’, ‘Promotion/career prospects’, ‘Self-appraisal of own skills/aptitudes’, ‘Advice from others’, ‘Student experience of the subject’, ‘A particular teacher/department’, ‘Inclinations before medical school’, ‘Experience of jobs so far’, ‘Enthusiasm/commitment: what I really want to do’, ‘Availability of postgraduate training places’, ‘Availability of career posts’, ‘The requirement to repay student debt’ and ‘Other reasons’. These factors were based on an initial set used in our studies in the 1970s, modified when new themes were identified by us, as either arising in comments made to us by doctors or as recurring themes in the research literature. The doctors were asked to indicate whether each factor had influenced their choice of specialty ‘not at all’, ‘a little’, or ‘a great deal’. Some of these factors were only presented to doctors in specific surveys (years after graduation): this is shown in Table 3 by ‘n/a’.
Inclusion of second and third choices: grouped cohorts
EM was the first, second or third choice of career (across all cohorts) for 9.1% of 1993–2000 graduates and 10.5% of 2002–2009 graduates in year 1, and 9.5% of both sets of cohorts in year 3 (Table 1). More men than women specified EM, consistently, in both year 1 and year 3. Our latest data for the 2015 graduates in year 1 and the 2012 graduates in year 3 show rises in the levels of first, second and third choices for EM which are similar to the rises just described in first choices for EM, see Table 1 for details.
Individual cohorts, and trends across all cohorts studied
We reanalysed to explore the evidence for trend over the whole range of cohorts studied, accepting that grouping the cohorts as above is somewhat arbitrary.
Figure 1 shows EM first choices for men and women in individual cohorts surveyed from 1993 to 2015, 1, 3 and 5 years after graduation, as percentages of respondents with 95% confidence intervals indicated on the figure. Among men across the whole period studied, there was evidence of an upward linear trend across the cohorts in first, second and third choices for EM among men in all years after graduation, but there was no evidence for a trend among women.
Emergency medicine as a first choice (including ties).
Figure 2 in Appendix 1 shows equivalent results for all EM choices, whether first, second, or third in priority. For both Figures 1 and 2, p values for chi square tests of linear trend are given as footnotes.
Emergency medicine as any choice.
Certainty of career choice
Certainty of career choice by specialty chosen and cohort group: percentages whose career choice was definite 1, 3, and 5 years after graduation.
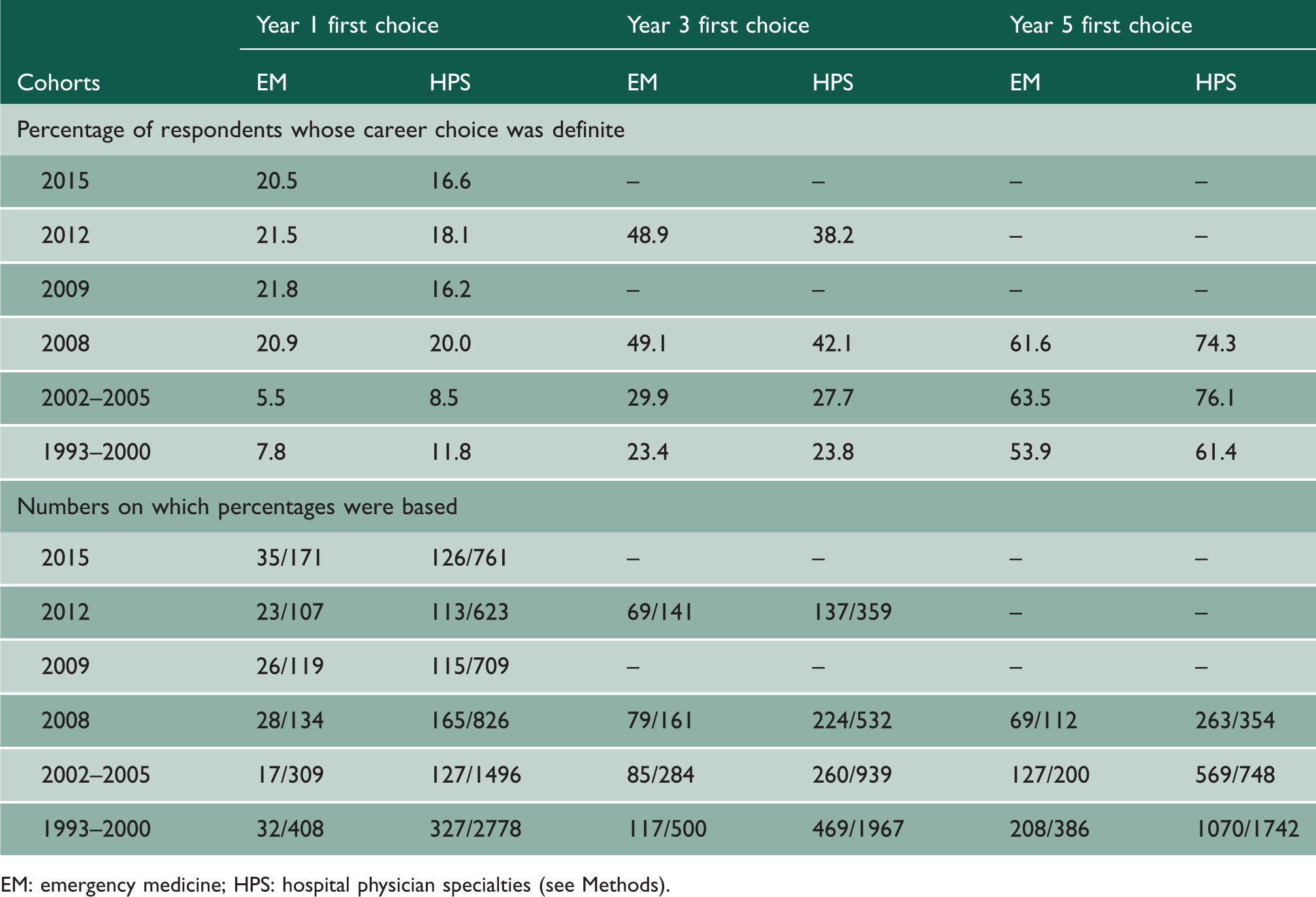
EM: emergency medicine; HPS: hospital physician specialties (see Methods).
Year 3 results showed higher percentages of certainty, with our most recently surveyed cohorts of 2008 and 2012 showing much higher figures than earlier cohorts. At year 5 the most recent EM data for the 2008 cohort showed that 62% were sure of their choice (Table 2). In the cohorts of 2009, 2012 and 2015 those selecting EM appeared surer of their choice than doctors choosing careers in the hospital physician specialties: this was not the case in earlier cohorts. There were no significant gender differences in certainty of choice for those selecting EM (p>0.05 in years 1, 3 and 5 using χ2 tests).
Factors influencing choice for EM
Among the most recently surveyed doctors at years 1, 3 and 5, the largest influences on choices for EM were in year 1 enthusiasm/commitment: what I really want to do (rated as a great deal of influence by 36% of those who chose EM), domestic circumstances (30%) and self-appraisal of own skills (30%); and in years 3 and 5 enthusiasm/commitment: what I really want to do (86% year 3, 80% year 5), experience of jobs so far (71%, 66%), and self-appraisal of own skills (51%, 64%); Table 3.
The pattern was similar for doctors who chose hospital physician careers, with the following exceptions. Doctors choosing EM in all years were less influenced by wanting a career with acceptable hours/working conditions (p<.001). Domestic circumstances were less influential on those choosing EM in years 1 and 3 (p < .001). In years 3 and 5 a particular teacher/department was less influential on those choosing EM (p < .01).
Looking forwards from early choices to later destinations (graduates of 2005)
Percentages of doctors in recent surveys who specified that each factor affected their career choice ‘a great deal’.

EM: emergency medicine; HPS: hospital physician specialties (see Methods). n/a denotes factors which were not included in specific surveys.
Year 1 data includes the 2012 and 2015 cohorts, year 3 data includes the 2012 cohort, and year 5 data includes the 2008 cohort.
p < .05; **p < .01; ***p < .001, comparing EM with hospital physician specialties, within each year, for each factor.
We used non-parametric tests (χ 2 tests, Mantel–Haenszel χ 2 tests for linear trend) to compare patterns of choices between subgroups and to explore trends in the data. When there were significant differences we used adjusted standardised residuals to identify unusually high or low cell counts for individual specialties or grouped specialties.
Ethics approval was obtained from the National Research Ethics Service, following referral to the Brighton and Mid-Sussex Research Ethics Committee in its role as a multi-centre research ethics committee (ref 04/Q1907/48 amendment Am02 March 2015).
Results
Response rate
In the first year after graduation, we contacted 50,531 registered doctors covering all 10 cohorts: 28,815 (57.0%) replied. The questionnaire was sent to 36,376 doctors in year 3 covering 8 cohorts and 21,764 (59.8%) responded. For five years after qualification, covering 7 cohorts, 17,897 from a possible 28,746 doctors (62.3%) replied.
Early career choices for EM: one, three and five years after graduation
First choice: grouped cohorts
Career preferences for emergency medicine: graduates of 2015 and 2012 compared with earlier cohorts (percentages of respondents).
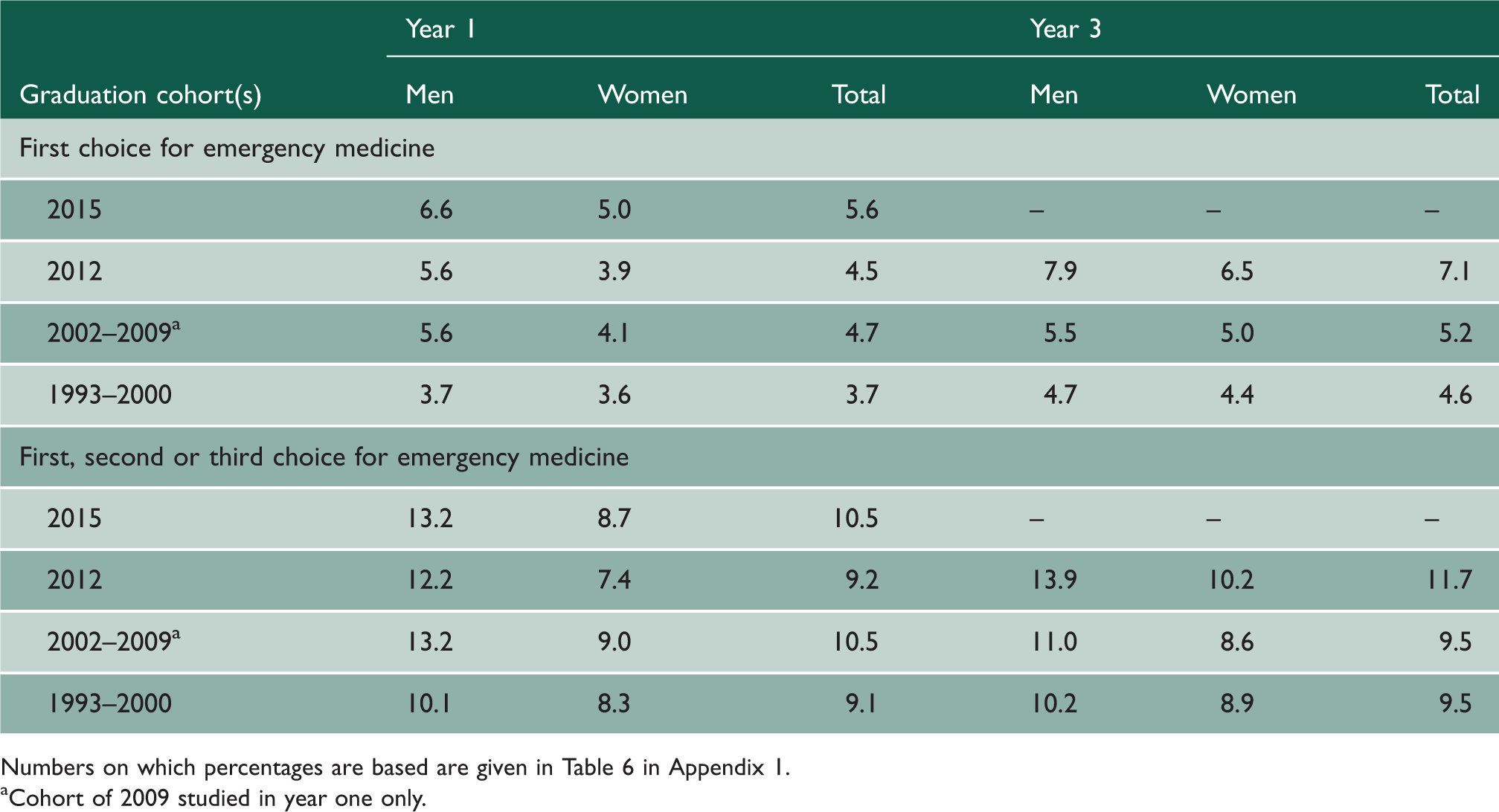
Numbers on which percentages are based are given in Table 6 in Appendix 1.
Cohort of 2009 studied in year one only.
Numbers and percentages of medical graduates whose original preference was for emergency medicine who eventually practised in each of four different destinations in year 10 (looking forwards from early preference to later destinations): 2005 cohort.

EM: emergency medicine; HPS: hospital physician specialties (see Methods).
‘Other clinical specialties’ includes the following: emergency medicine, anaesthesia, clinical oncology, surgery, paediatrics, pathology, psychiatry, and radiology.
Looking backwards from later destinations to early choices (2005 cohort)
Doctors who were working in emergency medicine in year 10, showing their career preferences in years 1, 3, and 5 (looking backwards from year 10 to preferences expressed in earlier years): 2005 cohort.

EM: emergency medicine; HPS: hospital physician specialties (see Methods).
Tied first choice or 2nd or 3rd choice.
Discussion
Main findings
EM has not shown a consistent rise in popularity as an early career preference over the period of our studies covering graduation years from 1993 onwards. The evidence for a rise is stronger among men than women, and stronger for the more recent graduation cohorts we have studied. However, doctors choosing EM in our most recent surveys in years 1 and 3, conducted in 2016 and 2015 respectively, were much more sure about their choice than their predecessors were who graduated a decade earlier. Nonetheless, our most recent year 5 survey, conducted in 2013, suggests that this increased certainty may not extend to the early years of specialist training.
Doctors’ enthusiasm and commitment, experience of jobs so far and self-appraisal of own skills were the biggest influences on choices for EM – as they also were for other specialties. EM choosers were less influenced by future financial prospects and experience of jobs so far than doctors choosing other careers.
Of the doctors who gave a first career preference for EM in years 1, 3 and 5, 18%, 43%, and 78%, respectively, were working in EM in year 10. These findings can be put in context by considering other specialties and their agreement between early choices and later destinations as reported by us elsewhere. 9 Considering doctors who expressed a career preference for general practice in years 1, 3 and 5, 82%, 92% and 96% were working in the specialty in year ten. The corresponding figures for early choices and later destinations for psychiatry were 75%, 93% and 97%. Those for radiology were 32%, 76% and 93%. Thus, EM was less of a sustained choice than choices for a number of other specialties. Men who were early choosers of EM were more likely than women to stick with their choice through to year 10, and women who were early choosers of EM were more likely than the men to be a GP by year 10. Viewed from year 10 destinations, looking back to early choices, three fifths of practising EPs in year 10 had not considered EM as a future career when they were in year 1.
Strengths and limitations
Numbers of respondents showing career preferences for emergency medicine, corresponding to percentages given in Table 1.

*Cohort of 2009 studied in year one only.
It is possible that non-response bias occurred, but we took steps to reduce this through sending frequent reminders to non-respondents. Doctors working in the UK but who did not obtain their primary medical qualification in the UK were not included in our study.
Comparison with existing literature
EM was the first choice of career for 4.4% of doctors one year after graduation for the 1993 to 2015 cohorts. Our last paper on EM choices, reporting on graduates from the qualification years of 1993–2002, found no trend across the cohorts in first choices for EM, but the latest data in that paper were from the 2009 cohort. 7 With the addition of the 2012 and 2015 cohorts there is now a clear upward trend in first choices among men (and women in year 3 only). This increase may be in part a consequence of concerted efforts by the RCEM in recent years to increase the attractiveness of the specialty.
More men than women specified EM as their first choice of career in year 1. This disparity in preferences widened for cohorts from 2009 onwards: 5.0% of women doctors in the 2015 cohort specified EM as their first choice compared with 6.6% of men. This gender difference is evident in other countries. Research in France found that women medical students’ belief that EM is better suited to men is negatively correlated with self-efficacy (‘belief in one’s ability to succeed’), which can lead to career avoidance. 10
One quarter of UK EM trainees surveyed in 2013 intended to work abroad (13%) or work eventually in a different specialty (10%). 11 Trainers and trainees in EM reported heavier workloads in 2016 compared with doctors in other specialties. 4 There is anecdotal evidence of high levels of attrition among EM trainees. 5 The high level of attrition can be attributed to the stressful working environment within EDs, which inevitably lowers the attractiveness of EM as a career choice to potential applicants.5,12,13
Key bodies responsible for EM training in the UK recently outlined a number of measures designed to reduce attrition in training: more support for each trainee, more funding for those trusts with the biggest training problems, and more flexible training. 5 These bodies also outlined strategies to improve the retention of EM doctors.
Possible future work
Our longstanding cohort studies of doctors are no longer supported by the Department of Health and are coming to an end. We hope that others will continue to use similar cohort methods to study the career progression of young doctors in vital specialties such as EM, to ascertain how larger numbers of new medical graduates can be encouraged to choose EM for their careers, and to understand what can be changed to create a future health service environment in the UK in which those who choose EM early on do not leave for an alternative specialty in large numbers as at present.
Declarations
Competing Interests
All authors want to declare: (1) financial support for the submitted work from the policy research programme, Department of Health. All authors also declare: (2) no financial relationships with commercial entities that might have an interest in the submitted work; (3) no spouses, partners, or children with relationships with commercial entities that might have an interest in the submitted work; (4) no non-financial interests that may be relevant to the submitted work.
Funding
The report is based on independent research commissioned and funded by the NIHR Policy Research Programme (project number 016/0118). The views expressed in the publication are those of the author(s) and not necessarily those of the NHS, the NIHR, the Department of Health, its arm’s length bodies or other government departments.
Ethics approval
This study was approved by the National Research Ethics Service, following referral to the Brighton and Mid-Sussex Research Ethics Committee in its role as a multi-centre research ethics committee (ref 04/Q1907/48 amendment Am02 March 2015).
Guarantors
TWL and MJG.
Contributorship
TWL and MJG designed and conducted the surveys. FS performed the analysis and wrote the first draft of the paper. All authors contributed to further drafts and all approved the final version.
Supplemental Material
sj-pdf-1-shr-10.1177_2054270420961595 - Supplemental material for Early career choices for emergency medicine and later career destinations: national surveys of UK medical graduates
Supplemental material, sj-pdf-1-shr-10.1177_2054270420961595 for Early career choices for emergency medicine and later career destinations: national surveys of UK medical graduates by Trevor W Lambert, Fay Smith and Michael J Goldacre in JRSM Open
Supplemental Material
sj-pdf-2-shr-10.1177_2054270420961595 - Supplemental material for Early career choices for emergency medicine and later career destinations: national surveys of UK medical graduates
Supplemental material, sj-pdf-2-shr-10.1177_2054270420961595 for Early career choices for emergency medicine and later career destinations: national surveys of UK medical graduates by Trevor W Lambert, Fay Smith and Michael J Goldacre in JRSM Open
Footnotes
Acknowledgements
We thank Ritva Ellison for data management and Alison Stockford for data entry. We are very grateful to all the doctors who participated in the surveys.
Provenance
Not commissioned; externally peer reviewed.
Data sharing statement
It may be possible for the authors to make tabulated data, produced in the course of this work but not included in the paper, available to interested readers on request.
Patient and Public Involvement
Patients were not involved in the design or any aspect of the study, by agreement with the funding body, since the study did not involve any medical or patient data. Results of the study are published in various papers in the peer-reviewed literature, and summary reports of our survey work are on our website at ![]()
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.