
Abstract
Summary
Objective
To report doctors' early career choices for obstetrics and gynaecology, their eventual career destinations and factors influencing their career pathways.
Design
Multi-cohort multi-purpose national questionnaire surveys of medical graduates in selected graduation years between 1974 and 2015.
Setting
UK.
Participants
UK-trained medical graduates.
Main outcome measures
Career specialty choices; certainty about specialty choice; factors which influenced doctors' career choices; career specialty destinations 10 years after graduation.
Results
Obstetrics and Gynaecology was the first choice of career for 5.7% of post-2002 graduates in year 1, 4.3% in year 3 and 3.8% in year 5. A much higher percentage of women than men specified Obstetrics and Gynaecology as their first choice: in year 1, 7.7% of women and 2.3% of men did so. The gender gap has widened since the 1970s and 1980s. In recent years, of those who specified Obstetrics and Gynaecology as their first choice in year 1 after graduation, 48% were working in Obstetrics and Gynaecology in year 10 (63% of men, 45% of women). Looking backwards from career destinations, 85% of doctors working in Obstetrics and Gynaecology in year 10 had specified Obstetrics and Gynaecology as a first, second or third choice of preferred career in year 1.
Conclusions
Interest in Obstetrics and Gynaecology among UK graduates appears to be exceeding the demand for new specialists. Policy needs to address risks of over-production of trainees and ensure that some graduates interested in Obstetrics and Gynaecology consider alternative careers. The large gender imbalance should encourage consideration of the reasons for men choosing Obstetrics and Gynaecology in falling numbers.
Introduction
Obstetrics and gynaecology in the UK 1 is facing workforce issues. The Centre for Workforce Intelligence reported in January 2015 that the Obstetrics and Gynaecology consultant workforce had grown by 53% over the decade to 2013, and that if this were to continue, workforce supply would outstrip patient demand leading to a substantial oversupply of trained Obstetrics and Gynaecology specialists by 2028. 2 They argued for an ‘immediate, substantial and sustained’ reduction in specialist trainee intake to reduce the risk of oversupply. The Royal College of Obstetricians and Gynaecologists reports a 30% attrition rate from Obstetrics and Gynaecology training, and that currently 15% of trainees consider leaving Obstetrics and Gynaecology. 3 Their latest survey of UK Obstetrics and Gynaecology consultants found reduced numbers of middle-grade staff, a consequent increase in working hours, and evidence of ‘increasingly variable consultant job plans’. 4 More recently, 88% of obstetric units reported difficulties in filling middle-grade rotas. 5 The situation is therefore somewhat confusing.
A 2003 study by us found that three-quarters of the UK graduates of 1999 who considered but then rejected Obstetrics and Gynaecology did so because of ‘poor career prospects’. 6 In Australia in 2010, Obstetrics and Gynaecology was ranked by medical students in the bottom three of 19 medical specialties for ‘lifestyle friendliness’. 7 A 2017 study in the UK reported that Obstetrics and Gynaecology trainees leave, or consider leaving, training for reasons which include low morale, excessive paperwork, poor support, difficulties with work–life balance and low job satisfaction. 8
A study by us of UK-trained graduates of 1974–2002 found falling percentages of doctors choosing Obstetrics and Gynaecology as their future career choice. 9 The decline was most evident among men. Obstetrics and Gynaecology was more popular among women than men doctors in Switzerland, Canada, the United States and New Zealand.10–13 Possible reasons for this gender disparity include a perception that women Obstetrics and Gynaecology trainees perform better in assessments,14,15 a perception that women patients prefer a female Obstetrics and Gynaecology doctor,16,17 and perhaps the possibility of gender bias and discrimination against men in training. 18
Our aim is to identify whether doctors' early career choices for Obstetrics and Gynaecology, their eventual career destinations and factors influencing career pathways have changed in recent cohorts of UK graduates.
Methods
Our study included contemporaneous surveys of the medical graduates of 1974, 1977, 1980, 1983, 1993, 1996, 1999, 2000, 2002, 2005, 2008, 2009, 2012 and 2015 from all medical schools in the UK. We sent postal and web-based questionnaires 1, 3, 5 and 10 years after qualification. We sent non-respondents up to four reminders. We have described the methodology used in detail elsewhere. 19
We asked structured questions about the doctors' preferences for future career specialty and about factors that have influenced their choice. These data were obtained at the first, third and fifth year after qualification from, respectively, 14 cohorts (1974–2015), 12 cohorts (1974–2008 and 2012) and 10 cohorts (1974–1980 and 1993–2008). We also tracked doctors' actual career progression in six cohorts (1993, 1996, 1999, 2000, 2002 and 2005) 10 years after graduation.
One, three and five years after graduation, we asked respondents What is your choice of long-term career specialty? Doctors were invited to list up to three choices in rank order and to indicate if any choices were of equal preference (‘tied’ choices). We then asked doctors How sure are you about the first choice given above? Respondents could rate their level of certainty about their career choice as ‘definite’, ‘probable’ or ‘uncertain’. In analysis, we produced a binary variable by combining those who replied definite or probable versus those who replied uncertain.
Doctors were asked to indicate how much each of 12 factors had influenced their choice of specialty: ‘Wanting a career that fits my domestic circumstances’, ‘Wanting a career with acceptable hours/working conditions’, ‘Eventual financial prospects’, ‘Promotion/career prospects’, ‘Self-appraisal of own skills/aptitudes’, ‘Advice from others’, ‘Student experience of the subject’, ‘A particular teacher/department’, ‘Inclinations before medical school’, ‘Experience of jobs so far’, ‘Enthusiasm/commitment: what I really want to do’ and ‘Other reasons’. The doctors were asked to indicate whether each factor had influenced their choice of specialty ‘not at all’, ‘a little’ or ‘a great deal’. Certain factors were only presented to doctors in specific years after graduation: omitted factors in particular surveys are indicated in tables by ‘n/a’.
We grouped hospital specialties other than Obstetrics and Gynaecology (see Appendix 1) as ‘other hospital specialties’, as a comparison group with Obstetrics and Gynaecology doctors. We used the term ‘hospital physician specialties’ to describe a second comparative subgroup (Appendix 1). We also created a comparison group which consisted of General Practitioners and Community Health doctors.
We used non-parametric tests (χ2 tests, Mantel–Haenszel χ2 tests for linear trend) to compare patterns of choices between subgroups and to explore trends in the data. When there were significant differences overall, we used adjusted standardised residuals to determine which subgroups were contributing most to the overall differences.
Results
Response rates
In the first year after graduation, we contacted 63,054 registered doctors covering all 14 cohorts: 39,411 (62.5%) replied. The questionnaire was sent to 48,899 doctors in year 3 covering all 12 cohorts: 31,466 (64.3%) responded. At five years after qualification, covering 10 cohorts, 24,970 from a possible 37,424 doctors (66.7%) replied. Year 10 destinations were available for 62.8% of year 1 responders (10,776/17,158), 65.2% of year 3 responders (10,742/16,473) and 68.6% of year 5 responders (10,651/15,528).
Early career choices for Obstetrics and Gynaecology: one, three and five years after graduation
First choice
In the graduation cohorts from 2005 to 2015, the levels of first choice for Obstetrics and Gynaecology were 5.7% (95% confidence interval: 5.3 to 6.1), 4.3% (3.9 to 4.8) and 3.8% (3.3 to 4.4), respectively, for years 1, 3 and 5 (Table 1). The corresponding figures for the cohorts from 1974 to 2002 were 3.6%, 2.8% and 2.4%. Percentages for individual cohorts from 2005 onwards are shown in Table 1, and Figure 1 shows the pattern for all cohorts from 1974. No trend was found in the year 1 and year 3 results for the cohorts from 2005 (p=.71 and .76, respectively).
Obstetrics and gynaecology as a first choice (including ties): graduates of 1974–2015. First choices for eventual career in obstetrics and gynaecology, contrasting cohorts who qualified in 2005–2015 with earlier cohorts: percentages and numbers (n/N) of respondents. Note: Year 3 results are based on the cohorts of 2005, 2008 and 2012 and year 5 results are based on the cohorts of 2005 and 2008. n/a: data not available (no survey undertaken).

A higher percentage of women than men, surveyed in year 1, have historically expressed a career preference for Obstetrics and Gynaecology and the rise in choices among women is clearly apparent in recent cohorts (Figure 1). Obstetrics and Gynaecology was the first choice of career in year 1 for 7.7% (7.1 to 8.2) of women who qualified in 2005–2015 compared with 4.9% (4.4 to 5.3) of women who qualified in 1974–2002. The figures for men were 2.3% (1.9 to 2.7) of 2005–2015 graduates and 2.5% (2.3 to 2.8) of 1974–2002 graduates. It is notable that one year after qualifying, from the 1999 cohort onwards, there was a large decline in choice for Obstetrics and Gynaecology among men, compared with women (for the 1999 cohort 0.5% of men chose Obstetrics and Gynaecology, and 3.4% of women; Figure 1). There was a similar decline in year 3 from the 1996 cohort onwards (i.e. survey time of 1999). Overall, the gender gap in choices for Obstetrics and Gynaecology increased over time (Figure 1).
In years 3 and 5, the large gender difference among the cohorts of 2005–2015 seen in year 1 was sustained (Figure 1): 5.8% (5.2 to 6.5) of women chose Obstetrics and Gynaecology compared with 1.9% (1.4 to 2.3) of men in year 3; and in year 5, 4.9% (4.1 to 5.7) of women and 2.0% (1.4 to 2.7) of men did so. In the cohorts of 1974–2002, the gender difference was less pronounced: in year 3, 3.5% of women and 2.1% of men chose Obstetrics and Gynaecology; in year 5, 2.9% of women and 1.8% of men did so.
Inclusion of second and third choices
In the cohorts of 2005–2015, Obstetrics and Gynaecology was the first, second or third choice of career for 8.9% of graduates in year 1, 5.3% in year 3 and 4.4% in year 5. The corresponding percentages for the cohorts of 1974–2002 were 7.1%, 3.9% and 2.9%. A higher percentage of women than men specified Obstetrics and Gynaecology in all years (Appendix 2).
Certainty of career choice
Certainty of career choice by specialty chosen: comparison between doctors who expressed a first preference for each specialty group at 1, 3 and 5 years after graduation: graduates of 2005–2015.
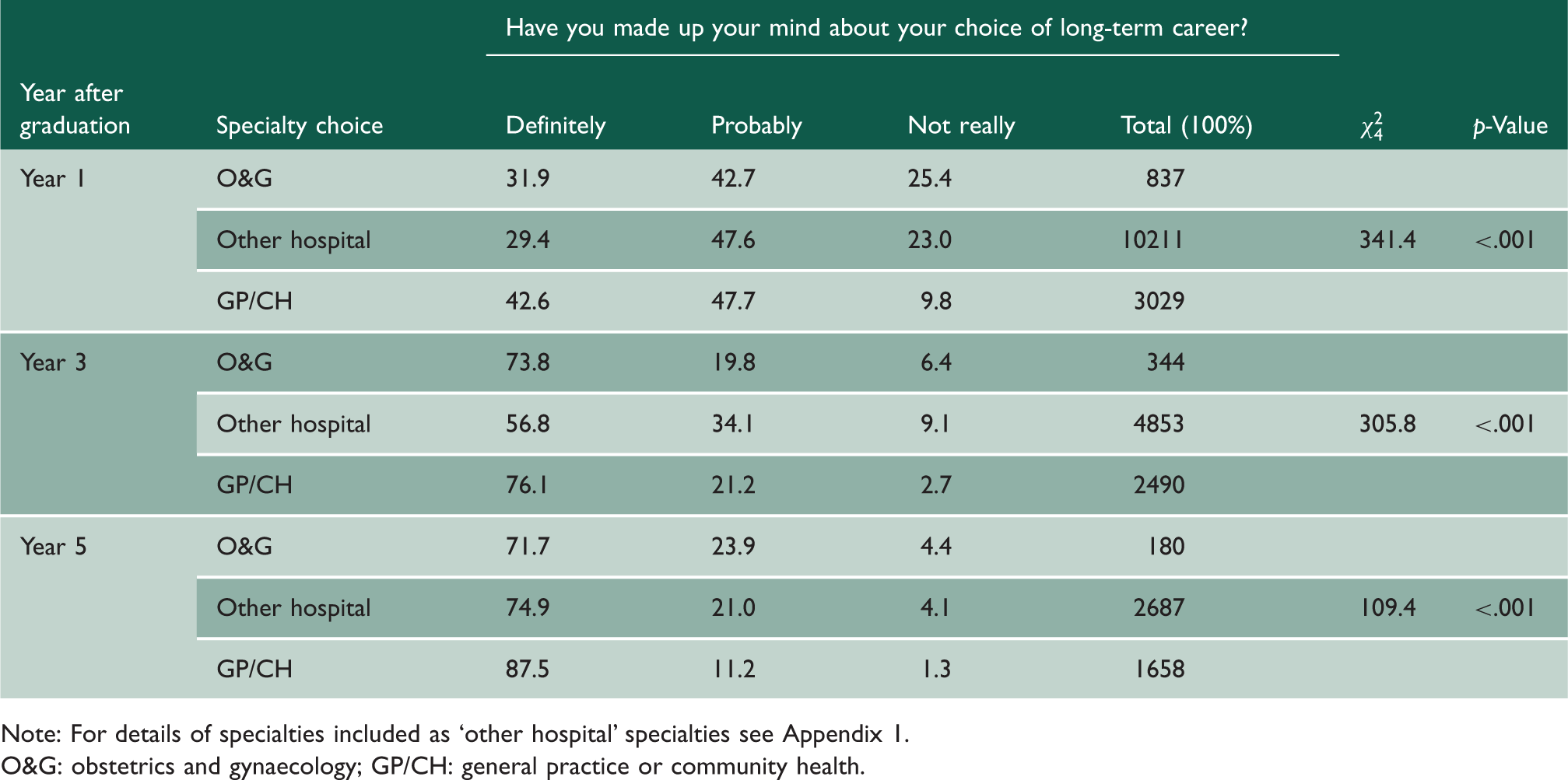
Note: For details of specialties included as ‘other hospital’ specialties see Appendix 1.
O&G: obstetrics and gynaecology; GP/CH: general practice or community health.
In year 1, there was a significant upward trend across the cohorts in the certainty of those doctors choosing Obstetrics and Gynaecology (p < 0.001): the level of certainty rose from 16.3% for the 2005 cohort to 33.4% for the 2015 cohort. There was no significant trend in years 3 and 5.
Factors influencing choice for Obstetrics and Gynaecology
Doctors who specified that each factor affected their career choice ‘a great deal’: percentages of graduates of 2005–2015.

Note: p-Values are computed comparing O&G with aGP/CH and bother hospital specialties, within each year, for each factor (p < .01).
For details of specialties included as ‘other hospital’ specialties see Appendix 1.
Numbers on which percentages are based vary due to item non-response, but are at least as large as the following: year 1 – O&G 843, Other hospital 10,307, GP/CH 3053; year 3 – O&G 347, Other hospital 4916, GP/CH 2520; year 5 – O&G 182, Other hospital 2735, GP/CH 1700.
O&G: obstetrics and gynaecology; GP/CH: general practice or community health.
Compared with those who chose other hospital specialties, those who chose Obstetrics and Gynaecology scored higher on student experience of the subject and enthusiasm/commitment: what I really want to do, and lower on wanting a career with acceptable hours/working conditions in year 1; in years 3 and 5, those who chose Obstetrics and Gynaecology scored higher on student experience of the subject, and lower on wanting a career that fits my domestic circumstances and wanting a career with acceptable hours/working conditions.
Compared with those who chose general practice or community health, those who chose Obstetrics and Gynaecology scored higher on student experience of the subject, particular teacher/department and enthusiasm/commitment: what I really want to do, and lower on wanting a career that fits my domestic circumstances, wanting a career with acceptable hours/working conditions and eventual financial prospects in years 1 and 3; in years 3 and 5 those who chose Obstetrics and Gynaecology also scored higher on experience of jobs so far.
Looking forwards from early choices to later destinations (graduates of 1993–2005)
Early career choices for Obstetrics and Gynaecology in years 1, 3 and 5 were compared with three career destination groups in year 10 after qualification (Appendix 3). Of those doctors who chose Obstetrics and Gynaecology in year 1, 48% were working in Obstetrics and Gynaecology in year 10. More men (63%) than women doctors (45%) who chose Obstetrics and Gynaecology in year 1 were working in Obstetrics and Gynaecology in year 10. Of those doctors who chose Obstetrics and Gynaecology in years 3 and 5, 73% and 86%, respectively, were working in the specialty at year 10.
Looking backwards from later destinations to early choices (graduates of 1993–2005)
Looking backwards, 85% of doctors practising in Obstetrics and Gynaecology in year 10 had considered Obstetrics and Gynaecology as a future career in year 1, whether as first, second or third preference (Appendix 4). This figure rose to 91% for year 3 and 93% for year 5.
Discussion
Main findings
There has been resurgence in first choices for Obstetrics and Gynaecology among doctors who graduated since 2005. In every cohort from 1974 to 2015, in every survey, more women than men specified Obstetrics and Gynaecology as their first choice of career. The overall increase in Obstetrics and Gynaecology choices in recent cohorts is due to a large increase among women: choices for Obstetrics and Gynaecology among men have remained static and have even fallen in some cohorts. Between the mid- and late 1990s, there was a collapse in the percentages of men choosing Obstetrics and Gynaecology in the early years after qualification. As the proportion of women entrants to medical school, and therefore in successive cohorts of doctors, has risen, increased interest among women in Obstetrics and Gynaecology careers has more than compensated for the static interest in the specialty among men.
One-third of doctors who specified Obstetrics and Gynaecology as their first choice were definite about their choice of long-term career in year 1. Men were more definite about their choice for Obstetrics and Gynaecology than women in year 1. The most recent cohorts have become much more definite about their choice of Obstetrics and Gynaecology as a career than older cohorts.
Of early choosers of Obstetrics and Gynaecology (in year 1), one-half were working in Obstetrics and Gynaecology in year 10, and one-third were working as GPs. Men early choosers of Obstetrics and Gynaecology were more likely than women to stay with their choice by year 10. Most doctors practising Obstetrics and Gynaecology in year 10 had specified Obstetrics and Gynaecology as a future career in year 1.
The gender disparity in choices for Obstetrics and Gynaecology has resulted in a remarkably large numerical difference between the numbers of men and women working in Obstetrics and Gynaecology in the 1993–2005 cohorts 10 years after graduation. Among our respondents, across six graduation cohorts, there were just 57 men in Obstetrics and Gynaecology in year 10 compared with 197 women.
Strengths and limitations
This study was a large-scale, national study of all UK-trained medical graduates. The response rates were good: 63% one year after graduation, 64% in year 3 and 67% in year 5. We asked doctors to specify their choices and reasons for those choices at each time point, thus not relying on retrospective data or rationalised recollection. The longitudinal nature of the data allowed us to follow the graduates to their eventual career destination.
As with all questionnaire studies, response bias is possible, but we sought to reduce this by sending frequent reminders to non-respondents, and emphasising that our research group was independent from government bodies. Also, because we have followed these cohorts for many years (some since the 1970s), we have an established presence among these cohorts of doctors. This study did not include doctors who graduated outside the UK.
Comparison with existing literature
Our previous study, which included up to the 2002 cohort, noted a decline in choices for Obstetrics and Gynaecology in the 1990s (from 4.2% of 1996 qualifiers to 2.2% of 1999 qualifiers). 9 The present study looked at later cohorts and found a steady rise in choices for Obstetrics and Gynaecology (peaking at 6.4% for the 2015 cohort). One small-scale study of students in a Welsh medical school found that 4% were considering Obstetrics and Gynaecology. 20 These students would correspond to the 2012 cohort in our study – where we found that a similar proportion of 5.6% were considering Obstetrics and Gynaecology. A study of Swiss doctors found that 5.9% of fourth year residents (2001 cohort) wanted a career in Obstetrics and Gynaecology 10 : 2.3% of our 2002 cohort, also surveyed in 2005, specified Obstetrics and Gynaecology as a first choice. With different workforce pressures and incentives in different countries, it is to be expected that the percentages would be different.
In our surveys, more women than men specified Obstetrics and Gynaecology as their first choice of career. For example, of the 2015 cohort, 7.5% of women doctors specified Obstetrics and Gynaecology as their first choice compared with 2.2% of men. The same disparity has been found in other countries,10–13 for example, in 2005 9.6% of Swiss fourth year women residents aspired to choose Obstetrics and Gynaecology compared with 1.7% of men. 10 Whilst gender is an important factor in career decisions, other predictors of choosing Obstetrics and Gynaecology include positive experience during undergraduate attachment, good role models, desire for a ‘narrow scope of practice’ and ethnicity.12,13,21 Other research has indicated that career motivation and life goals are also factors that influence specialty choice. 10
Our study found an upward trend across cohorts in choices for Obstetrics and Gynaecology among women, notably from the 2005 cohort onward, and a downward trend among men. The collapse in the popularity of Obstetrics and Gynaecology among men in the late 1990s could be linked to workforce issues in Obstetrics and Gynaecology at the time: a lack of consultant expansion and a reduction in training numbers.9,22,23 We know from our previous research that men, when deciding on a career, rate ‘promotion and career prospects’ and ‘eventual financial prospects’ as more important than women do. 24 A study in the United States found a decline in choices for Obstetrics and Gynaecology over time between 1997 and 2004, but that the proportion of women choosing Obstetrics and Gynaecology rose. 13
Of early choosers of Obstetrics and Gynaecology, one-third were not working in Obstetrics and Gynaecology in year 10. This figure is very similar to the 30% of UK Obstetrics and Gynaecology trainees who do not finish their training programme. 3 Most doctors practising in Obstetrics and Gynaecology as careers had specified Obstetrics and Gynaecology as their future career one year after graduation. A Canadian study found that doctors who ultimately chose a career in Obstetrics and Gynaecology had, at the start of medical school, specified Obstetrics and Gynaecology as one of their first career choices. 12
Interpretation and conclusions
In our introduction, we noted that the Centre for Workforce Intelligence stocktake report showed oversupply of doctors wishing to work in Obstetrics and Gynaecology, relative to patient demand. The Centre for Workforce Intelligence report recommended reductions in training places, and by implication in subsequent consultant posts: assuming their analysis to be accurate, it does not sit comfortably alongside the substantially increased level of interest we report here in Obstetrics and Gynaecology in recent cohorts, particularly among women. Policy has to address this mismatch, firstly to ensure that large numbers of doctors do not embark on a training path which will ultimately not lead to a consultant opportunity, and secondly to ensure that those undertaking Obstetrics and Gynaecology training are able to maximise the benefit of their training even if it means that they have to modify their ambitions and redirect them to an alternative specialty where their transferable skills and training can be utilised to the best effect. Reasons for the current high attrition rate of Obstetrics and Gynaecology trainees need to be investigated and addressed. Work still needs to be done by medical educators, the Department of Health, Health Education England and the Royal College of Obstetricians and Gynaecologists to attain a balance between junior doctors' aspirations for careers in Obstetrics and Gynaecology, availability without over-production of training programmes, numbers of specialist trainees and numbers of likely consultant posts, to avoid under-supply or over-production of the workforce in Obstetrics and Gynaecology.
There are misperceptions that female patients prefer female Obstetrics and Gynaecology doctors (52% have no preference), and that female Obstetrics and Gynaecology doctors perform better than men.16,17 Despite the increase in women in medicine and despite the potential for an oversupply of women Obstetrics and Gynaecology doctors, the specialty should remain a viable career to all doctors, irrespective of gender.
There are areas for further research which are beyond the scope of this study. These could include consideration of differences between graduates of different schools, perhaps related to variations in the duration and availability of undergraduate attachments in Obstetrics and Gynaecology; whether undertaking an Obstetrics and Gynaecology placement within Foundation training influences career choice; and whether increased opportunities to train and work less than full time have made a difference to Obstetrics and Gynaecology recruitment.
Footnotes
Declarations
Acknowledgements
We thank Ritva Ellison for data management, and Janet Justice and Alison Stockford for data entry. We are very grateful to all the doctors who participated in the surveys.
Provenance
Not commissioned; peer-reviewed by Joe Rosenthal.