
Abstract
Objectives
To study early and eventual career choices for nephrology among UK medical graduates and investigate factors which influenced career preferences.
Design
Self-completed survey questionnaires mailed to medical graduates 1, 3, 5 and 10 years after graduation.
Setting
United Kingdom.
Participants
UK medical graduates in 15 year-of-qualification cohorts between 1974 and 2015.
Main outcome measures
Early career specialty choices, career specialty destinations at 10 years and ratings of factors affecting career choices.
Results
Around 0.4%–1.1% of these junior doctors expressed a career preference for nephrology, varying by year of qualification and years after qualification. Among all graduates of 1993–2002 combined, 0.4% expressed a career preference for nephrology 1 year after qualification rising to 1.0% in year 5. Among graduates of 2005–2008, the corresponding figures were 1.0% in year 1 falling to 0.7% in year 5. Only 18% of doctors who chose nephrology in year 1 eventually became nephrologists. Of doctors who were practising as nephrologists for 10 years and more after qualification, 74% of the women and 56% of the men had decided to pursue a career in nephrology by year 5 after qualification. ‘Enthusiasm/commitment’ had a great deal of influence on those who chose nephrology, for all cohorts and all years studied.
Conclusions
The most recent data suggest that the proportion of young doctors who sustain an interest in nephrology through the early postgraduate training years may be lower than among their predecessors. Efforts are needed to reverse the declining trend and increase interest in nephrology.
Background
Kidney disease, whether acute kidney injury or chronic kidney disease, is an important global public health challenge facing health systems. 1 It is a major cause of mortality and morbidity related to chronic disease, which is associated with substantial healthcare resource use. 2 For instance, in 2014 in England, 2.6 million adults aged over 16 years were living with chronic kidney disease stage 3–5, which constitutes 6.1% of population of this age group. 3 It was estimated that chronic kidney disease imposed 1.44–1.45 billion pounds in 2009–2010 on the English NHS (equivalent to nearly 1.3% of all NHS budget in that year). 4 The global burden of chronic kidney disease continues to increase as a consequence of higher detection rates, population growth and greater life expectancy. 5
The status of kidney care varies over time and across world regions. The renal workforce plays a pivotal role in kidney care delivery and includes nephrologists, primary care physicians and nurse practitioners who hold different levels of responsibility. Globally, nephrologists are the main specialist medical providers responsible for both chronic kidney disease (93%) and acute kidney injury (95%) care, regardless of national income level. 1 The density of nephrologists is variable across countries, which has an impact on the availability and delivery of care for patients. 5 Most countries (74%) reported shortages in nephrologists. Overall, the mean number of nephrologists and nephrology trainees was 8.83 and 1.87 per million population (pmp), respectively. 1 Africa, South Asia and Oceania & South East Asia have the lowest nephrologist density around the world (less than 5 pmp). 1 Correspondingly, Ireland, Turkey and the UK (8.5 pmp) have the lowest ratio among European nations. 5
The underpinning reasons for the shortage of nephrologists in developed countries are different from those in developing countries. In developed nations, researchers report declining interest in nephrology among trainees because the field is ‘unappealing’, demanding and has poor work–life balance with less remuneration compared to other specialties such as dermatology.5,6 Conversely, in developing countries, lack of training programmes, undersupply of expensive treatment such as dialysis and transplantation, and migration of health professionals including nephrologists from developing to developed countries are the main causes for the current paucity of nephrologists.6,7
A nephrology training programme is available in 96 out of 121 countries (79%) with variations in structure and length. Most training programmes (86%) take two to four years. Nephrology training can follow training in general internal medicine, be a dedicated training after qualification, or be a mix of both depending on region and/or training centre, or follow some other structure. 1 In the UK, the nephrology training programme is usually delivered within five years including two years Core Training in General Internal Medicine (Acute Medicine), delivered either through the core medical training programme or the acute care common stem, followed by three years of clinical nephrology and runs up to the award of a Certificate of Completion of Training. 8 According to the latest figures, in 2017 in England, 376 medical registrars and 536 consultants were working in the renal field. 9
A better understanding of factors that motivate trainees to choose nephrology as a specialty is essential. This will allow achievement of optimal criteria for admission to renal specialty training programmes and ensure that talented trainees are attracted and retained in nephrology. In turn, this would be of great benefit not only for health systems but also for trainees and medical graduates who intend to pursue a career in nephrology.
To date, little research has been carried out that particularly seeks the views of medical graduates at different points of time regarding a career choice for nephrology. In order to bridge this knowledge gap, we describe the findings from our surveys which identify trends for nephrology choice over different cohorts and examine factors affecting career choices for nephrology.
Methods
Data collection
The UK Medical Careers Research Group has undertaken longitudinal national surveys of cohorts of medical school graduates since 1974. The design and sampling frame of surveys aim to recruit and follow all medical graduates from all UK medical schools in particular graduation years, identified by registration with the General Medical Council. The subjects were asked to answer multi-purpose questionnaires by post or online at different time slots: one, three and five years after qualification and longer intervals thereafter. Thus the surveys were contemporaneous, with longitudinal follow-up of the cohorts. Non-respondents in each survey year were sent up to four postal or email reminders. Further details of the design and survey methods are reported elsewhere. 10
For the present paper, we utilised data gathered from 15 cohorts, comprising the UK medical graduates of 1974, 1977, 1980, 1983, 1993, 1996, 1999, 2000, 2002, 2005, 2008, 2009, 2011, 2012 and 2015. Based on the study aims, three main areas of investigation are: career choice, influencing factors and career destination. Relevant data for addressing the two former issues were extracted from 15 cohorts (1974–2015), 12 cohorts (1974–2008 and 2012) and 10 cohorts (1974–1980 and 1993–2008) at the first, third and fifth year after qualification, respectively. Ten years after graduation, data on qualifiers from 1993 to 2002 (5 cohorts) were used for identifying destinations.
Research instrument
The survey instrument used in this study was developed and revised over many years to allow the survey to be self-completed and to reflect doctors' careers and concerns. Participants received a research questionnaire containing both open and closed questions exploring demographic information, career choice and plans and employment history.
We explored participants’ career choice by asking ‘What is your choice of long-term career?’, giving boxes for entering up to three specialty choices in order of preference. Respondents were also asked about the level of certainty of their specialty choices and were offered three options: ‘definite’, ‘probable’ and ‘uncertain’. In all surveys, 13 factors were listed and participants were asked to assess their impact on their choice of future career. A three-point response scale was provided: ‘not at all’, ‘a little’ and ‘a great deal’.
Data analysis
To stabilise cohort variations, for most analyses, individual cohorts were merged into three cohort groups: graduates of 1974–1983, graduates of 1993–2002 and graduates of 2005–2015.
For analysing specialty choices, choices with equal preference were considered as ‘tied’ choices, e.g. if a participant's first choice was both for nephrology and for another named specialty, we specified it a tied first choice for nephrology.
In our analysis, the term ‘other hospital physician specialties’ refers to specialties, except nephrology, in which the consultants are hospital physicians. In the UK, trainees in these specialties usually complete Core Medical Training prior to entering a Specialty Training programme.
Bivariate cross-tabulation with χ2 test was used for assessing trends over time and statistically significant differences between two variables. The Mantel–Haenszel linear-by-linear χ2 test was employed for linear trend over cohorts. Confidence interval widths were 95% for all calculations. The data were analysed by means of the IBM SPSS Statistics for Windows, V22 11 and Microsoft Excel (2010).
Results
Response rate
Overall, 15 surveys were included in this paper; 69,670 registered doctors were contacted in the first year after qualification, of whom 40,412 responded (58.0%). Correspondingly, the response rate was calculated to be 64.3% (31,466/48,899) in year 3 and 66.7% (24,970/37,424) in year 5.
Early career choices for nephrology: one, three and five years after graduation
First choices 1, 3 and 5 years after graduation for eventual careers in nephrology.

Note: Linear trend and heterogeneity have been calculated using the columns headed 1974–1983, 1993–2002 and 2005–2015. Linear trend across cohorts (
a2005, 2008 and 2012 cohorts only.
bExcludes 1983 cohort in year 5.
c2005 and 2008 cohorts only.
Online Appendix Table 1 presents the percentages of doctors in each individual cohort who expressed a preference for an eventual career in nephrology. There was a wide range of variation in choices in terms of cohort and years after qualification. For instance, in year 5 first preferences for nephrology varied from 1.3% in the 2000 cohort to 0.2% in the 1974 and 1977 cohorts.
Nephrology as a career choice for male and female doctors
Considering all cohorts and years, nephrology has been a more popular career choice among men than women; however, the size of the observed gap has varied according to cohort and time since qualification (Figure 1).
Percentage of doctors making nephrology their first career choice 1, 3 and 5 years after graduation. Blue: male. Red: female.
Comparison between cohort groups in year 1 revealed an increase over time in the percentage of both male and female doctors choosing nephrology as their first preference. In year 3, nephrology as a first choice of eventual career grew steadily in popularity for men but for women showed a rise among 1993–2002 graduates, then a substantial fall among 2005–2012 graduates. The first choices for nephrology in year 5 for both genders had an increase in cohorts 1993–2002, and then a decline in cohorts 2005–2008.
Online Appendix Figure 2 shows nephrology as any career choice (i.e. first, second or third choice) for both male and female doctors. The observed trend is similar to the trend in nephrology as first choice.
Certainty of choice
Percentages scoring each factor as having a great deal of influence on their career choice.

OHPS: other hospital physician specialties.
*p < .01; **p < .001, comparing nephrology with other hospital physician specialties, within each year, for each factor.
Factors influencing career choice
The doctors were asked to provide a view on the importance of 13 different factors affecting the choice of career specialty. A number of factors were identified by most respondents as having a great deal of importance (Table 2).
The highest percentage of doctors whose first choice of career was nephrology in year 1 (60.7%) and 5 (81.7%), scored ‘enthusiasm/commitment’ as having a great deal of influence. Although the importance of this element increased over time, in year 3, it ranked as the second most important influence (65%) after ‘experience of jobs so far’ (75%) for aspiring nephrologists. In all three survey years, ‘hours/ working conditions’ was the only factor that was significantly less important (p < 0.001) for aspiring nephrologists than aspiring other hospital physician specialists.
Comparing men and women, ‘enthusiasm/commitment’ was the most important consideration for men. The second important driver for men was ‘self-appraisal’ in year 1 (45%) and ‘experience of jobs so far’ in the following years. For women, the two most important motivators were ‘enthusiasm/commitment’ (60%) and ‘a particular teacher/department’ (55%) at year 1 and ‘experience of jobs so far’ and ‘enthusiasm/commitment’ in the following years.
In comparison, for doctors seeking a career in other hospital physician specialties, on all survey occasions and for both genders, ‘enthusiasm/commitment’ and ‘experience of jobs so far’ were respectively identified as the first and second powerful drivers of specialty choice. The importance of these factors continued to increase as time passed from graduation. Women scored more highly for these factors than men.
Overall cohorts and years, financial issues such as ‘future financial prospects’ and ‘financial circumstances whilst training’ were perceived to be unimportant influences.
Comparing early choice with eventual destination
Looking forward from early choice to eventual destinations
Career destinations for nephrology at 10 years looking forward from early choices.
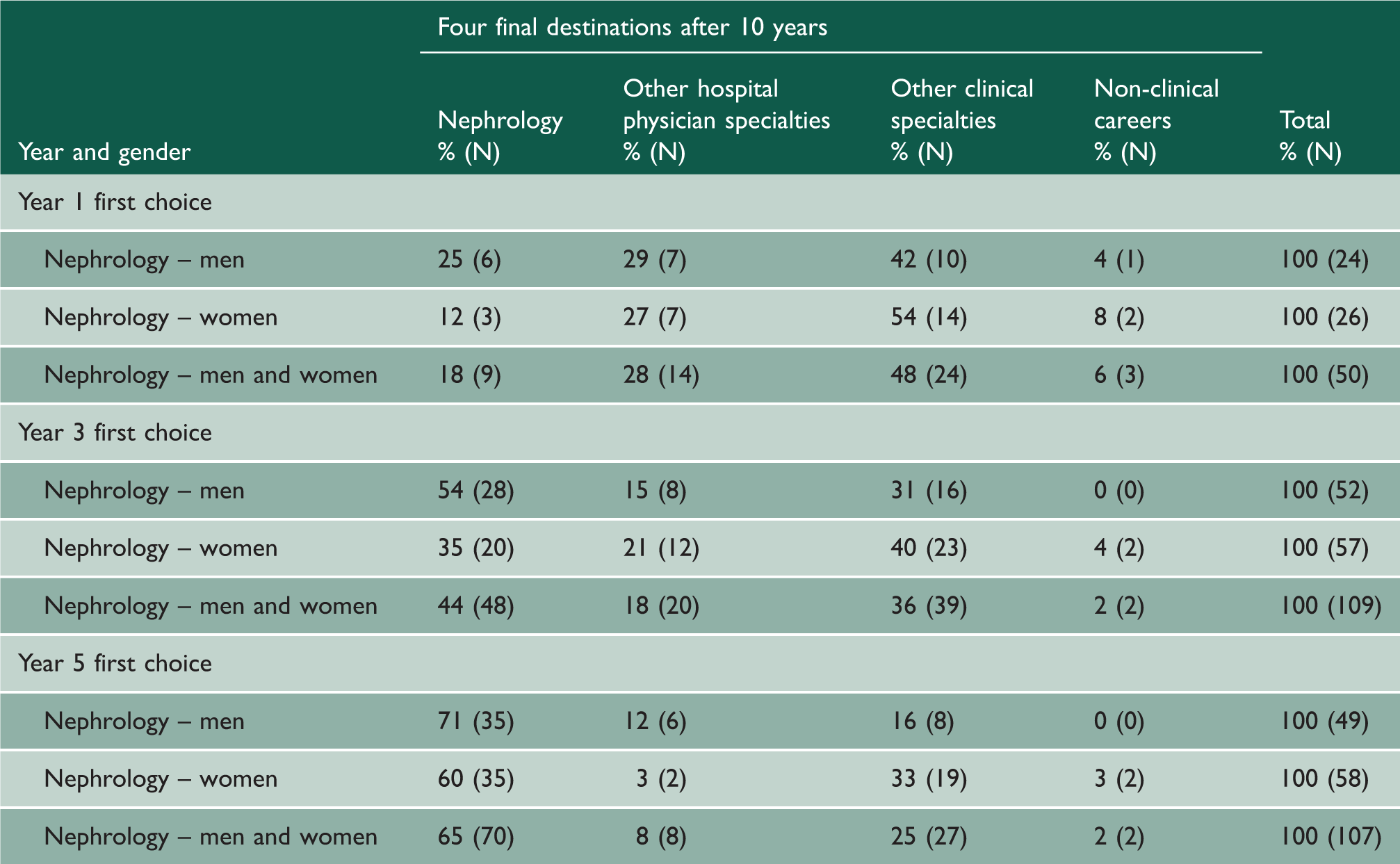
Male doctors were significantly more likely than female doctors to maintain their early career choice and become practising nephrologists. For instance, 71% of men and 60% of women whose early career choice in year 5 was nephrology eventually progressed into nephrology.
Looking backward from career destinations to early choices
Original career choices of doctors practising as nephrologists in year 10 (looking backward).

When looking back to year 1 and 3 after graduation, more male than female nephrologists had specified nephrology, but a higher percentage of female than male nephrologists had specified nephrology as their preferred career choice in year 5 (75% vs 56%).
The commonest career choice in year 1 for practising nephrologists had been other hospital physician specialties (69%).
Discussion
Main findings
To our knowledge, this is the first nationwide survey in the UK to examine the trend of choices for career in nephrology and report on the influencing factors among medical graduates at time intervals.
More medical graduates have initially chosen nephrology as a career recently compared to previous generations, but nephrology choices among the most recent medical graduates we surveyed did not increase as time passed from graduation. This failure to maintain early choice, which was unlike that seen in earlier cohorts, requires further investigation to reveal underlying reasons.
A gender difference was reported in this study, with men more likely than women to specify nephrology as their first choice. The gender gap almost disappeared for graduates of 1993–2002 but returned for recent graduates from 2005.
Only one-seventh of doctors who chose nephrology in year 1, and a fifth in year 3, were sure about their choice. Workforce planners and educational decision makers may find it worthwhile to investigate why so few of those who express a choice for nephrology at this stage are firmly committed to their choice.
The findings highlighted that doctors who chose nephrology were mostly influenced by enthusiasm and commitment to the specialty, by their work experiences in the specialty, or by a particular teacher or department. The latter factor was more important in year 1, and in the following years, work experience was more influential. Intending nephrologists were not motivated by financial issues.
Our data on the timing of specialty choice confirm that most of the decision-making about wanting a career in nephrology took place several years after qualification. Doctors who, in the early years after graduation, intended a career in nephrology seemed to change their minds early on but this also continued even after year 5. It would be beneficial to investigate why they did not continue to aspire to a career as nephrologists.
A low level of correspondence was identified between being a nephrologist and having made early career choices for nephrology: many eventual nephrologists did not choose it in years 1 or 3.
Comparison with other research
UK-based studies
Our findings signified a concern regarding the willingness of recent graduates to enter nephrology despite a low competition rate for a UK specialty trainee position in renal medicine (1.37 candidates per post in 2016). 12 Gender disparities in choices for nephrology in our study were small, but it does seem to have more appeal for men than women. Similar papers related to these cohorts have been published in other specialties.13–15
Regarding influencing factors, enthusiasm and work experience were important for both intending nephrologists and doctors aspiring to other hospital physician specialties, which have a common training entrance pathway, i.e. Core Medical Training. 8
One advantage of nephrology is that, unlike specialties such as surgery, doctors who make late decisions can revise their career plans and enter nephrology training with ‘transferable skills’ from general physician practice, probably with realistic information derived from their work experiences.16,17
Studies outside the UK
Gender disparity has been reported previously in choices for nephrology in various countries outside the UK. 5 Possible reasons for this issue are the paramount importance for many women of balancing career and family 18 stemming from stereotypical social roles for men and women 19 ; nephrologists' out-of-hours working time commitments19–21; possible pay differentials in some countries, which disadvantage female nephrologists 22 ; course difficulty and poor teaching 23 ; unattractive practice environment of nephrology; and the existence of specialties such as anaesthesiology and emergency medicine which may be regarded by some as more life-style friendly. 5 Poor income in nephrology generally was also cited as a disincentive by researchers in Australia 21 and Spain. 24
In many countries, nephrologists seem to make their specialty decision several years after qualification. Some studies outside the UK have suggested that this might reflect an unfavourable perception of nephrology including difficulty in obtaining posts, 20 undesirable level of income,21,25 long work hours21,25 and complexity of renal patients.21,23
Implications
Women make up 51% of higher specialty trainees in renal medicine in the UK. 26 Work–life balance is an important determinant of career choice among female doctors, 27 and concerns about long work hours and heavy workload in nephrology were frequently reported in other studies.19–21 Workforce planners and educational providers can support nephrologists through offering family friendly strategies such as flexibility in training and working hours. The NHS Improving Working Lives initiative from 2000 aimed to promote a healthy work–life balance among its staff including doctors, 28 but it is unclear that its implementation has had any specific effect on nephrologists. It is interesting that intending nephrologists scored lower on the importance they ascribed to hours, working conditions and domestic considerations than did doctors who chose other hospital physician specialties. It may evidence that those doctors who choose nephrology do so in full awareness of its lifestyle demands.
Many early decisions to choose nephrology did not translate into a later career in the specialty. Moreover, female doctors made late decisions about pursuing their career in nephrology. It is important to address the forward and backward mismatch between original choices and career destination in nephrology by focusing on identifiable influencing factors.
Early exposure to renal medicine in medical school and the foundation programme, including increased use of mentors, could highlight its attractive interventional aspects, as well as necessary exposure to patients with chronic kidney disease. 23 Evidence shows that nephrology is perceived as a challenging subject in medical school23,25 and our data highlighted that nephrology is chosen as a specialty because it is what the trainees want (enthusiasm/commitment) which may refer to its intellectual content and clinical activities.
While in a UK setting, there is little scope in the NHS for direct financial incentives favouring one specialty, improvements to working conditions through innovative work scheduling and the promotion of clinical independence at work may confer benefits in increasing commitment.
Strengths and limitations
A strength of this unique large national study of UK doctors is the repeated cohort design, whereby different groups of medical graduates were surveyed in the same ways at different points of time, to follow up their career progression and reveal factors that may affect their choices over time. Furthermore, the high response rate increases confidence in generalising the survey results. 29 However, the findings must be considered in light of some methodological considerations. Given the survey methodology, no inference can be made about causal relationships. The scope of this study is limited to UK medical graduates; thus, international medical graduates, who make a significant contribution to the UK medical workforce, 30 were not considered in this research.
Conclusions
There is a shortfall in the medical workforce provision for renal care from UK medical graduates. There seems to be a decline in interest in nephrology as time passes from graduation, especially among female doctors. Several factors including relevant job experience influenced the decision to pursue nephrology. Late decisions to commit to a career in nephrology were evident in our data, which suggests that doctors with an interest in nephrology could be encouraged earlier in their careers to pursue it. Systematic efforts are required to improve interest in nephrology.
Footnotes
Declarations
Acknowledgements
We thank Ritva Ellison for data management and Janet Justice and Alison Stockford for data entry. We are very grateful to all the doctors who participated in the surveys.
Provenance
Not commissioned; peer-reviewed by Beryl De Souza.