
Abstract
Summary
Objectives
To report on doctors’ reasons, as expressed to our research group, for choosing academic careers and on factors that would make a career in clinical academic medicine more attractive to them.
Design
Postal, email and web questionnaires.
Setting
UK.
Participants
A total of 6936 UK-trained doctors who graduated in 1996, 1999 and 2000.
Main outcome measures
Open-ended comments about a career in clinical academic medicine.
Results
Of doctors who provided reasons for pursuing a long-term career in clinical academic medicine, the main reasons were enjoyment of academic work and personal satisfaction, whether expressed directly in those terms, or in terms of intellectual stimulation, enjoyment of research, teaching and the advancement of medicine, and the job being more varied than and preferable to clinical work alone. Doctors’ suggestions for making clinical academic medicine more attractive included improved pay and job security, better funding of research, greater availability of academic posts, more dedicated time for research (and less service work) and more support and mentoring. Women were more likely than men to prioritise flexible working hours and part-time posts.
Conclusions
Medical schools could provide more information, as part of student teaching, about the opportunities for and realities of a career in clinical academic medicine. Women, in particular, commented that they lacked the role models and information which would encourage them to consider seriously an academic career. Employers could increase academic opportunities by allowing more time for teaching, research and study and should assess whether job plans make adequate allowance for academic work.
Introduction
Positive reasons for doctors to become clinical academics include ‘the challenge of research’ and the ‘intellectual environment’ 1 and ‘variety and intellectual stimulation’. 2 Perceived disincentives include difficulty in obtaining research funding, lower pay than clinical colleagues, lack of job security and reduced clinical training while in academic training.1–3 A systematic literature review of career choice in academic medicine found that reported incentives were completion of research in medical school, a desire to teach or do research and the presence of a role model; reported disincentives included low pay, lack of autonomy and lack of career flexibility. 4 Women, more so than men, are reportedly held back by these disincentives and barriers, and their under-representation in academic medicine is said to impair research agendas, affect patients and waste public investment. 5 Women comprise just 28% of UK clinical academics. 6
The UK Medical Careers Research Group has studied career preferences of junior doctors, and their subsequent career pathways, for many years. In surveys of UK graduates of 1996 in 2007, and graduates of 1999 and 2000 in 2012, we included questions about attitudes to academic careers. Our aims here are to report on the doctors’ views, expressed to us about clinical academic careers, and their views about what changes could be made to clinical academic medicine to make it a more attractive career option.
Methods
Postal and web questionnaires were sent in 2007 to the 1996 cohort and in 2012 to the 1999 and 2000 cohorts. Up to four reminders were sent to non-respondents. Contact details were supplied by the General Medical Council. We omitted deceased doctors, doctors who asked to be excluded and doctors who were uncontactable. Further methodological details are available elsewhere.7,8
We asked the 1996 cohort two open-ended questions: ‘If you have chosen to pursue a long-term career in clinical academic medicine, what are your main reasons for that choice?’ and ‘If you do not intend to work in clinical academic medicine, are there any changes which would have made it more attractive to you as a career option?’ The 1999 and 2000 cohorts were asked to ‘give us any comments you wish to make, on any aspect of your training or work’. We extracted comments which contained any of the following text strings: academi, research, teach, study, education, papers, post-doc, publish, phd, fund, publication, dean, fellowship, doctora, lecturer, lectureship, thesis, MBA, university.
This was a qualitative study. As such, it was not our primary intention to quantify the frequency with which particular views were held about clinical academic careers. Rather, we aimed to identify issues worthy of consideration, even if they were raised by small numbers of individuals.
We developed a coding scheme which reflected the main themes raised. Two researchers coded the themes independently and inter-coder differences were resolved through discussion. Quantitative data were analysed by univariate crosstabulation and χ 2 statistics.
Results
Response
The response rate was 67% (2452/3668) for the 1996 cohort survey in 2007, and 62% (4484/7176) for the 1999 and 2000 surveys in 2012.
Views on doing academic work (1999 and 2000 cohorts)
In all, 1327 respondents (699 from the 1999 cohort, 628 from the 2000 cohort) provided comments. The comments of 339 doctors contained a keyword relating to academic work. Examination of context narrowed the number of doctors making a relevant comment to 124 (9.3% of commenters). This included 30 doctors working as clinical academics or aspiring to do so.

Some doctors gave more than one reason and we counted each reason.
Number of doctors who commented upon academic issues, not the number of commenting doctors (N = 1327).
p < 0.05; Significance tests comparing men and women.
We also include abstracts of the original doctors’ quotations followed by a unique code: the full quotations are in the Appendix. Suffix ‘M’ denotes a man and ‘W’ a woman.
Time for academic work/study leave
The most frequent comment was that there was insufficient time to concentrate on academic work. One aspiring clinical academic wrote of ‘too little flexibility to allow people to develop … academic interests’ (M1). Some contracts only allowed for one Supporting Professional Activity (SPA): ‘I am an employed consultant with only 1 SPA. I am therefore not involved in teaching, audit, research’ (F2). One surgeon complained that ‘1 session per week for combined Research/Admin/Teaching/Study did not allow for the degree of development I had hoped’ (M3). Some found better working conditions abroad: ‘I get time and funding … to … teach, do research and supervise trainee projects’ (F4).
Support/supervision/mentor/advice
Supervisors and mentors were very important. One doctor commented: ‘[I] have benefited from great advice and support from key, senior colleagues’ (M5). Another wrote: ‘it would be great to have a mentor … who can advise me regarding my academic/clinical career’ (F6). One doctor had ‘lacked good advice/mentoring’ (M7).
Work-life balance/women academics
Some described ‘sacrifices’ made in pursuit of an academic career: ‘I love being a doctor but if I knew the personal and family sacrifices … I doubt I would have chosen this profession’ (F8). Many doctors found it difficult to combine academic work with childcare, though some working situations were better than others: ‘An organised rota with protected time as I had at [named hospital] enabled me to make a successful fellowship application. This is in contrast to [named hospital] where the rota was shambolic and consultants unsupportive’ (F9).
Many women described ‘a lack of mentorship for women in academic medicine’ (F10). This was compounded by having a family: ‘ … women are greatly underrepresented in the higher echelons of academia and now that I have my own sights on such positions I wonder how difficult it will be to “break through”’. A pathologist found it ‘difficult working very long hours in general medicine while pregnant. Research funding is very competitive and difficult to get if working part-time’ (F11).
Enjoyment of academic work
Academic work was rewarding and enjoyable for many: ‘I spent 3 years in research and did an international fellowship which I believe greatly helped me’ (M12). Another said ‘I enjoy my work very much and would only consider changing jobs if my funding dried up!’ (M13).
Some enjoyed academic medicine, but not as a career: ‘There have been two reasons that I have ended up taking a consultant job rather than looking to continue down an academic path. Firstly job security. Secondly the scarcity of consultant jobs’ (M14).
Career structure/job security
Some described the clinical academic career path as difficult: ‘[I am] moving towards an academic career but the obstacles are huge compared with [the] NHS route’ (M15).
Some clinical academics were ‘fortunate’ or ‘lucky’ to have gained a certain post: ‘I am lucky that my path as a clinical academic has been (a) supported by a strong research/clinical institution and (b) fortunate with fellowship awards’ (M16). Another found that ‘trying to develop a post-PhD research career while undertaking clinical duties was very challenging’ (M17).
Indecision, a decade post-graduation, remained evident for some: ‘I remain undecided if I want a lifelong academic career or would prefer to be a NHS clinician with an active interest in research’ (M18).
Many doctors mentioned job insecurity. One academic clinical oncologist had ‘educated myself out of employment in the place I would prefer to live’ (F19).
Access to teaching/quality of teaching
Several doctors had ‘poor access to protected teaching whilst working’ (M20). Some felt that the quality of teaching was inadequate: ‘few consultants have a good understanding of good teaching/training practice’ (M21). Another expressed concern for junior doctors taught by ‘senior registrars reaching senior positions having worked fewer hours’ (F22). A radiologist feared having ‘to use (SPA) time to meet (Continuing Professional Development) requirements and may have to give up other roles such as teaching’ (F23).
Academic pressures/targets
Some resented pressure to write academic papers: ‘We went in to this to be clinicians, not to be paper churners’ (M24). Another said: ‘I spent 3 years in postgraduate research which has been completely unhelpful to my career’ (M25).
Working abroad
Several doctors commented about academic opportunities abroad: ‘in the US, academic medicine is strongly encouraged’ (M26). One said that compared with Canada ‘opportunities for research funding in my speciality are very limited in the UK’ (F27). A surgeon working in Australia said that ‘with a healthy interesting job, with the opportunity to teach and direct research, I can offer my family some stability without having to commute around the country’ (M28).
Funding
Some doctors lacked funding for study leave: ‘study leave is capped at £600 a year’ (F29). One doctor was unable ‘to obtain funding for a PhD in medical education despite having done an academic training fellowship, research in education, [and] having a relevant master’s degree’ (M30).
Academic/clinical balance
Doctors in academic work face conflicting demands on their time and expertise in the areas of clinical service work, academic research and teaching. Few mentioned this need for balance as a problem or disincentive to an academic career, but for those who did, it was an important issue.
One doctor felt that the UK system did not promote balance: ‘I feel the UK is very poor in its support for anything other than service delivery development, and pays only lip service to training or academic pursuit’ (M31). Doctors working Less Than Full Time found it particularly hard to do research. One doctor, whose contract was for 50% research said that ‘on paper, I am being given a great opportunity to progress in research and to work less than full time, but in reality, I am being given a heavy burden of clinical duties’ (F32). Incorporating teaching into the mix of responsibilities was mentioned by some: ‘It is now very difficult to find the time to do all the things I would like to such as teach and do research’ (F33).
Pay
Several believed that senior academic opportunities were few in number, and that pay was sometimes low given the amount of responsibility involved: ‘there are very few post-doctoral fellowships that would allow consultant pay-scale and this has forced me to take on a full NHS post without an honorary university contract in order to still have some grounding for my academic pursuits’ (M34). One doctor felt ‘embarrassed [by] how little I earn at my level of training. A career in hospital/academic medicine is just not sustainable as paid so little’ (F35). A few doctors drew comparisons between pay for academic work in the UK compared with abroad: ‘PhD salaries and the balance between work and family life are much better in Denmark than in the UK’ (M36).
Portfolio career
Some doctors had ‘portfolio careers’ which enabled them to do some academic work: ‘the flexibility of this non-training grade has allowed an acceptable work/life balance & also the development of a “portfolio” career involving a large commitment to teaching & medicine writing’ (M37). Another described doing ‘various pieces of work that are all inter-related: academia and clinical, but also writing books, journalism, live performances’ (M38).
Reasons for pursuing a clinical academic medicine career (1996 cohort)
In this earlier survey, undertaken in 2007, reasons were given by 160 respondents who had chosen to pursue an academic career.
Enjoyment and personal satisfaction were the dominant reasons given, whether expressed directly in those terms, or in terms of intellectual stimulation, enjoyment of research, teaching and the advancement of medicine, or simply as the job being more varied and preferable to pure clinical work.
Typical comments were that clinical academia is ‘interesting and creative’ (male, dermatology), and that doing academic work ‘helps to maintain an interest and enthusiasm in your job’ (female, ophthalmology). A male anaesthetist commented that academic work ‘provides stimulation and maintains interest. Opportunity to learn new skills, improve understanding’. Another doctor preferred the ‘challenging mind-broadening environment rather than purely service directed future’ (male, clinical academic). A male microbiologist felt that ‘academic medicine gives you the chance to ask and try to answer interesting clinical questions, not to be in just routine clinical service, with no intellectual stimulation and input’. A female adult psychiatrist wrote that whilst she did ‘enjoy research and teaching…I find clinical psychiatry emotionally draining at times and research/teaching is refreshing and re-energises me for my clinical work’. Further examples of reasons given are shown in Box 1.
Changes which would make clinical academic medicine more attractive (1996 cohort)
Percentage distribution of changes to clinical academic medicine which would have made it a more attractive career option a , by gender – 1996 cohort surveyed in 2007.
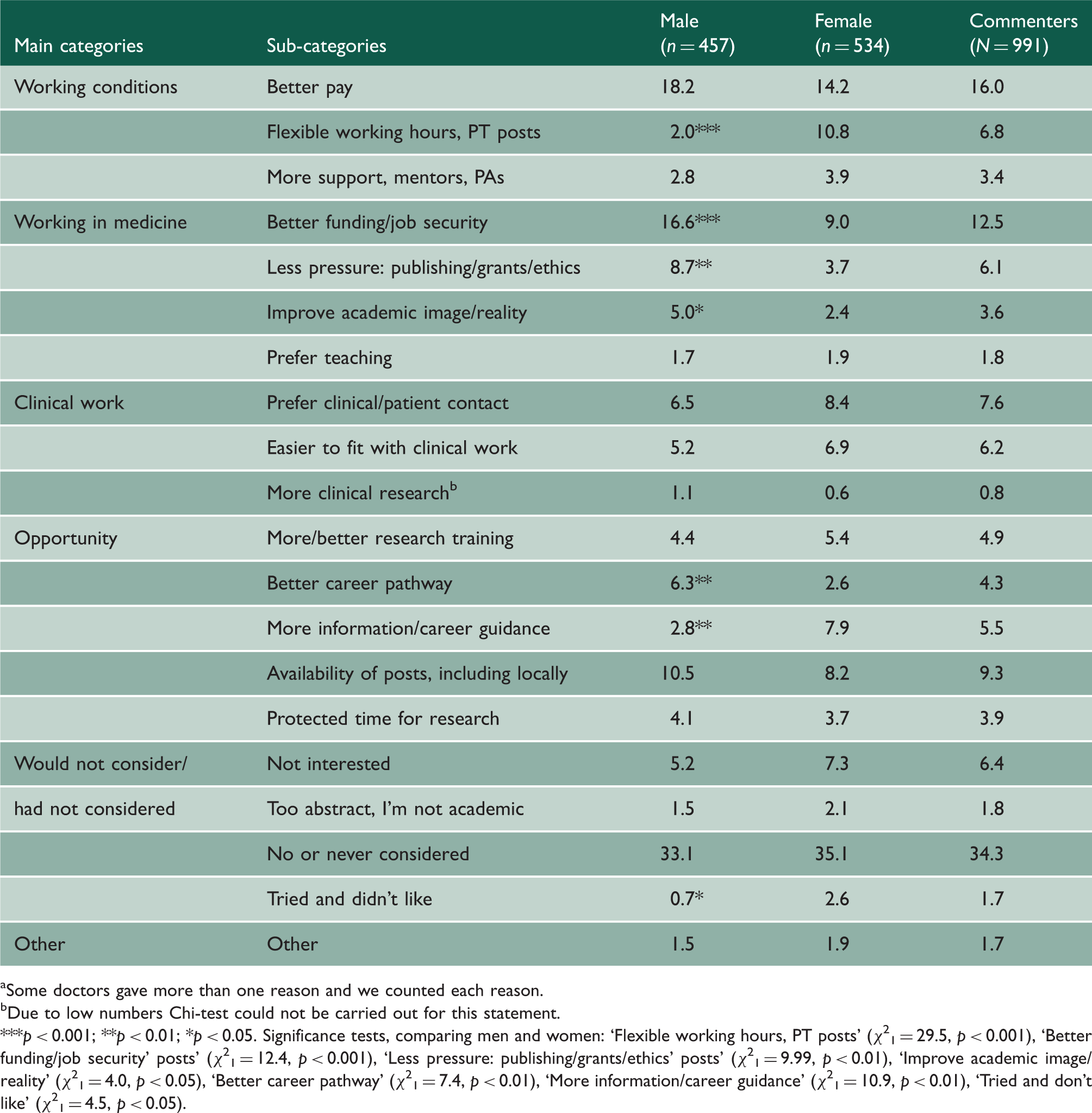
Some doctors gave more than one reason and we counted each reason.
Due to low numbers Chi-test could not be carried out for this statement.
p < 0.001; **p < 0.01; *p < 0.05. Significance tests, comparing men and women: ‘Flexible working hours, PT posts’ (χ21 = 29.5, p < 0.001), ‘Better funding/job security’ posts’ (χ21 = 12.4, p < 0.001), ‘Less pressure: publishing/grants/ethics’ posts’ (χ21 = 9.99, p < 0.01), ‘Improve academic image/reality’ (χ21 = 4.0, p < 0.05), ‘Better career pathway’ (χ21 = 7.4, p < 0.01), ‘More information/career guidance’ (χ21 = 10.9, p < 0.01), ‘Tried and don’t like’ (χ21 = 4.5, p < 0.05).
Examples of reasons for choosing a long-term career in clinical academic medicine, 1996 cohort (numbers of male and female respondents a raising each theme in parentheses).
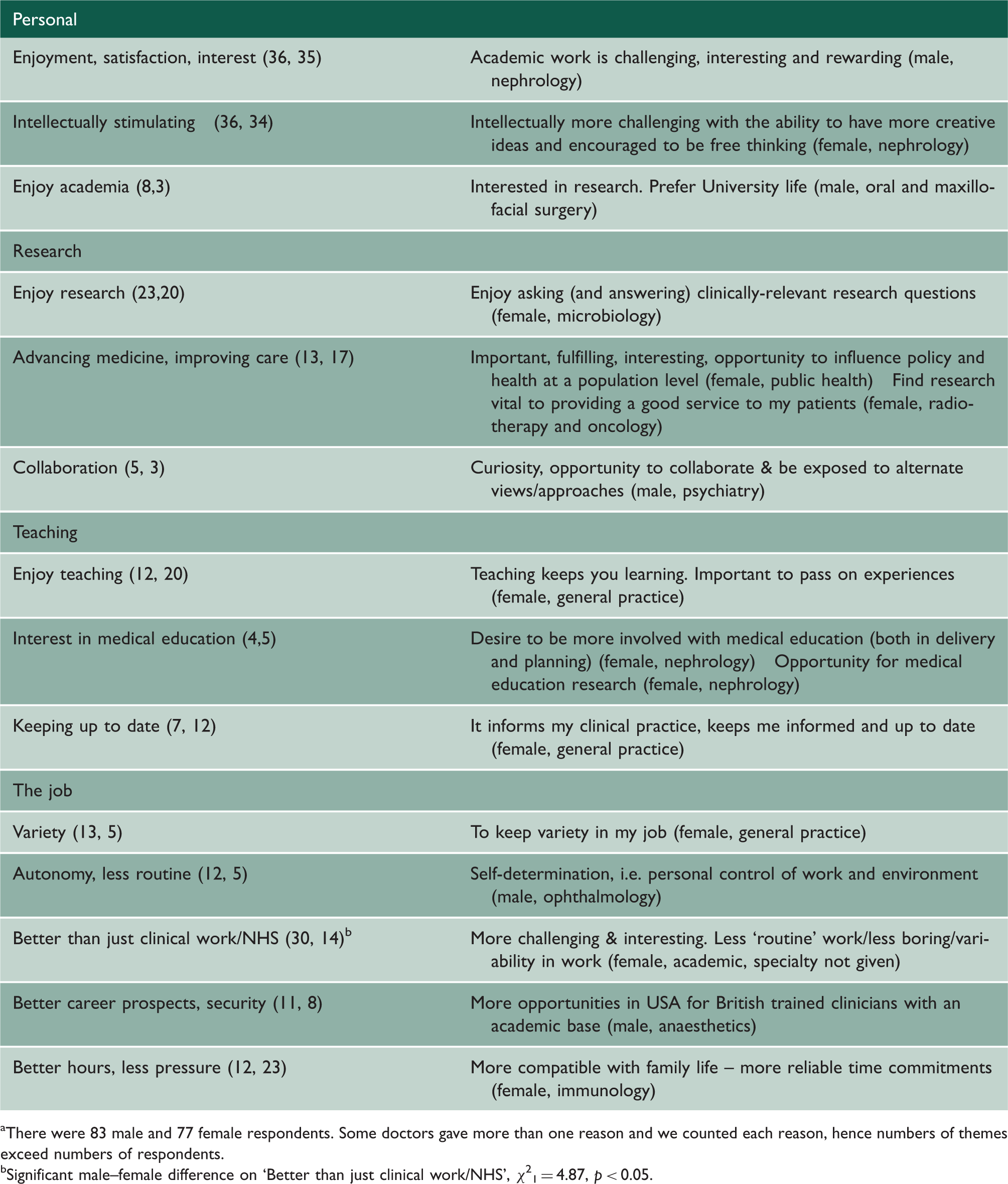
There were 83 male and 77 female respondents. Some doctors gave more than one reason and we counted each reason, hence numbers of themes exceed numbers of respondents.
Significant male–female difference on ‘Better than just clinical work/NHS’, χ21 = 4.87, p < 0.05.
Examples of changes to clinical academic medicine which would make it a more attractive career option, 1996 cohort.

The most frequently suggested improvement to make clinical academia more attractive was ‘better pay’. Many respondents in this 2007 survey said that academic pay should be equal to that for clinical work: ‘most academic posts are poorly paid compared with clinical work’ (female, general practice) was a typical comment.
Other suggested changes included responses we classified as: ‘better funding/job security’, ‘better availability of posts, including locally’, and ‘preference for clinical/patient contact’. More men than women suggested ‘better funding/job security’, ‘less pressure: publishing/grants/ethics’, ‘better career pathway’, and ‘improve academic image/reality’. More women than men suggested ‘flexible working hours, part-time posts’, and ‘more information/career guidance’. More women also said that they had ‘tried and didn’t like’ clinical academic medicine.
Discussion
Main findings
Senior doctors who chose to pursue a long-term career in clinical academic medicine did so because they enjoyed the career, derived satisfaction from it, and found it interesting or intellectually stimulating. Many doctors who had decided not to work in clinical academic medicine had never considered it, or would not consider it, as a career; and preferred clinical work. In our 2007 survey, doctors’ suggestions to make clinical academia more attractive included higher pay, better funding and more job security. In our 2012 survey, pay comparability with non-academic doctors was much less often mentioned; however, doctors mentioned difficulties in finding funding for academic work and a shortage of fellowships, and holding high responsibility in academic work relative to their pay level. There were unfavourable pay comparisons with those in academic work outside the UK. Our 2012 survey found that senior doctors wanted more time for academic work, better supervision, mentoring and careers advice, and the parents in our survey wanted to strike a better work-life balance.
Strengths and weaknesses of the study
Our analysis was national, multi-cohort, recent and was based on the comments of doctors in their own words.
As a qualitative study where only doctors who chose to write relevant comments participated, non-respondent (or non-commenter) bias is possible. The results are not a numerical quantification of views but should be seen as identifying themes, rather than measuring the frequency with which particular views were held.
Comparison with existing literature
Similar reasons for choosing an academic career (enjoyment, satisfaction, interest, intellectual stimulation) were given by doctors in other studies.1,2,4 Two issues raised by our doctors are not apparent in other literature. The first is the perception of ‘pressure’. Some respondents referred negatively to pressure in academia – to obtain research grants, to manage clinical work alongside research work and so on. Others, contrarily, wrote that they felt that academic work could be less pressured than clinical work and could offer time to think and develop. The second issue was a view, expressed by some, that academic work offered a richer and more interesting and fulfilling career option than pure clinical work. Others appeared bored by academic work. Perhaps here we are tapping into personality traits and how different doctors respond to the same situation.
We did not present factors as closed items on a questionnaire, as other studies have.9–11 For example, we did not mention directly the possible influence of role models. In fact, no 1996 graduates cited the influence of a role model in their decision to pursue clinical academic medicine, as found in other studies. 4 However, it seems likely that role models were important to the 1996 graduates who were following academic careers, but the absence of academic role models for many doctors is the real issue. When doctors talked freely about their training and employment (our 2012 survey), many doctors raised the importance of good supervision, support and mentoring.
Many improvements to academic careers suggested by our respondents were also found in other studies, 4 although the desire for more posts in the doctor’s local area is new. In a recent paper on doctors’ mobility, we reported a trend towards reduced mobility among doctors as they pursued their careers. 12
Women wanted more flexible working hours, more part-time posts, more information and better career guidance. More part-time provision would benefit women, men and employers, by promoting work-life balance, staff contentment and staff retention. 13 The Medical Schools Council’s ‘Women in Clinical Academia Working Group’ surveyed senior clinical academics, most of whom graduated in the 1970s and found that they benefited from strong links with senior role models, but that women medical students were unable to identify such figures in their lives. 14 These third and fourth year students were studied in 2006: during their earlier years in medical school only 1 in 10 medical clinical professors were women, and six UK medical schools had no female professors. 15 Other studies support the benefits of a mentor-mentee relationship for female academic doctors.16,17
Implications
Many doctors do not consider a career in clinical academia. It is important to raise awareness amongst medical students. Women need more information about clinical academic careers, and senior women clinical academics should be more involved in providing advice. Trainers should provide more time and support to doctors to undertake academic work. Local training programmes may benefit by considering these issues.