
Abstract
Objective
There is scarcity of reliable information on stroke in Lebanon. We aim to determine the potential risk factors for stroke in the Lebanese population.
Design
A retrospective case-control study was conducted between January 1st, 2012 and December 31st, 2014 at two different tertiary hospitals in Lebanon. Data were collected through a designed data collection sheet. A multiple logistic regression determined stroke risk factors. The strength of association between the dependent variable and independent variables was expressed in odds ratio (OR) through 95% confidence interval.
Setting
Lebanon
Participants
Lebanese hospitalized patients.
Main outcome measures
Stroke risk factors
Results
Overall, 202 stroke cases and 530 stroke-free controls were included. The mean age of stroke was 68 ± 13 years. Age, smoking and a history of hypertension, cardiac arrhythmia, coronary heart disease/myocardial infarction, deep venous thrombosis/pulmonary embolism, and migraine were significantly associated with high risk of stroke. Grade 3 blood pressure had the highest OR (44.112; 95% CI, 16.144–120.528).
Conclusions
The results of this study confirm the significant contribution of certain well-identified risk factors with stroke. Modifying, treating and controlling major stroke risk factors though medications or lifestyle change would result in having a second change in the Lebanese population. Therefore, we recommend implementing preventive strategies on those pathologies to reduce the risk of total stroke in Lebanon.
Introduction
Stroke, or cerebrovascular accident, is a common cause of morbidity and mortality worldwide. In 2013 alone, there were 10.3 million new strokes, 6.5 million stroke deaths, 25.7 million stroke survivors and 113 million disability-adjusted life years due to stroke. 1 Developing countries had the greatest share of global stroke burden and death compared to developing countries, comprising 75.2% of stroke mortality and 81.0% of stroke-related disability-adjusted life years. 1
Lebanon is a developing country in the Middle East. The provision of health service by governmental hospitals has declined during the last few decades mainly due to managerial and medical issues, where only half of the 24 public hospitals were left operational with an average of 20 active beds per hospital. On the other hand, private hospitals have developed in both quality and quantity and today they represent about 90% of the total hospital beds in the country. The majority are owned by physicians and localised in Beirut and surrounding Mount Lebanon. 2
There is a scarcity of reliable information on stroke in Lebanon. The adjusted stroke prevalence in Lebanon was 0.50% (95% confidence interval, 0.33–0.66) in 2012, and the rate of stroke mortality reached 62.7/100,000 population in 2011.3,4 Despite having stroke intervention rate in Lebanon higher than other reported rates in developing countries (administration rate of recombinant tissue plasminogen activator is 10.3% for stroke cases at the largest tertiary care center in Lebanon), this intervention is still very limited due to large time interval between arrival at the hospital and computed tomography completion (average time 49.4 min) and therefore large time interval between arrival and IV recombinant tissue plasminogen activator (average time interval 102.4 min). 5
Risk factors for cerebrovascular accident are now well established, and validated tools, which predict risk of stroke, are included in clinical guidelines. However, even with respect to those well-established stroke risk factors, significant ambiguity persists about the strength of their association with stroke risk due to substantial differences between populations, including genes, cultural factors, environmental risk factors and ethnicity. We aimed to conduct a hospital-based case–control study to determine the potential risk factors for stroke in the Lebanese population.
Methods
Study design
A retrospective, hospital-based, case–control study was conducted on all stroke patients over 18 years old admitted to two Lebanese tertiary hospitals located in the capital Beirut (one private and another governmental) between 1 January 2012 and 31 December 2014. The Ethics committee of the Lebanese University has approved this study and waived the need for informed consent from the patients whose data were used in this study since it was observational with no traceability for patients. The basic ethical principles were respected including respect for persons, beneficence and justice. 6
Study sample size
No study has been published in Lebanon concerning stroke risk factors and the strength of association between stroke and well-known risk factors. Therefore, sample size was calculated with an α risk of 5%, a β risk of 20%, a ratio of controls to cases of 2:1 and a minimal exposure probability of 36.9%, representing the prevalence of hypertension among Lebanese people older than 21 years. 7 The minimal sample size necessary in order to show a 2.98 increase in the risk of stroke among hypertensive people, according to the INTERSTROKE study, is 123 subjects with 41 cases and 82 controls based on Epi info. 8 In regard to smoking, the prevalence of cigarette smoking in Lebanon among those aged 15 years or more is 30.7%. 9 The sample size required to detect a 1.67 increase in the risk of stroke among cigarette smokers, according to the INTERSTROKE study, is 566 subjects with 189 cases and 377 controls. 8 However, we considered all stroke patients admitted to the two interested hospitals within the study period and we increased the number of controls in order to improve the statistical power of the study.
Development of data collection sheet
The data collection sheet was based on different publications’ findings, written in English language and included four parts. The first part included patients’ socio-demographic characteristics, diagnosis, imaging techniques and medications. The second part included patients’ symptoms on admission. The third part addressed all potential risk factors of stroke. The fourth part was related to patients’ laboratory data upon admission to hospitals.
Data collection and definition of stroke and certain diagnostic categories
All variables were collected retrospectively based on information present in patients’ files. Evidence of medical history was based on the laboratory tests results stated, the presence of a reported disease history or treatment history and the definition of certain diagnostic categories, including stroke and transient ischemic attack, hypertension and blood pressure grades, diabetes, dyslipidemia and overweight and obesity.10–14
Inclusion and exclusion criteria
Hospitalised stroke patients were included if they were 18 years or older and diagnosed with stroke by computed tomography or magnetic resonance imaging. Stroke patients were excluded if clinical information was unavailable or computed tomography scan or magnetic resonance imaging were not performed.
Control patients were included if they were 18 years or older and admitted to the same hospitals as stroke patients but with disorders or procedures unrelated to stroke or transient ischemic attack. Controls were chosen from the departments related to infectious diseases, cancer, endocrinology diseases, respiratory diseases, kidney diseases and digestive diseases as well as orthopaedic surgeries.
Statistical methods
Data were analysed using SPSS version 21; p value <0.05 determined statistical significance. Continuous variables were presented as means with standard deviation and categorical variables as percentages. The differences in baseline characteristics between stroke patients and stroke-free patients were analysed using chi-square test for qualitative variables and sample t-test for quantitative variables. Fisher’s exact test was used when the expected cell size was less than five.
A stepwise ascending logistic regression was conducted. The strength of association between the dependent variable (presence of stroke or not) and independent variables was expressed in odds ratio through 95% confidence interval. The independent variables’ list included the potential risk factors such as medication history, history of certain diagnosis, smoking history, family history of stroke and heart attack and the different categories of blood pressures.
Results
Summary of primary results
Two hundred and fifty stroke cases were admitted to the interesting hospitals between 1 January 2012 and 31 December 2014. Among those, 48 stroke cases were not diagnosed with stroke by computed tomography scan or magnetic resonance imaging and therefore were excluded. Overall, 732 patients were included in the present study with 202 cases diagnosed with stroke and 530 stroke-free controls. The mean age of stroke was 68 ± 13 years. Males constituted 53.5% of stroke patients. Among stroke patients, 25.7% had transient ischaemic stroke (transient ischaemic attack), 59.4% had ischaemic stroke and 14.9% had haemorrhagic stroke. The in-hospital stroke mortality rate was 7.4%, with haemorrhagic rate higher than ischaemic rate, 20% versus 7.5%, respectively.
Due to missing data in regard to patients’ addresses (43.7% of the sample), this sample mainly represented Lebanese patients living in Beirut (46.6% of patients with available address in their hospital file) and Mount Lebanon (44.2%). Only 4.6% of patients with available address lived in Beqaa, 3.6% live in North Lebanon and 1% live in South Lebanon.
Characteristics of stroke patients in the private and governmental hospitals.
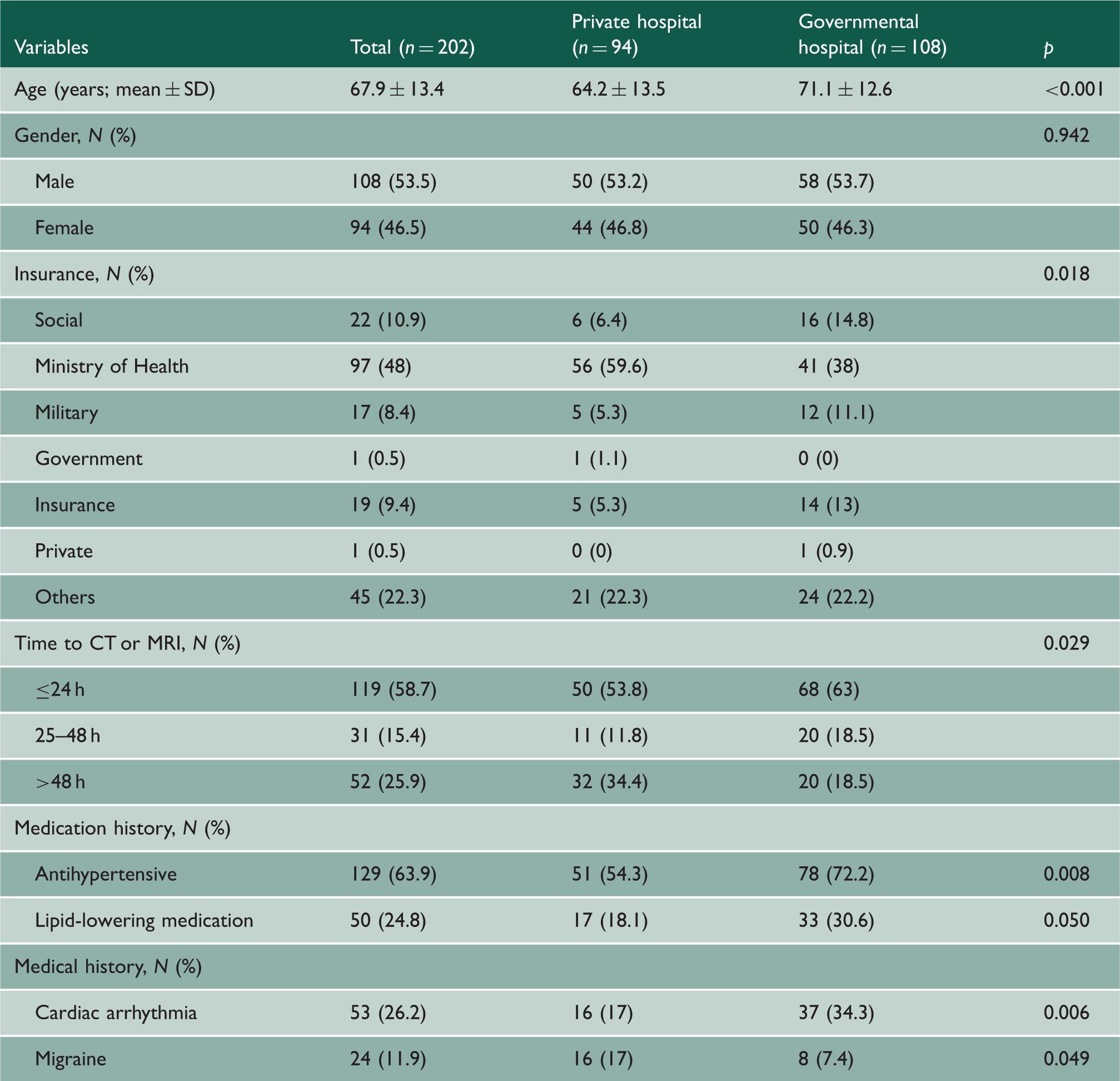
CT: computed tomography; MRI: magnetic resonance imaging; SD: standard deviation.
Characteristics of the study sample.

SD: standard deviation; TIA/CVA: transient ischaemic attack/cerebrovascular accident.
Factors predicting stroke risk in the Lebanese population (−2 log likelihood, 417.511 and Nagelkerke R Square, 0.651).

BP: blood pressure; CI: confidence interval; OR: odds ratio; *statistically significant (p < 0.05).
Subjects were stratified on the basis of age range and sex. The incidence of ischaemic stroke and haemorrhagic stroke was more common after the age of 65 years. Most of the ischaemic stroke incidences occurred in the age range of 65–69 years and 70–74 years, 20.0% and 16.7%, respectively, while most of the haemorrhagic stroke incidences occurred in the age range of 70–74 years and 75–79 years, 16.7% and 20.0%, respectively. In stratification by sex, males predominated females in number of ischaemic stroke, but in haemorrhagic stroke, we had 50% of males and 50% of females.
Factors predicting ischaemic and haemorrhagic stroke risk in the Lebanese population.

BP: blood pressure; CI: confidence interval; ORa: adjusted odds ratio; *statistically significant.
Discussion
In this study, we were able to confirm that age, smoking and the presence of a history of hypertension, cardiac arrhythmia, coronary heart disease/myocardial infarction, deep venous thrombosis/pulmonary embolism and migraine are associated with increased odds ratio of a risk of total stroke among the Lebanese population.
Similar to many high-income and Middle East countries, the mean age of our stroke patients was within the sixth and the seventh decades; male patients constituted the majority of our stroke patients, and ischaemic stroke was the most reported type of stroke.15,16
Hypertension is a common disease considered as an important risk factor leading to stroke. In a cross-sectional survey conducted in Lebanon with people older than 21 years, the crude prevalence of hypertension was 36.9% with about three quarters of Lebanese aged 65 years and older having hypertension. 7 In this study, a total of 43.7% of included patients (72.3% of cases and 32.8% of controls) were hypertensive. Only 63.9% of stroke cases were under antihypertensive treatment compared to 43.6% of controls who were taking antihypertensive medication for hypertension treatment or prevention. These results highlighted the necessity of conducting a prospective study in order to assess patients’ adherence to antihypertensive medication and whether this is related to decreasing stroke risk in Lebanon. However, our study suggests that the risk of stroke is seven times higher among hypertensive patients than those with normal blood pressure, which is in agreement with the results of other studies.17,18 The strength of the association between hypertension and cerebrovascular accident in Lebanon is stronger compared to what was reported by the INTERSTROKE study (odds ratio 2.98), 7 Qatar (odds ratio 2.73), 19 Pakistan (odds ratio 4.16) 20 and the Netherlands (relative risk 1.6). 21
Our findings confirm the significant association between cardiac arrhythmia and coronary heart disease/myocardial infarction and stroke which is in concurrence with other studies.20,22 Our results also suggest a six-fold increase in the risk of stroke in patients with migraine, similarly to what was suggested by other studies.23,24 Moreover, this study demonstrates a significant association between smoking and stroke risk, confirming the results of numerous studies performed across different ethnicities and populations. 25
The relative role of risk factors in ischaemic or haemorrhagic stroke remains inconsistent. In one study, a risk factor might favour one stroke type; in another, it might favour another stroke type and in another, it might not favour either of the stroke subtypes. 26
In the multivariate analysis, an increased age was associated with ischaemic stroke but not with haemorrhagic stroke. This is in accordance with a population-based observational study to predict ischaemic stroke, but not with the hospital-based Copenhagen Stroke Study and Danish National Indicator Project where age did not predict any type of stroke. 26
Being a female was associated with the risk of haemorrhagic stroke in our study; however, this might be due to older age at the incidence of stroke and longer life expectancy among women. Nevertheless, sex did not herald stroke type in many studies including the Danish National Indicator Project. 26
Hypertension is a well-documented risk factor for both types of strokes. Hypertension was only associated with the risk of ischaemic stroke in this study but not of haemorrhagic stroke when we separated our stroke cases based on types of strokes, which is in occurrence with the population-based case-controlled Perth study. 27 However, it is unclear whether the presence of hypertension is a favour of either of the stroke subtypes especially given that many studies showed different results where hypertension did not favour either of the stroke subtypes, or was associated to ischaemic stroke alone or haemorrhagic stroke versus ischaemic stroke. 27 Moreover, we can assume that we did not find hypertension to be associated with the risk of haemorrhagic stroke in our population due to a limited number of haemorrhagic cases included. Antihypertensive treatment was found to reduce the risk of both stroke subtypes, ischaemic stroke and haemorrhagic stroke, confirming the 40-year results of clinical trials.28,29
Cigarette smoking favoured ischaemic stroke alone and not haemorrhagic stroke, which contradicts the findings of many studies including the Hemorrhagic Stroke Project and the Danish National Indicator Project, but confirms the findings of a systematic review of 14 case–control studies and 11 cohort studies as well as the Atherosclerosis Risk in Communities Study.26,30–32
Cardiac arrhythmia/atrial fibrillation and coronary heart disease/myocardial infarction were also found to be associated with the risk of both stroke subtypes in our study. The Danish National Indicator Project only found them to be associated with ischaemic stroke rather than haemorrhagic stroke. 26 Anticoagulant treatment has also been associated with a decreased risk of ischaemic stroke in our population, which is also confirmed by a meta-analysis of six randomised trials. 33
Migraine was found to be a predictor of ischaemic stroke. A systematic review and meta-analysis of 14 observational studies confirmed the fact that migraine is a risk factor for ischaemic stroke. 23 Other studies reported a relationship with ischaemic stroke based on migraine type.24,34
Modifying, treating and controlling major stroke risk factors through medications or lifestyle change would result in having a second change in the Lebanese population in particular and in the Middle East in general especially when someone knows his/her score risk.
The strength of our study is the limitation of the common types of potential biases in case–control studies. To reduce the selection bias, control patients were selected from the same hospitals as case patients; community-based controls were unfeasible. To minimise observer’s bias, a standardised collection sheet was used to collect data and a protocol was developed for collecting, measuring and interpreting information.
There are, however, numerous potential limitations in our study. This study has been conducted retrospectively and patients’ files were missing for certain data, which might have limited certain data value and affected the results including specific diets, alcohol consumption and physical activity. Moreover, the large odds ratios and the wide 95% confidence intervals found in the multivariate analysis of certain risk factors with haemorrhagic stroke indicate that we have a limited number of cases to fit the analysis we are conducting and that more information is needed to be precise in the magnitude of the effect of certain risk factors. A larger and prospective study would be of interest to address the issue of the association between stroke and other well-defined risk factors, which did not reach statistical significance in our study.
In conclusion, the results of this study confirm the significant contribution of age, cigarette smoking, hypertension, coronary heart disease/myocardial infarction, deep venous thrombosis/pulmonary embolism and migraine to increase the prediction of total stroke risk in the Lebanese population. Therefore, we recommend implementing preventive strategies on those pathologies to reduce the risk of total stroke.
Footnotes
Declarations
Acknowledgements
We would like to thank the Rectorate of the Lebanese University, Beirut-Lebanon, to support this work.
Provenance
Not commissioned; peer-reviewed by Osama Amin.