
Abstract
Objectives
To determine an association between unemployment rates and human immunodeficiency virus (HIV) mortality in the Organisation for Economic Co-operation and Development (OECD).
Design
Multivariate regression analysis.
Participants
OECD member states.
Setting
OECD.
Main outcome measures
World Health Organization HIV mortality.
Results
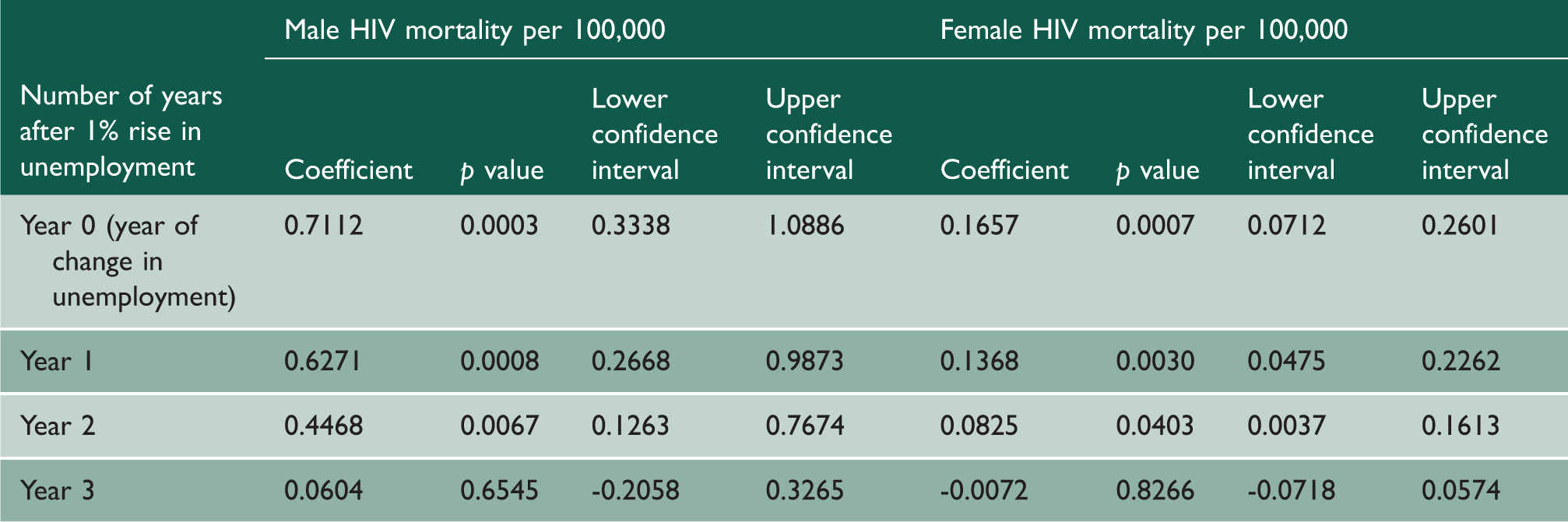
Between 1981 and 2009, a 1% increase in unemployment was associated with an increase in HIV mortality in the OECD (coefficient for men 0.711, 0.334–1.089, p = 0.0003; coefficient for women 0.166, 0.071–0.260, p = 0.0007). Time lag analysis showed a significant increase in HIV mortality for up to two years after rises in unemployment: p = 0.0008 for men and p = 0.0030 for women in year 1, p = 0.0067 for men and p = 0.0403 for women in year 2.
Conclusions
Rises in unemployment are associated with increased HIV mortality. Economic fiscal policy may impact upon population health. Policy discussions should take into consideration potential health outcomes.
Introduction
The world is facing one of the most severe global recessions in modern history, with rising unemployment levels across a range of countries. 1 There are concerns regarding the adverse effect of the prolonged economic recession on population health outcomes. 2
Unemployment in the OECD, 2006 and 2009.
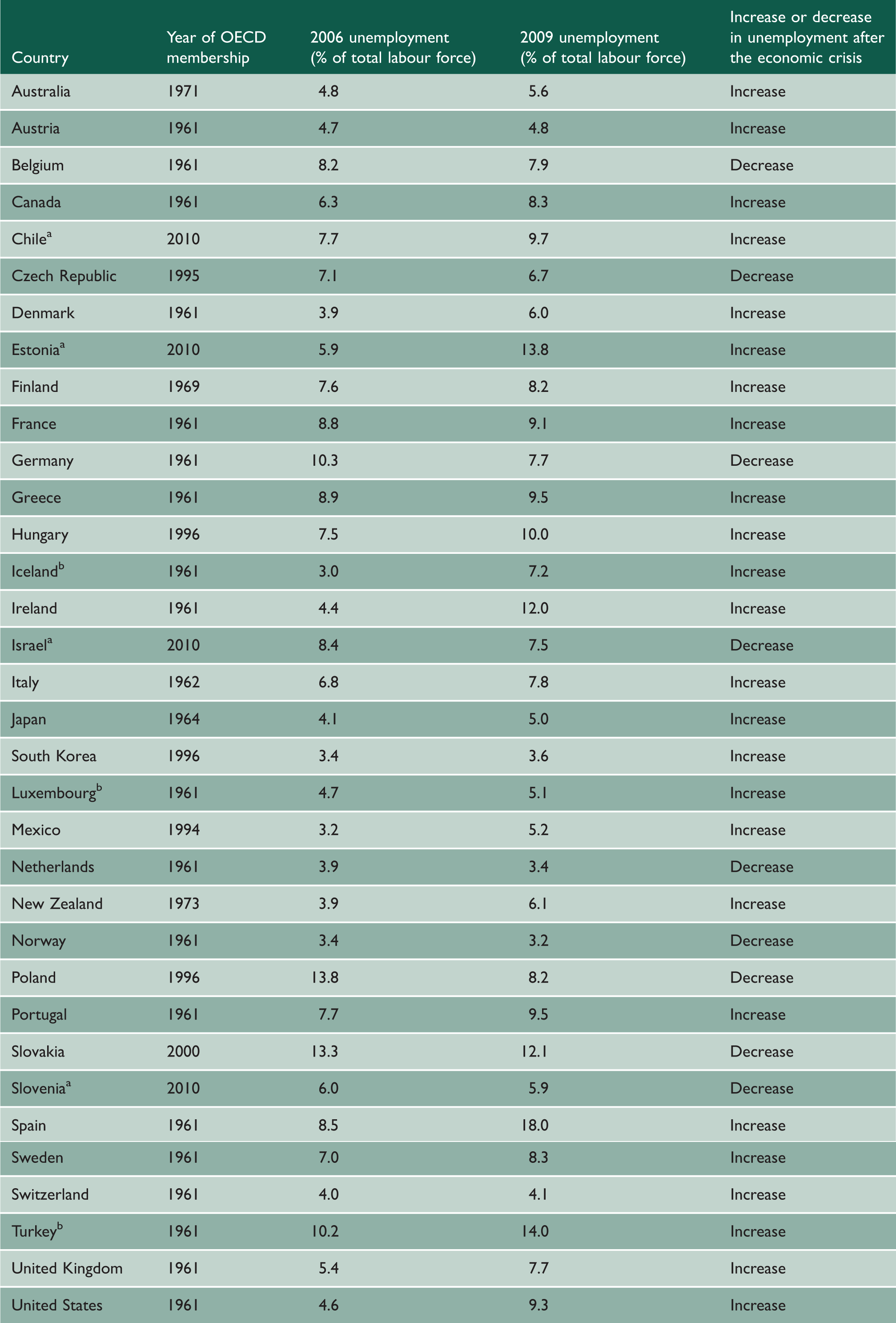
OECD: Organisation for Economic Co-operation and Development.
aChile, Estonia, Israel and Slovenia were excluded from our analysis as they joined the OECD in 2010 (outside the scope of our study).
bIceland, Luxembourg and Turkey were excluded from our analysis due to insufficient HIV mortality data.
Studies exploring impact of economic downturns on population outcomes have shown that periods of economic hardship are associated with increased mortality and worsening health outcomes.6–8 More recent national studies have confirmed these ‘adverse effects',9–11 demonstrating associations between unemployment and all-cause mortality, suicide rates and road traffic accidents. In contrast, detailed analyses of the relationship between unemployment and specific pathologies have, by and large, been neglected.
A small number of studies have investigated the effect of financial downturns on HIV-infected individuals in single country settings,12,13 concluding that unemployment is an independent risk factor for disease progression and mortality. However, population-wide correlations at the national or multinational level, in addition to long-term trends, have yet to be determined.
We sought to build on earlier studies to determine the effect of changes in unemployment on HIV mortality across the OECD between 1981 and 2009, hypothesising that rising unemployment rates are associated with increased HIV mortality. The substantial increases in unemployment in recent years as well as the availability of high-quality epidemiological and socioeconomic data within the OECD provide a clear opportunity to assess any association.
Methods
Data collection
Data were analysed for 27 of the 34 current OECD member states. Chile, Estonia, Israel and Slovenia were excluded from our analysis as they joined the OECD in 2010, outside the scope of our study. Iceland, Luxembourg and Turkey were excluded from our analysis due to insufficient HIV mortality data (Table 4 in Appendix).
HIV mortality data by sex was obtained from the World Health Organization’s (WHO) mortality database, 14 which is updated annually from civil registration systems of member states. Only medically certified deaths attributed to HIV are recorded in this dataset. The quality of this data has been evaluated by the WHO. 15 Reported national death statistics were assessed by completeness, coverage and quality. Completeness was defined as the proportion of all deaths that are registered in the population covered by the vital registration system for a country. Of the 27 countries included in our analysis, 26 had achieved 100% completeness. The Republic of Korea had 89% completeness. Coverage is calculated by dividing the total number of deaths reported from vital registration system for a country-year by the total number of deaths estimated by the WHO for that year for the national population. Twenty-one countries included in our analysis had 100% coverage. Greece (88%), Italy (99%), Japan (97%), Republic of Korea (88%), Mexico (96%) and Norway (98%) were assessed to have suboptimal coverage. No adjustments have been made to the raw data to account for under-coverage. Quality was determined by taking into account the revision of the International statistical classification of diseases, and related health problems were used for national vital registration statistics, the completeness of data and minimal use of ill-defined categories of death. Of the 27 national datasets used in our analysis, 11 were considered to be of high quality, 13 of medium quality and 3 of low quality. We used age standardised death rates (ASDR) per 100,000 as the basis of our analysis. The ASDR, as defined by the WHO, is the weighted average of age-specific mortality rate per 100,000, where the weights are proportional to the number of individuals in the corresponding age groups of the WHO standard population. 15 We chose to use ASDR as it controls for differences in age distribution within populations by accounting for age-specific mortality rates. 16 Socioeconomic data were obtained from the World Bank’s Development Indicators Database 2013. 17 Unemployment was taken to be the proportion of the labour force without work but available and seeking employment, as defined by the World Bank. 17
Statistical analysis
Multivariate regression analysis was used to assess the relationship between HIV mortality (dependent variable) and unemployment (independent variable). To ensure that results were not driven by extreme observations for certain countries, a fixed-effects approach was used in our regression models, including 26 dummy variables for the 27 countries in the dataset. Doing this meant that the model evaluated mortality changes within individual countries while holding constant time-invariant differences between countries including higher predispositions to HIV, as well as political, cultural and structural differences. This conservative modelling approach made the data more comparable. The demographic structure of the selected countries was also controlled for by incorporating total population size, in addition to the percentage of the population aged over 65 years and less than 15 years into the model. Economic factors were controlled for by incorporating inflation, changes in GDP (gross domestic product) per capita and interest rates into the model. Healthcare resources were controlled for by incorporating the number of hospital beds per 1000 and number of physicians per 100,000. Both out-of-pocket health expenditure and health expenditure per capita (measured in purchasing power parity) were also controlled for. And finally, developmental indicators were controlled for by incorporating the prevalence of urbanisation, the mean calorific intake of the population as well as accessibility to clean water.
We used the Cook–Weisberg test 18 to assess for and to confirm heteroskedasticity (where sub-samples have different distributions) in the data used. Therefore, robust standard errors were included in the regression models; this allowed us to account for heterogeneity in unemployment data due to differences in the way that countries measured unemployment rates, along with factors such as underemployment or social programmes (for example, back-to-work initiatives or programmes that see individuals move from employment to education or training) that may otherwise have hidden or suppressed actual unemployment rates.
This methodology has been widely used in similar health-economic studies and is regarded as a statistically robust approach.8,19–22
The ordinary-least-squares linear regression model was as follows:

We conducted one-, two- and three-year time-lag multivariate analyses to quantify the long-term effects of changes in unemployment on HIV mortality. Several robustness checks were also conducted; these are detailed in the Results section.
Stata SE version 12 was used for the analysis (Stata Corporation, Texas, USA). The “regress” command was used for our analysis.
Results
Multiple regression and lag analysis.
The data show the impact of a hypothetical 1% rise in unemployment on HIV mortality, controlling for proportion of population up to age of 14, proportion of population over age of 65, population size, 30 country controls, inflation, changes in GDP per capita, interest rates, urbanisation, nutrition (mean calorie intake), access to water, number of hospital beds per 1,000, number of physicians per 100,000, out of pocket expenses, health spending per capita (measured in purchasing power parity).
A 1% rise in unemployment was found to be associated with a statistically significant rise in HIV mortality per 100,000 in both men and women (coefficient for men 0.7112, 95% CI: 0.3338–1.0886, p = 0.0003; coefficient for women 0.1657, CI: 0.0712–0.2601, p = 0.0007). According to the most recent UN estimates,
23
the combined population of the OECD countries is estimated to exceed 1.24 billion individuals. Based on this, a hypothetical 1% rise in unemployment across the OECD would be associated with 4327 male and 1050 female additional HIV deaths, during the year of the unemployment rise, not taking into consideration any lagged or longer term effects of unemployment. Time lag analysis showed that each given 1% rise in unemployment was associated with increased HIV mortality for up to two years after the initial unemployment change (Table 2, Figure 1). For year 1, coefficient for men is 0.6271, CI: 0.2668–0.9873, p = 0.0008; coefficient for women is 0.1368, CI: 0.0475–0.2262, p = 0.0030. In year 2, coefficient for men is 0.4468, CI: 0.1263–0.7674, p = 0.0067; coefficient for women is 0.0825, CI: 0.0037–0.1613, p = 0.0403. In year 3, changes were non-significant.
A 1% rise in unemployment is associated with statistically significant lagged increases in HIV mortality for two years, in both men and women.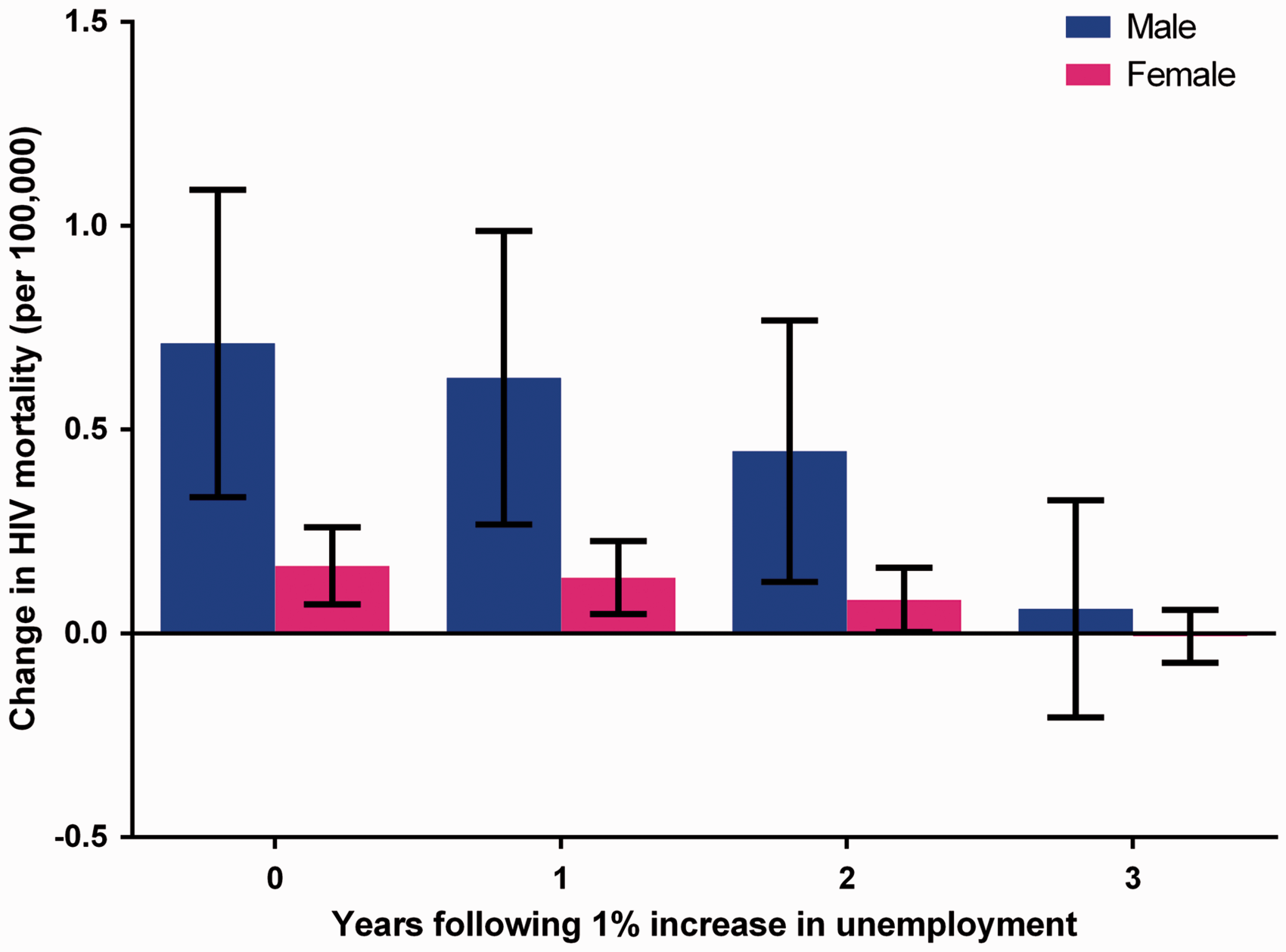
Robustness checks
Robustness checks.

Multiple regression analyses were re-run using the controls in the original analysis in addition to those mentioned in the table below. The data show the impact of a 1% rise in unemployment, on HIV mortality, using the mentioned controls.
Discussion
Findings
This study has shown that increased unemployment in the OECD countries is associated with an increase in HIV mortality. These effects become apparent in the immediate time frame but also persist in the medium term. The scale of this association is such that a hypothetical 1% rise in unemployment in the OECD would be associated with an excess HIV mortality, in the order of thousands. Importantly, this statistically significant finding persisted even after accounting for a variety of potential confounding factors.
Our results show that the increase in HIV mortality, associated with rising unemployment, disproportionately affects males in comparison to females. This difference is reflected in the WHO’s reported HIV mortality figures. 14 The underlying explanation for this difference is likely to be a complex interplay between various biological, behavioural and social factors. Furthermore, the increased risk of suicide and all-cause mortality during unemployment tends to be greater in men.27–29 This observed difference may partially be the result of men being more reluctant to seek healthcare services and therefore presenting at later stages of disease progression. 30
Potential mechanisms
The mechanism by which unemployment might drive HIV mortality is currently unclear. We hypothesise that a number of mechanisms may potentially link the two variables. First, unemployment might negatively impact upon the socioeconomic status of HIV-infected individuals. The influence of social background on health outcomes has been extensively documented in the published literature. 31 Studies have shown that there is a strong association between low socioeconomic status and increased risk of HIV mortality.32–35 Some propose that this is the result of delayed diagnosis and treatment due to reduced healthcare access. 32 Others have demonstrated that a statistical association remains even after adjustment for such factors, suggesting that low socioeconomic status may be an independent factor for HIV mortality. 34
Similarly, previous regional studies have shown that unemployment itself is also associated with delayed access to treatment. 35 It has been shown that even after accounting for this, unemployment remains an independent risk factor for HIV morbidity and mortality. 13 Our study shows that this association, at least with regard to HIV mortality, holds true on a much more macroscopic level, across the OECD.
The link between unemployment and an elevated incidence of suicide has also been well established.7,8,10 Underpinning these observations are the detrimental effects that unemployment has on psychological health and wellbeing. It is possible that this psychological effect and its associated behavioural changes may also contribute to increased mortality in HIV patients.
Exclusion of out of pocket expenditure from our analysis reduced the magnitude of association between unemployment and HIV mortality, suggesting that reduced out of pocket expenditure during times of unemployment may not contribute towards increased HIV mortality in year 0 (Table 2).
Strengths and limitations
Our quantitative macroeconomic approach confers several methodological strengths. We considered a much larger range of countries than previous studies, enabling investigation of international trends. Notably, our study used a conservative, fixed-effects regression analysis model. Modelling rates as normally distributed above and below the predicted value, which is essentially done by linear regression, is an unusual approach (rates cannot be negative, for example, yet this method permits and indeed expects negative rates). However, with large datasets, it can be justified if the model fits the data sufficiently: We believe that our analysis meets both of these criteria. This model together with the implemented robustness checks, and inclusion of 13 potential confounders and 26 country-specific dummy variables, account for many of the criticisms levelled at other studies looking at the relationship between health outcomes and unemployment, namely, the omission of potential confounding variables that are likely to be correlated with both unemployment rates and HIV mortality rates. In using a panel data approach to compare unemployment rates at interval of one year, for each year after the increase in unemployment with the mortality rates in each country, we also controlled for time-invariant heterogeneity between countries; something that aggregate, time-series analyses fail to do. The potential influence of bias was also minimised from this study by only using data taken from high-quality, objective, centralised databases. The quality of the mortality data has been evaluated by the WHO. 15 However, the dataset makes no attempt to correct suboptimal national civil registration coverage. Despite this, across the whole OECD dataset, a high degree of total coverage is achieved. In addition, mortality in HIV persons where cause of death was not attributed to HIV would have been omitted from our analysis.
However, the broad overview of this study is also a source of weakness. Since we only evaluated annual data compiled at the national level, any variations or discrepancies that might have been present, in smaller geographical regions or across shorter timeframes, would not have been captured. Indeed, it has been shown that substantial variation in unemployment occurs at the subnational and regional levels and this can influence health outcomes. 36 Second, the endpoints of our analysis focused solely on measures of mortality. We did not consider the effects of changes in unemployment on other HIV health measures, which could have yielded different results. Third, we were unable to stratify unemployment distribution by socioeconomic class. As discussed above, socioeconomic status is thought to contribute to HIV mortality. As a result, this study fails to dissect the influence of this potential confounding factor. Fourth, while this study does show an association between unemployment and HIV mortality, a causal link cannot be established. It is possible that rises in HIV mortality could result in a rise in unemployment; a phenomenon known as endogeneity. Indeed, there is substantial historical precedent of employment discrimination against HIV-infected individuals. However, the impact of HIV infection status on employability is extremely variable depending on geo-social factors. 37 The likelihood of endogeneity confounding our findings is unlikely, since implausibly large increases in HIV prevalence would probably be required in order to affect unemployment rates in such a short timeframe. Additionally, our lag analysis which demonstrates a long-term influence of unemployment on HIV mortality would not be consistent with such a phenomenon. Finally, our study analyses ecological data and so is prone to ecological fallacy – we cannot infer conclusions about individual doctors or patients from country-level data.
Implications
Our findings could have important implications both for healthcare professionals and to policy makers. Previous studies have shown that unemployment can exacerbate the perceived barriers to healthcare access. 38 This is directly reflected by reduced healthcare utilisation by unemployed individuals compared to their employed counterparts. 39 Our study provides further support to the importance of clinician awareness of the potentially increased vulnerability of unemployed patients. Steps to facilitate healthcare access and ensure the rapid delivery both of diagnosis and treatments could address such vulnerabilities. What strategies would be most suitable in tackling such an issue is unclear. The evidence supporting the efficacy of different interventions with the aim of addressing health inequalities due to social determinants has been largely inconclusive. 40
At the macro level, the influence of economic policy on public health cannot be overlooked. Fiscal policies that increase unemployment rates should only be exercised with due consideration, not only because of their social and economic repercussions but also since they may also act to adversely affect population health, specifically in this case, HIV mortality. Indeed, current austerity measures could contribute towards exacerbating the burden of infectious diseases, including HIV.41 Policies promoting return-to-work such as work-sharing programmes or those that prevent further unemployment could potentially benefit HIV survival. 1
Conclusions
The recent global recessions led to a rapid increase in unemployment across almost all OECD member states, and the economies of many countries have yet to recover. This event has raised the question of how unemployment may impact HIV outcomes at the population level. Our study has shown that increases in aggregate unemployment are associated with significantly higher HIV mortality in the OECD. Policy interventions and austerity measures, which may increase unemployment, are a key concern, possibly presenting additional barriers to HIV management.
Footnotes
Declarations
Acknowledgements
None
Provenance
Not commissioned; peer-reviewed by Simon Howard