
Abstract
Objective
There has been significant concern that austerity measures have negatively impacted health in the UK. We examined whether budgetary reductions in Pension Credit and social care have been associated with recent rises in mortality rates among pensioners aged 85 years and over.
Design
Cross-local authority longitudinal study.
Setting
Three hundred and twenty-four lower tier local authorities in England.
Main outcome measure
Annual percentage changes in mortality rates among pensioners aged 85 years or over.
Results
Between 2007 and 2013, each 1% decline in Pension Credit spending (support for low income pensioners) per beneficiary was associated with an increase in 0.68% in old-age mortality (95% CI: 0.41 to 0.95). Each reduction in the number of beneficiaries per 1000 pensioners was associated with an increase in 0.20% (95% CI: 0.15 to 0.24). Each 1% decline in social care spending was associated with a significant rise in old-age mortality (0.08%, 95% CI: 0.0006–0.12) but not after adjusting for Pension Credit spending. Similar patterns were seen in both men and women. Weaker associations observed for those aged 75 to 84 years, and none among those 65 to 74 years. Categories of service expenditure not expected to affect old-age mortality, such as transportation, showed no association.
Conclusions
Rising mortality rates among pensioners aged 85 years and over were linked to reductions in spending on income support for poor pensioners and social care. Findings suggest austerity measures in England have affected vulnerable old-age adults.
Introduction
The long-term decline in mortality among those aged 85 years and over in England has reversed, since 2010 among men and 2011 among women (Figure 1).
1
By 2013, rates for men were 4% higher than in 2010, while among women they were 6.1% higher. This was not seen in other older age groups, though the long-term decline among those aged 75 to 84 years recently plateaued. Among those aged 65 to 74 years, and those just under pension age, mortality rates continued to decline.
Decline and rise in mortality rates among pensioners by age in England before and after 2011. Source: Office for National Statistics.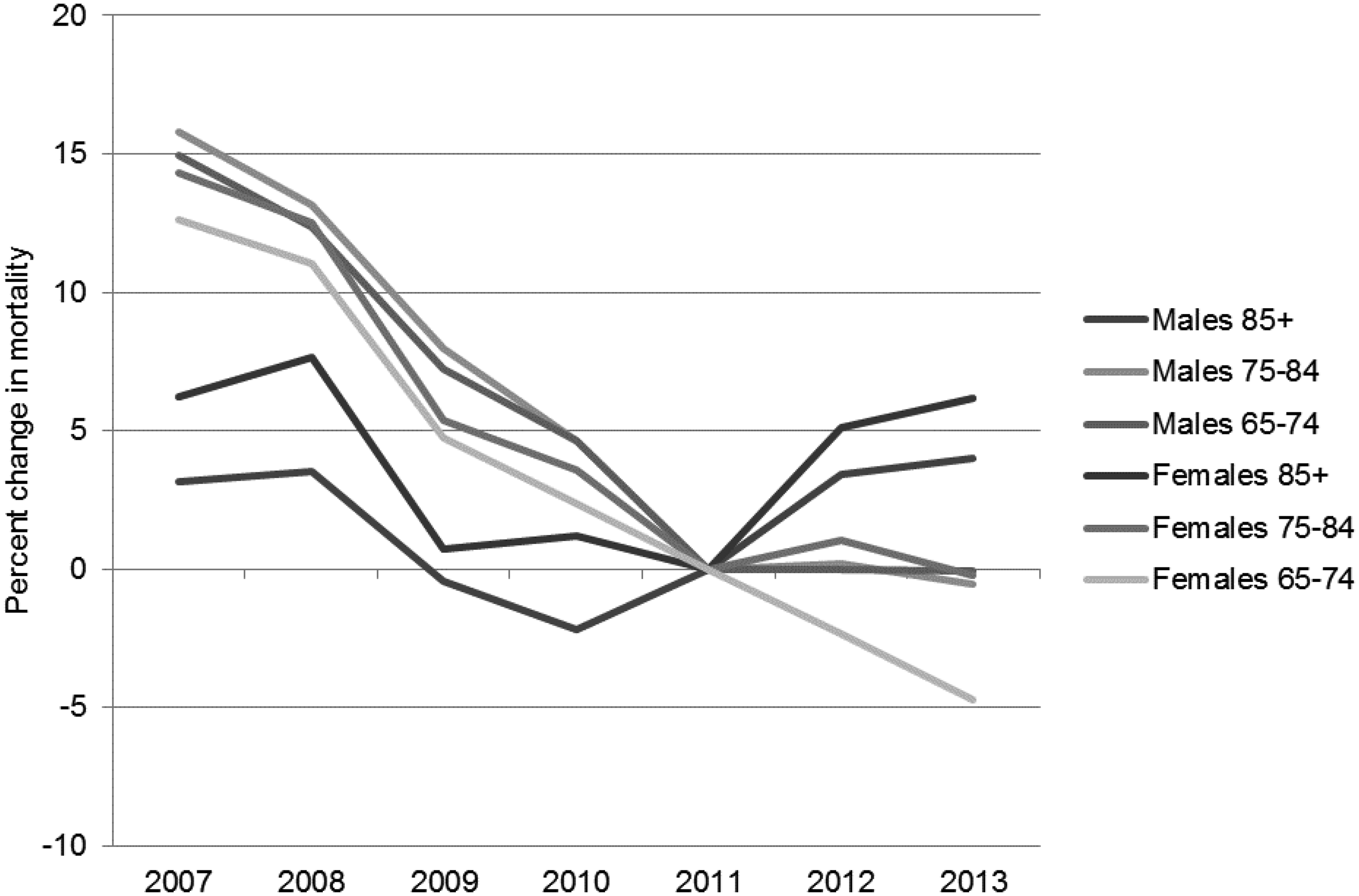
These unexplained increases have occurred in the context of a large-scale experiment with austerity measures in the UK. With a stated aim to reduce the deficit, the Coalition government sought cuts totalling £85 billion. 2 It reduced per capita spending on local services by 23.4% and made structural reforms to welfare administration and the generosity and conditions attached to receipt of benefits. In total, these changes resulted in a net reduction in welfare expenditure of £16.7 billion, about 7% less than would be expected prior to these reforms. 3 The coincidence of rising mortality and budget cuts has led several commentators to speculate that there might be a causal relationship.
Healthcare professionals are in the front line when it comes to dealing with the health consequences of some of these policies. A survey published in the BMJ in 2013 found that, among over 1000 GPs surveyed, 68% indicated that they had seen evidence of their patients’ health being affected by reductions to their benefits, and 94% said their workload had increased to some degree due to increasing financial hardship among their patients. 4 Rising claims for homelessness assistance have been linked to reduced spending on housing services and welfare support. 5 Food bank use has been highest in areas facing largest cuts to benefit spending and where most claimants have had their benefit payments stopped for failing to meet certain conditions. 6 Fit-for-work tests have coincided with rising suicides, prescriptions for anti-depressants and declining mental health. 7 In turn, there have been calls for medical professionals to be involved in assessing whether welfare benefits were adequate to ensure the health of their patients and to act as advocates where they see need emerging.8,9
In this context of austerity, alongside rising old-age mortality, there have been concerns among clinicians and public health practitioners that the welfare system is losing its ability to provide adequate support and care for older persons. Public Health England examined mortality at ages over 65 years and considered three possible explanations – statistical artefact, influenza and cold weather – concluding that the increase was linked to a prolonged flu season and especially cold winter in 2012. 1 The report did not consider reductions in government expenditure, but the possibility of these links was raised in a recent New Statesman article, asking ‘Why are the old dying before their time?’ 10 Citing recent data from the Office of National Statistics showing declining life expectancies, it raised concerns that reduced social care for the elderly and other community services for the elderly may explain these trends. These concerns were shared by Caroline Abrahams from Age UK, who stated ‘the most obvious likely culprit is the rapid decline of state-funded social care in recent years, which is leaving hundreds of thousands of older people to struggle on alone at home without any help’. 11
If Public Health England’s attribution of rising mortality to cold weather and flu is correct, then it should lead to an elevation of mortality in regional swathes across the nation. However, as noted in their report,
1
and as shown in more detail in Figure 2, trends have varied considerably across local authorities, with no apparent geographic patterning consistent with regional outbreaks. About one-quarter of local authorities actually experienced a decline in old-age mortality deaths over 2011 to 2012, while another quarter experienced especially large rises of 9%.
Change in mortality rates among pensioners aged over 85 years across local authorities in England, 2011 to 2012.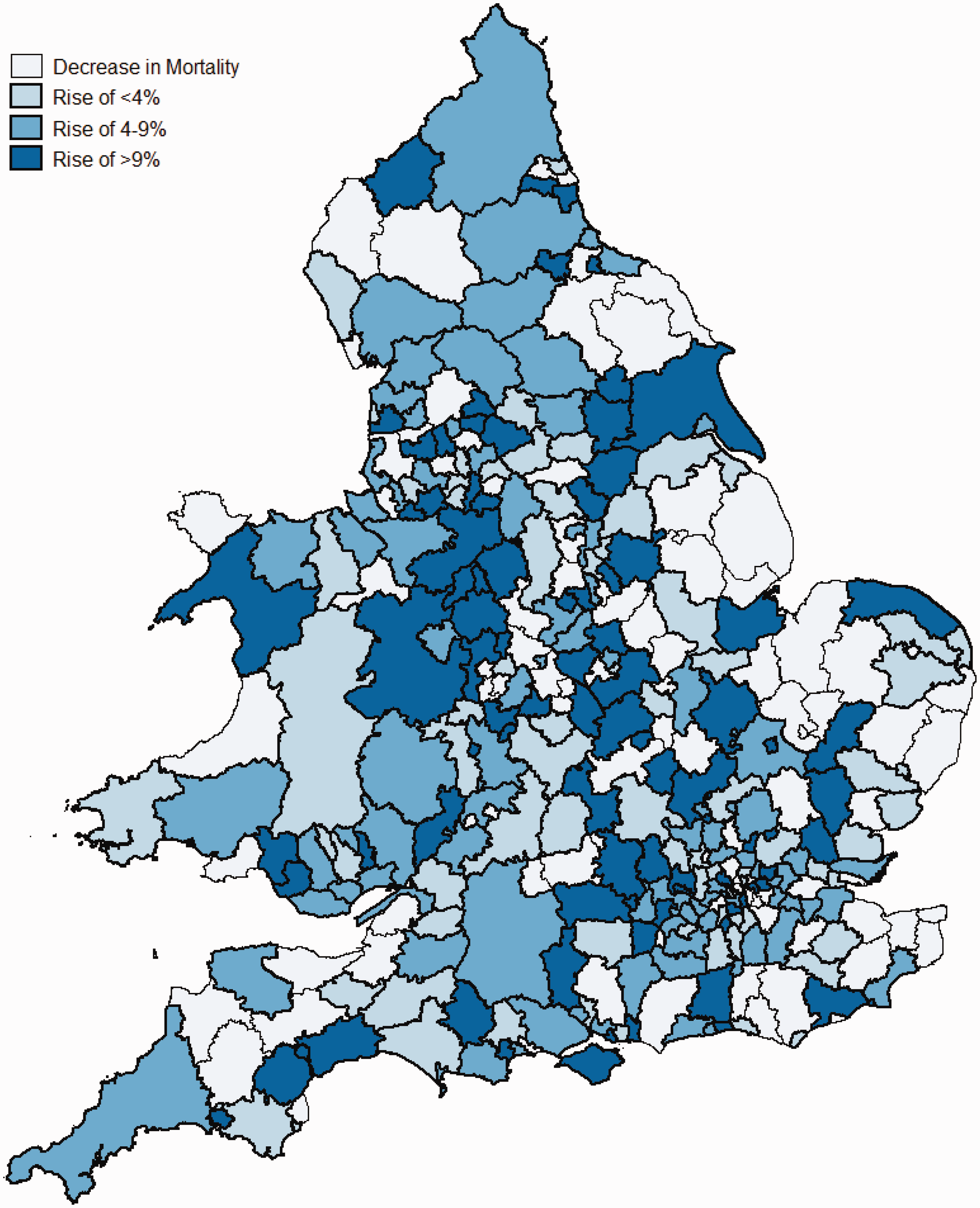
Here, we test the hypothesis that reductions in spending on the various forms of social and economic support which benefit older people could impact on mortality rates. Although the basic state pension has been protected from public spending cuts, with a ‘Triple lock’ increasing it by the highest figure of inflation, average earnings or 2.5%, unlike other welfare benefits, there have been substantial cuts in two major areas particularly affecting older people. First, the Coalition government reduced Pension Credits, which provide financial support to pensioners on low incomes. This has two components, Guarantee Credit, which guarantees that all pensioners receive a weekly income of £151.20 (single) or £230.85, somewhat higher than the basic state pension, and Savings Credit, which gives those with small amounts of savings additional cash payments. Both also give recipients entitlement to a range of other benefits, such as reduced Council Tax. In 2011, the government froze weekly Savings Credit payments, and in 2012, increased eligibility thresholds leading to a significant reduction in claimants and a reduction in payments (Web Appendix Table A1). As shown in Figure 3, average spending on Pension Credit dropped from £759 per pensioner in 2011 to less than £675 per pensioner in 2012.
Spending on Pension Credit and social care across 324 local authorities in England, 2007 to 2013. Notes: Spending adjusted for inflation using GDP deflator.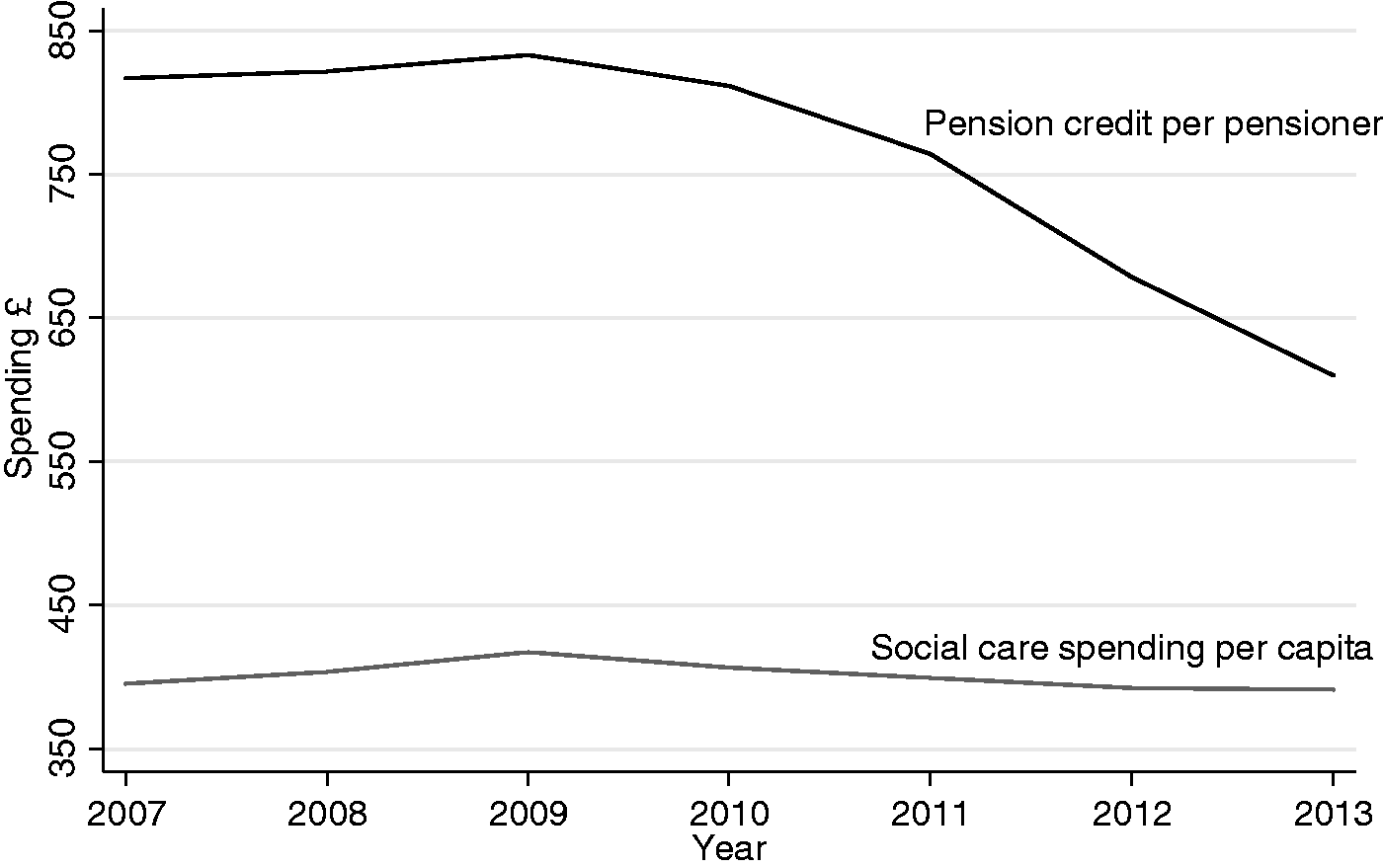
Second, local authorities have reduced spending on social care to achieve budget deficit targets. This includes reduced funding for residential care, day and domiciliary care, and assessment and care management for elderly people. The Institute for Fiscal Studies has calculated that while spending on health increased by 4.3% in real terms during 2010–2011 and 2014–2015, spending on social care fell by 11.5%. 12 Social care spending on older people has been especially hard hit; spending on people aged 65 years and over made up only 51% of total adult social care spending in 2013–2014, down from 56% in 2009–2010. 13
Using data from 324 local authorities in England spanning 2007–2013, we test the hypothesis that budgetary reductions in spending on Pension Credit and social care and reductions in the number of Pension Credit beneficiaries are associated with increasing mortality observed among pensioners aged 85 years and over.
Methods
Data
We collected data on age-specific mortality from the Office for National Statistics for 324 lower-tier local authorities in England (excluding City of London and Isles of Scilly due to small population size), which were available for years covering 2007 to 2013. 14 We used annual population estimates to calculate mortality rates for all persons aged 85 years and over per 1000 population. These data were matched to local authority data on welfare expenditure, including social care from the Department of Communities and Local Government, and on state pensions and Pension Credit from the Department for Work and Pensions.15,16 Because upper tier councils control spending on social care and some other services, these expenditures were allocated to lower-tier districts by their population weightings within the overall council. All spending data are in constant pounds per capita. We obtained data on the number of Pension Credit beneficiaries from Nomis. 17 The count for every quarter was averaged over fiscal years and divided by the number of pensioners in local authorities to obtain the annual prevalence of Pension Credit beneficiaries.
Statistical model
We used a multiple linear regression model to assess the association of changes in mortality rates with changes in welfare provisioning for older-age adults. Specifically, we used a first difference model, examining how the annual change prevalence of Pension Credit beneficiaries, amount spent on Pension Credit per beneficiary, and the amount of spending per capita on social care in local authorities related to the annual percentage change in mortality for pensioners aged over 85 years, as follows:
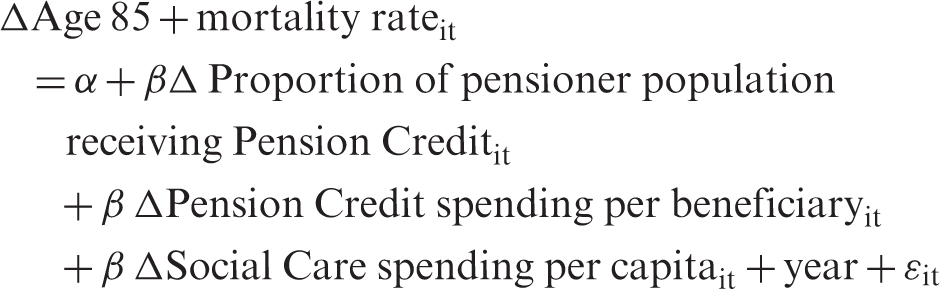
Here i is local authority and t is year. Spending data were converted into annual percent changes per capita. This approach controls for between-area differences by only examining the associations between changes in spending and benefit coverage in relation to changes in mortality within each local authority. Thereby, fixed characteristics influencing differences in mortality rates between areas are unlikely to confound our analysis. To correct for pre-existing time trends, we included an adjustment for the linear time-trend.
These analyses were conducted for total mortality rates and for men and women separately. Though we hypothesised that, given their vulnerability, it would be the oldest groups that would be most affected by cuts in spending, we also examined these relationships using changes in mortality rates among pensioners aged 65 to 74 years and 75 to 84 years to test the specificity of our findings. We removed outliers from local authorities where annual percentage changes in mortality and spending were >|20%| and those in which standardised residuals exceeded two standard deviations because of instability due to small numbers in some authorities, although the results were not qualitatively affected by this step. All models were computed using STATAv13.0 with robust standard errors adjusted for clustering effects of local authorities.
Results
Relationship between annual changes in welfare spending and coverage and mortality among pensioners aged 85+ years, 324 local authorities in England, 1843 local authority-years, 2007 to 2013.
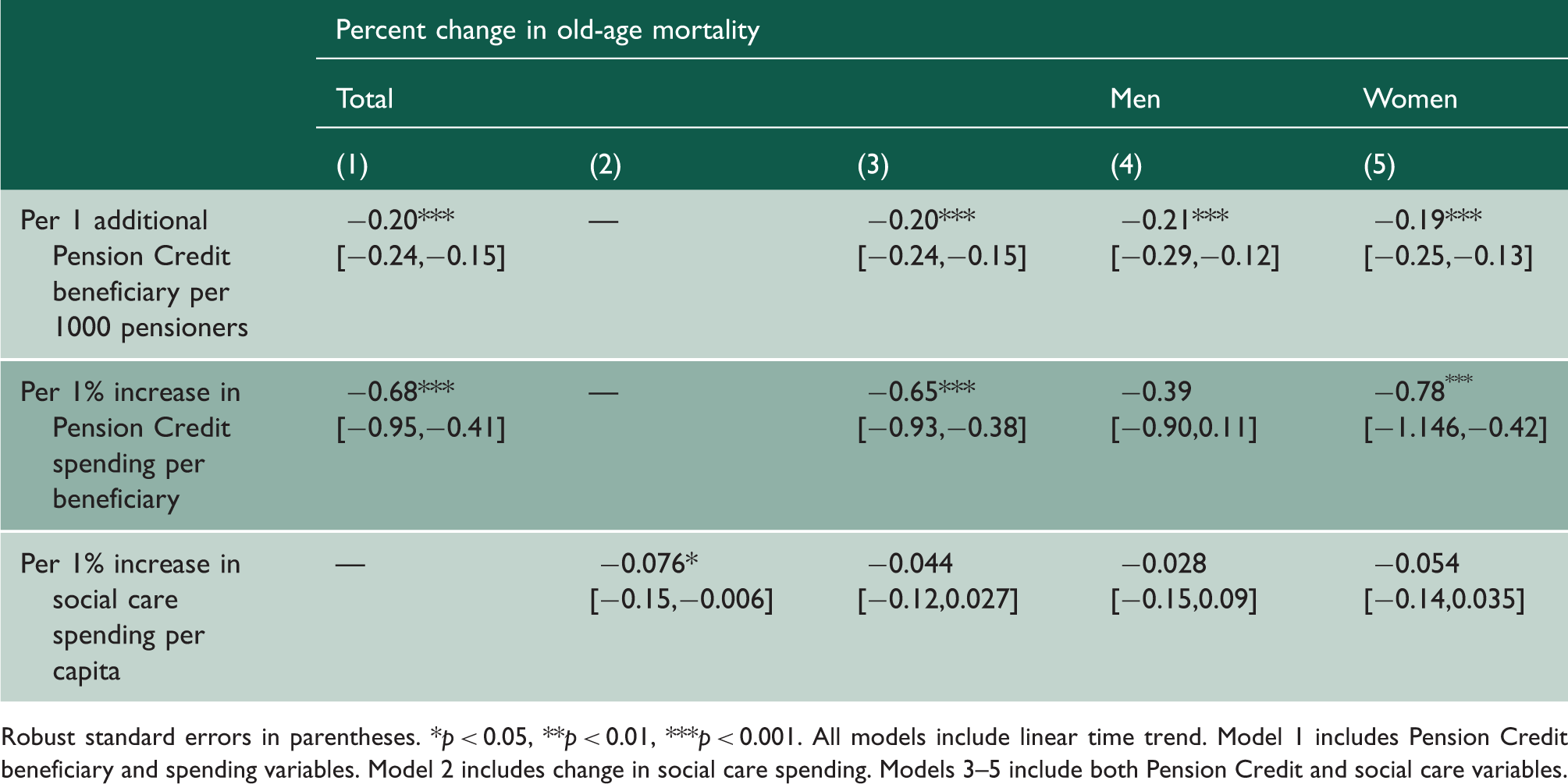
Robust standard errors in parentheses. *p < 0.05, **p < 0.01, ***p < 0.001. All models include linear time trend. Model 1 includes Pension Credit beneficiary and spending variables. Model 2 includes change in social care spending. Models 3–5 include both Pension Credit and social care variables.
We also found that greater reductions in social care per capita were associated with a significant rise in old-age mortality (0.08%, 95% CI: 0.006–0.015%, but, as shown in Table 1, this association was attenuated to non-significance after adjusting for changes in Pension Credit beneficiaries and expenditure (0.04; 95% CI: −0.03 to 0.12).
Relationship between annual changes in welfare spending and coverage and mortality among pensioners by age, 324 local authorities in England, 1843 local authority-years, 2007 to 2013.
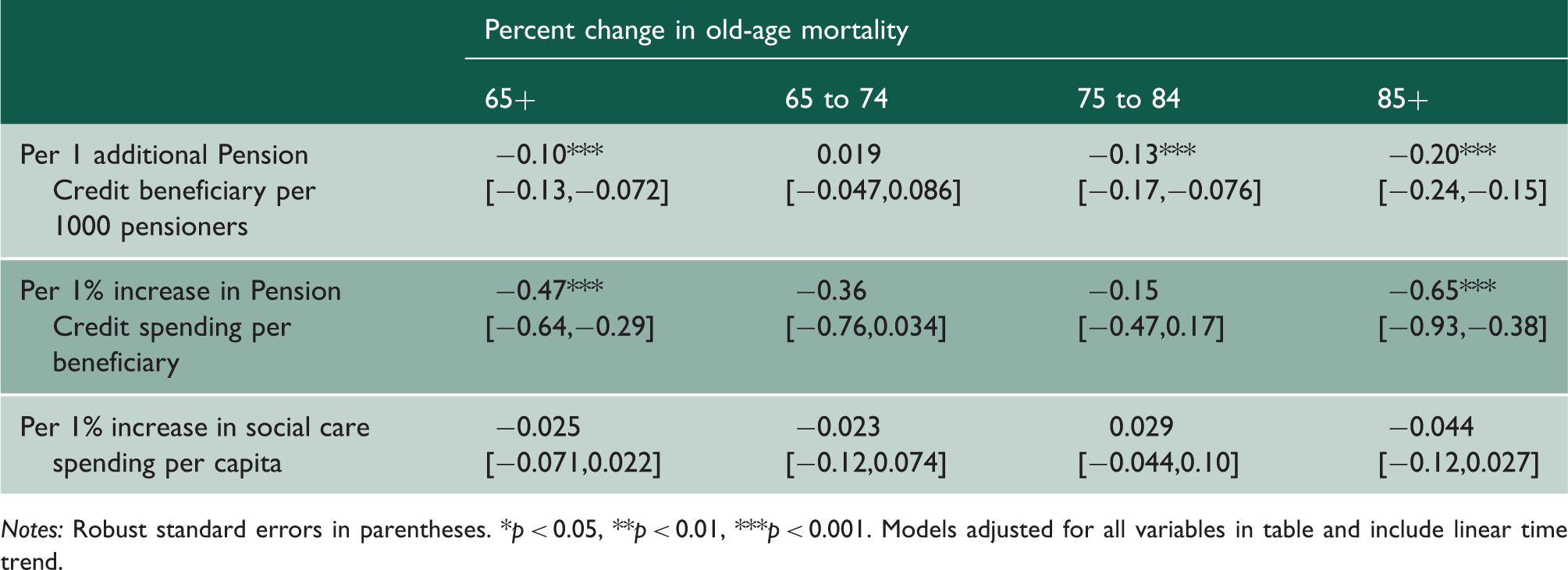
Notes: Robust standard errors in parentheses. *p < 0.05, **p < 0.01, ***p < 0.001. Models adjusted for all variables in table and include linear time trend.
Robustness checks
We performed a series of robustness and specificity checks. First, we incorporated additional data from Nomis that specified beneficiaries of the Savings Credit and Guarantee Credit portions of Pension Credit coverage separately, and provided information on average weekly spending per beneficiary. Consistent with the changes that were made to Savings Credit in 2011 and 2012, we observed that annual reductions in spending and coverage in the Savings Credit portion of Pension Credit were more strongly associated with increasing old-age mortality (Web Table A3). Second, we examined different categories of local authority spending, including total spending, transportation, central services and cultural and recreational services, to check the specificity of our findings. None was significantly associated with old-age mortality rates (Web Table A4). Next, we adjusted for the level of state pension spending, which was not reduced during this period. Our main findings were unchanged; consistent with the observation that Pension Credits were protective, we found that each 1% increase in spending on state pensions was associated with a significant decrease in old-age mortality of 0.55% (95% CI: 0.26–0.85%) (Web Table A4, model 6).
Discussion
Principal findings
Our results suggest that budgetary reductions to incomes of the poorest pensioners may have increased their vulnerability and risk of mortality. There was a strong association of reductions in spending on Pension Credit and reductions in Pension Credit coverage with rising age-85+ mortality rates.
Strengths and weaknesses
To our knowledge, this study is the first to link data on welfare spending to old-age mortality rates in the UK for recent years, in a period when death rates have risen. Using cross-local authority variation, we were able to identify associations with different categories of welfare spending. Falsification tests showed a high degree of specificity in our findings. For example, it was the Savings Credit portion of Pension Credit, which underwent changes in both eligibility and generosity that was most strongly associated with increasing mortality among those in the oldest age group. We also observed an association with social care spending, but did not find associations with other areas of spending that would not be expected to have an impact on old-age mortality, but which underwent cuts between 2011 and 2013. Furthermore, we would expect that cuts to spending would impact the oldest, most vulnerable pensioner groups, and indeed, observed no, or only weak, associations with younger pensioner groups.
The statistical analysis has several limitations, however. First, we could not investigate relationships between changes in receipt of welfare and social care and risk of mortality at the individual level as such data were not available to test this research question. Thus, our analysis is ecological and could be vulnerable to ecological fallacy. Second, ideally this study would examine what conditions those over 85 years are dying from to identify the mechanisms involved. However, cause of death coding is notoriously unreliable at these ages. Those who reach the age of 85 years often have multiple disorders, any one of which could be identified as the cause of death. 18 Moreover, there may be geographical clustering related to custom and practice in attribution of deaths at these ages to particular causes. Nonetheless, many of the common causes of death in older people in England are associated with risk factors such as cold and impaired nutrition, with another form of income supplementation in older people, winter fuel payments, linked to about half of the decline in excess winter mortality observed in England during the 1990s. 19 Thus, the findings are biologically plausible.
The limitations of death coding among the oldest people prevent detailed assessment of the causes of the increased deaths. However, if influenza has indeed played a role it seems most likely to be among those rendered vulnerable by welfare cuts. Previous research in England has shown that mortality from influenza is twice or three times as high in the most deprived areas20,21 so, even if influenza is implicated, the findings presented here suggest that its associated mortality may be affected by changes to the Pension Credit system or reduced care for elderly people. As with all statistical analysis of observational studies, there is potential for other unobserved, time-varying confounding factors, although we adjusted for pre-existing time trends and relatively fixed differences across local authorities in surveillance and monitoring.
Another possibility to be considered is the existence of a cohort effect. Yet those now aged 85 years, the so-called ‘golden generation’ have been one of the most intensely studied from this point of view as they have shown especially high rates of health improvement throughout life. 22 Thus, the current decline is especially surprising. Finally, we were unable to examine social care spending on pensioners specifically, which could have biased our estimate of the impact of social care cuts downward.
Implications for clinicians and policymakers
Pensioners have been one group thought to be protected from austerity policy, as much emphasis has been placed on promises to protect the state pension, as illustrated by the aforementioned ‘Triple Lock’. However, this does not apply to the Pension Credit, which directly impacts upon the poorest older age adults, one of the most vulnerable groups in the population.
While ostensibly the decline in Pension Credit spending may seem relatively small, it is important not to consider this narrowly in relation to total income, but rather in relation to residual income after fixed costs of housing and basic utilities are taken account of. For the poorest pensioners, a change of even a few pounds could make a considerable difference to disposable income. 23 As reported, declines of this magnitude can cause significant stress and anxiety to people of older ages, which could precipitate heart attack or stroke. Other plausible mechanisms could include reduced nutrition, inadequate heating, damp or other health damaging circumstances, and social isolation. In addition, as noted above, losing eligibility will remove entitlement to other benefits. It is not possible, with the data available, to determine with certainty the mechanisms that might be involved in increased mortality. This complexity, and the multiple pathways involved, means that qualitative research may be more helpful in elucidating the roles that they play.
Our findings also have implications for the NHS. Many health service professionals have expressed concern about increasing pressure on their services attributable to cuts to social security spending. 24
In conclusion, it has widely been assumed that pensioners have been spared the worst of budgetary reductions and welfare reforms. However, some have questioned this 25 and the analysis presented here suggests that this is not, in fact, the case. Both recent and proposed future changes to welfare spending fall heavily upon pensioners. 26 The social care spending gap, exacerbated by population ageing and rising demand for services, has been projected to be £2.8 to £3.5 billion by 2019/20. 27 This suggests things will get worse for vulnerable old-age pensioners. Healthcare professionals are witnesses to the consequences of these cuts, and thus have a crucial role in drawing attention to them and advocating publicly for policies that protect some of the most vulnerable individuals in society.