
Abstract
Objective
Economic measures such as unemployment and gross domestic product are correlated with changes in health outcomes. We aimed to examine the effects of changes in government healthcare spending, an increasingly important measure given constrained government budgets in several European Union countries.
Design
Multivariate regression analysis was used to assess the effect of changes in healthcare spending as a proportion of total government expenditure, government healthcare spending as a proportion of gross domestic product and government healthcare spending measured in purchasing power parity per capita, on five mortality indicators. Additional variables were controlled for to ensure robustness of data. One to five year lag analyses were conducted.
Setting and Participants
European Union countries 1995–2010.
Main outcome measures
Neonatal mortality, postneonatal mortality, one to five years of age mortality, under five years of age mortality, adult male mortality, adult female mortality.
Results
A 1% decrease in government healthcare spending was associated with significant increase in all mortality metrics: neonatal mortality (coefficient −0.1217, p = 0.0001), postneonatal mortality (coefficient −0.0499, p = 0.0018), one to five years of age mortality (coefficient −0.0185, p = 0.0002), under five years of age mortality (coefficient −0.1897, p = 0.0003), adult male mortality (coefficient −2.5398, p = 0.0000) and adult female mortality (coefficient −1.4492, p = 0.0000). One per cent decrease in healthcare spending, measured as a proportion of gross domestic product and in purchasing power parity, was both associated with significant increases (p < 0.05) in all metrics. Five years after the 1% decrease in healthcare spending, significant increases (p < 0.05) continued to be observed in all mortality metrics.
Conclusions
Decreased government healthcare spending is associated with increased population mortality in the short and long term. Policy interventions implemented in response to the financial crisis may be associated with worsening population health.
Introduction
The sub-prime mortgage crisis which began in 2007 in the USA rapidly evolved by 2008 into a global economic crisis with severe impact on European Union member states. 1 Countries in the Eurozone with lower growth prospects and higher debt burdens were most affected. 2 Greece, Ireland and Portugal received significant financial support from the European Union and International Monetary Fund, in return for reductions in government expenditure, including government healthcare expenditure. 3 In particular, Greece has been severely hit with multiple rounds of government bailouts. As a result, there have been demands of severe reductions in government spending with worries of insufficient debt relief. 4 Other European Union member states, faced with a constrained fiscal environment, have also reduced healthcare expenditures. 5
Reductions in healthcare expenditures in the European Union have been achieved by: containing staff costs; lowering payments for pharmaceutical products and medical devices; delaying or abandoning infrastructure spending; reducing payment tariffs for clinical procedures; increasing out-of-pocket expenditures of patients or employers; and increasing waiting times. 5
Outside of the economic crisis, European health systems are experiencing several drivers to reduce costs and control expenditure. These include: ageing populations;6,7 new technologies, which have tended to be cost-creating rather than cost-reducing; 8 and chronic illnesses such as non-communicable diseases.
The association between government healthcare expenditure and health outcomes is therefore of clear importance. Previous studies have demonstrated a relationship in European Union countries in an earlier time period (1980–1995). 9 Moreno-Serra and Smith showed that this is applicable globally. 10 Greece, which recently experienced severe economic recession, austerity and reduced public health spending, has seen higher unmet medical need than prior to the financial crisis, 11 increased age standardised mortality in 2011–2012 12 and worsening under-5 mortality at the onset of the financial crisis. 13 More recent research into Europe-wide trends for healthcare spending and health outcomes are limited. Our aim was to determine the effect of changes in government spending in the European Union on population mortality, within and outside of economic crises, 1995–2010, controlling for a number of economic, geographic and medical factors.
Methods
Data extraction
Socioeconomic data for the period 1995–2010 were obtained from the World Bank’s Development Indicators and Global Development Finance 2013 edition. 14 Government debt as a percentage of gross domestic product data were obtained from the International Monetary Fund Historical Public Debt Database. 15 Mortality data were obtained from the Institute for Health Metrics and Evaluation; 16 metrics were selected on their capacity to demonstrate the effects of government healthcare spending on mortality of different age groups of society: neonatal mortality; postneonatal mortality; mortality from the age of one to five years old; adult male mortality; and adult female mortality rate.
Comparison of government healthcare spending (measured as a percentage of total government spending) in 2009 for European Union countries.
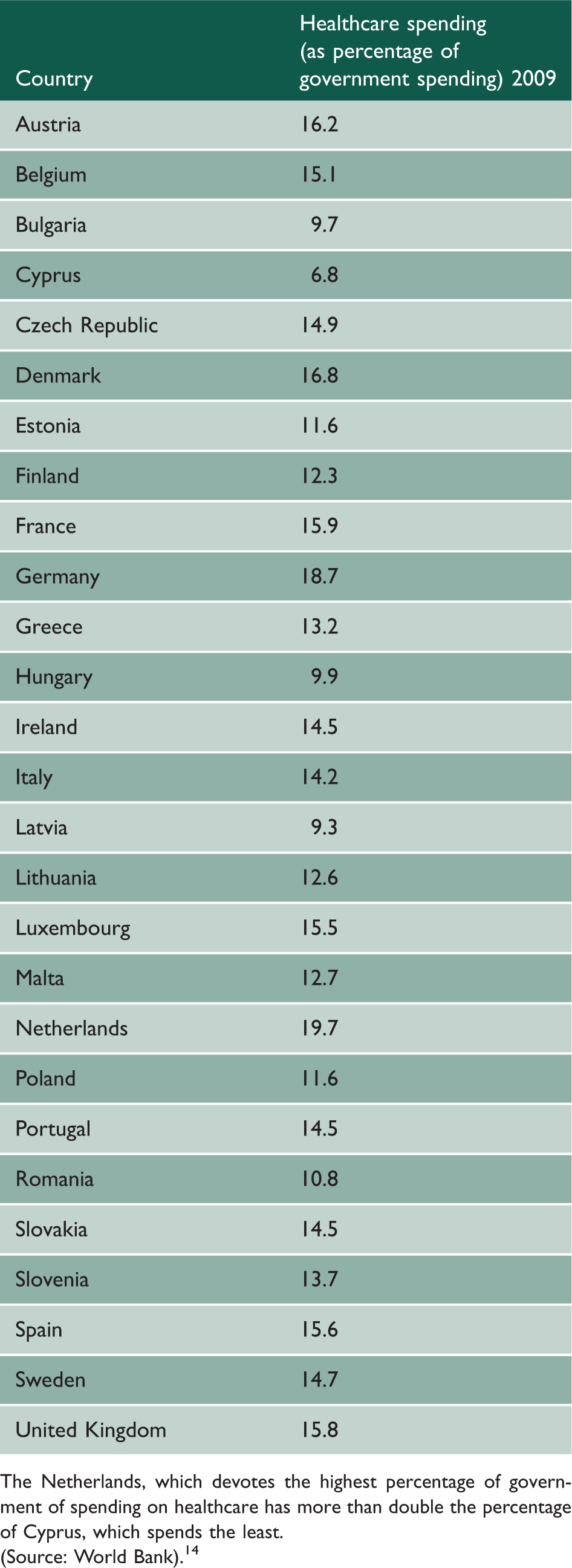
The Netherlands, which devotes the highest percentage of government of spending on healthcare has more than double the percentage of Cyprus, which spends the least.
(Source: World Bank). 14
Statistical analysis
Multivariate regression analysis was used to assess the relationship between population mortality measures (dependent variables) and government spending on healthcare (independent variable). To ensure that results were not driven by extreme observations for certain countries, a fixed-effects approach was used in the regression models, including 27 dummy variables for the 27 countries in the dataset. This approach removes potentially confounding between-country differences including higher predispositions to mortality as well as political, cultural and structural differences, while isolating the association between economic variables and mortality using within-country variations. The fixed-effects approach is more conservative than alternative analytical approaches, such as random effects or pooled ordinary least squares, because it essentially includes an additional 27 control dummy variables, losing degrees of freedom, which might be appropriate in view of the need to protect the type-I error rate from the large number of statistical tests. In effect, this conservative modelling approach made the data more comparable. Demographic structure of the countries analysed was controlled for by incorporating in the model total population size, the percentage of the population over 65 years of age and less than 15 years.
We used the Cook-Weisberg test
18
to assess for and to confirm heteroscedasticity (where subsamples have different distributions) in the data used. Therefore, robust standard errors were included in the regression models, accounting for the heterogeneity in the government spending dataset due to, for example, differences in the way countries measured spending on healthcare. We conducted analyses for each of the three measures of government spending on healthcare (as percentage of total government expenditure; measured as a percentage of gross domestic product and purchasing power parity). This methodology utilising the fixed-effects approach for cross-country analysis, has been widely used in similar health-economic studies, and is regarded as a statistically robust and conservative approach.19–24 We used the following regression model:

where i is the country and t is the year; H is the response variable or health measure (mortality); G is the predictor variable (government healthcare expenditure); α represents the population structure of the country being analysed; η is a dummy variable for each country included in the regression model; and ɛ is the error term.
We conducted 1, 2, 3, 4 and 5 time-lag multivariate analyses to quantify the long-term effects of changes in government healthcare spending on mortality.
We then conducted several robustness checks, detailed in the results section. Notably, we re-ran the analysis simultaneously introducing the following additional controls: gross domestic product per capita changes; inflation; unemployment; government debt as a percentage of gross domestic product; urbanisation; mean calorie intake; access to water; out-of-pocket expenditures; number of hospital beds per 1000; number of physicians per 100,000; and private health spending (measured as a percentage of gross domestic product) and totalling 41 controls. The regression model used was as follows:

We used Stata SE, version 12, for the analysis (Stata Corporation, College Station, TX, USA).
Results
Time lag analysis showing the association between government health spending and child mortality.
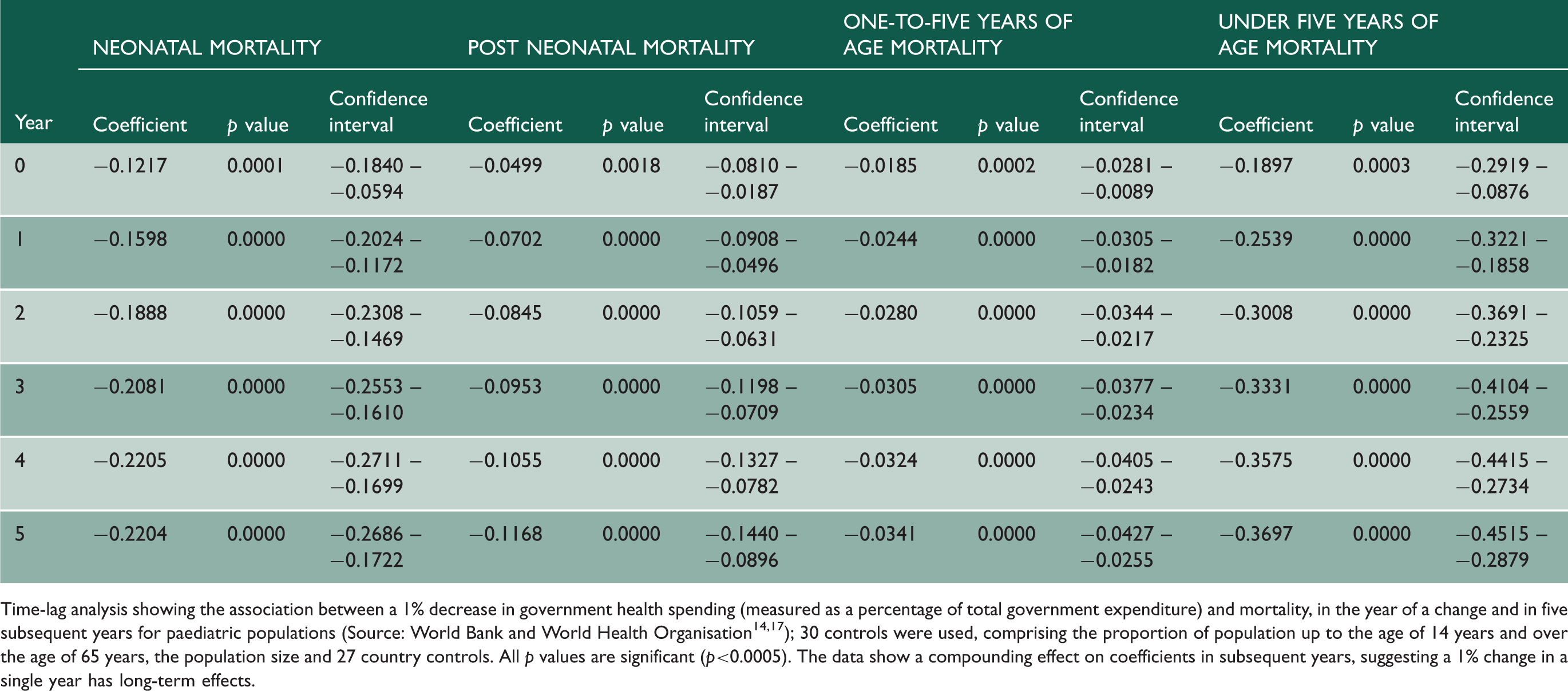
Time-lag analysis showing the association between a 1% decrease in government health spending (measured as a percentage of total government expenditure) and mortality, in the year of a change and in five subsequent years for paediatric populations (Source: World Bank and World Health Organisation14,17); 30 controls were used, comprising the proportion of population up to the age of 14 years and over the age of 65 years, the population size and 27 country controls. All p values are significant (p<0.0005). The data show a compounding effect on coefficients in subsequent years, suggesting a 1% change in a single year has long-term effects.
Time lag analysis showing the association between government health spending and adult mortality.
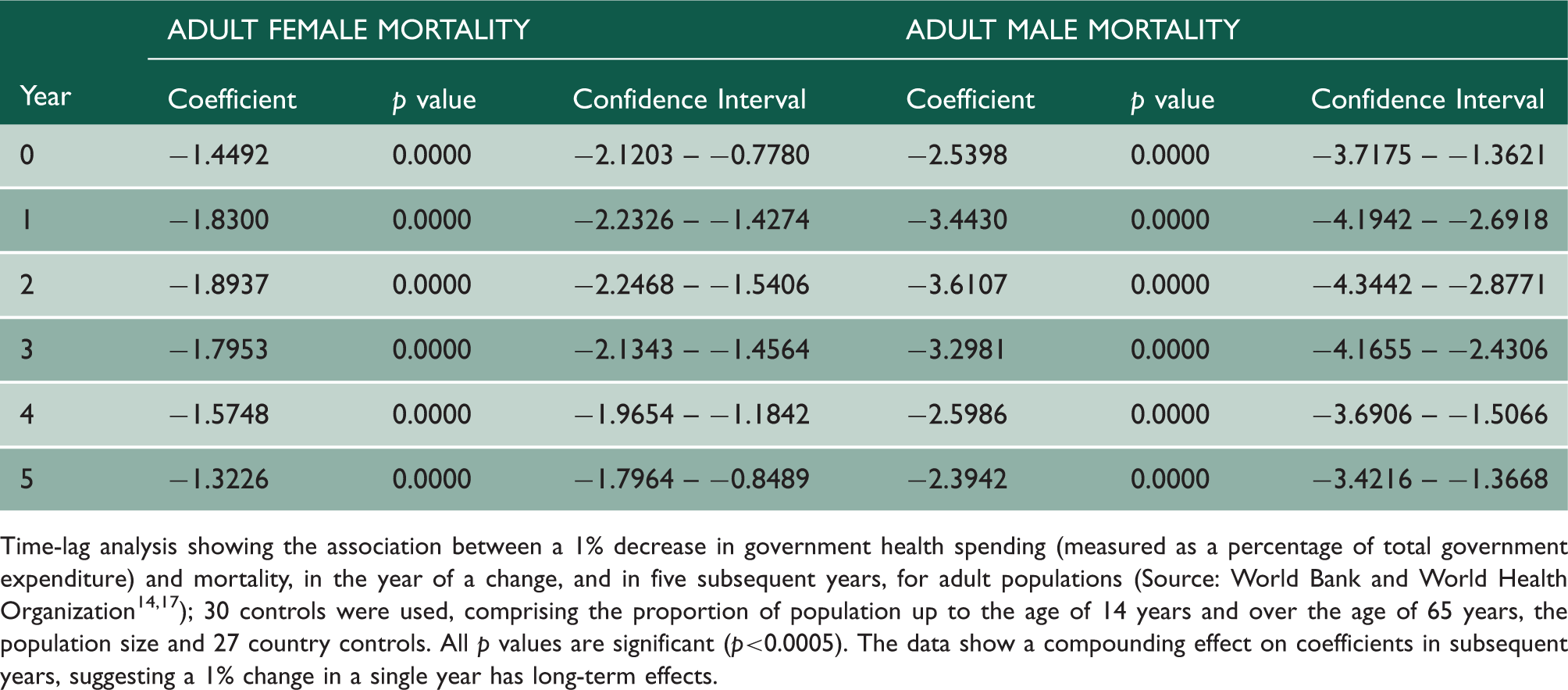
Time-lag analysis showing the association between a 1% decrease in government health spending (measured as a percentage of total government expenditure) and mortality, in the year of a change, and in five subsequent years, for adult populations (Source: World Bank and World Health Organization14,17); 30 controls were used, comprising the proportion of population up to the age of 14 years and over the age of 65 years, the population size and 27 country controls. All p values are significant (p<0.0005). The data show a compounding effect on coefficients in subsequent years, suggesting a 1% change in a single year has long-term effects.
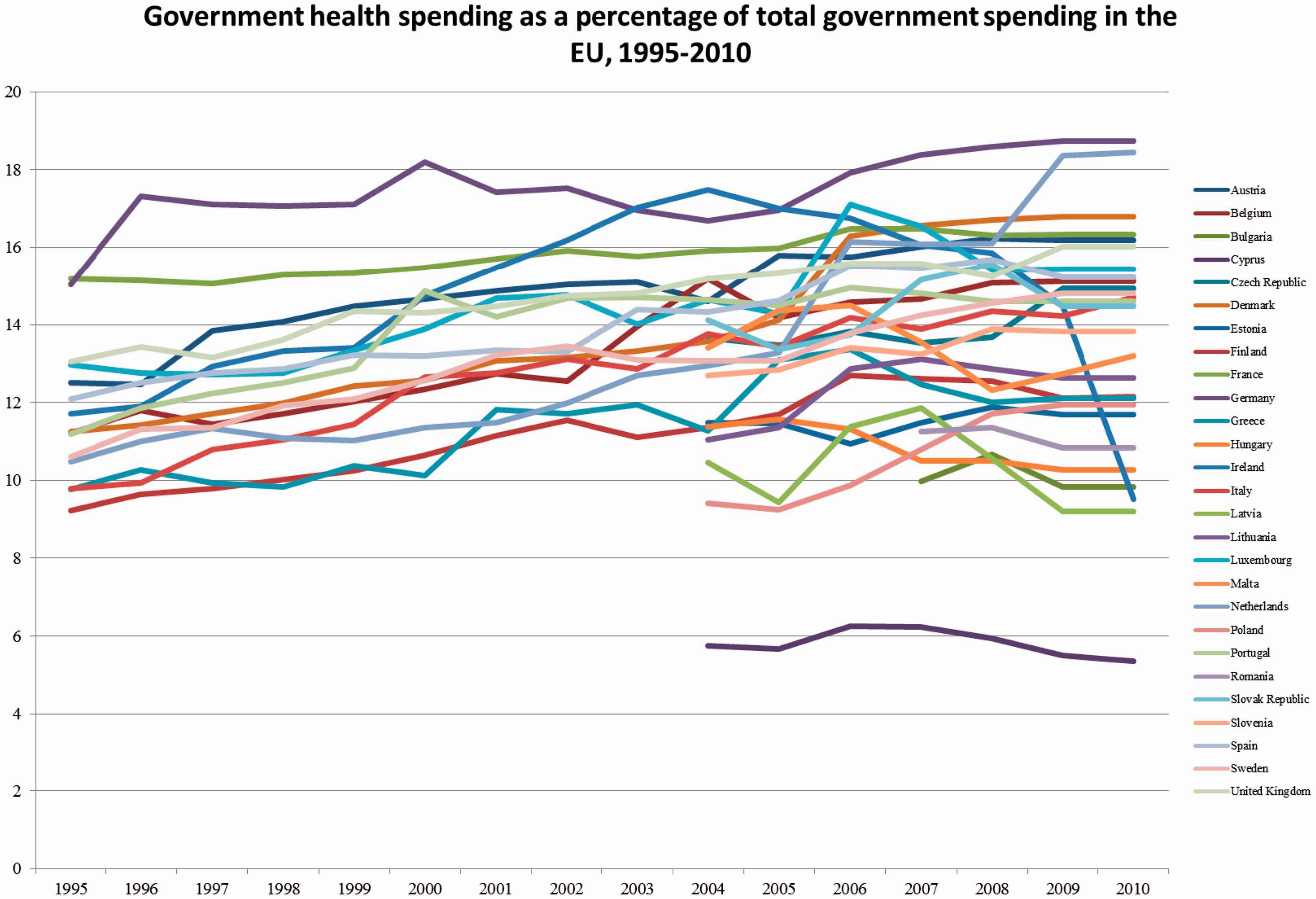
European Union spending on healthcare by country, 1995–2010.
The time-lag analysis, conducted to determine the long-term effects of changes in government healthcare spending, showed that all coefficients were statistically significant (p < 0.0005) in the five years following the reductions in government healthcare expenditures. For adult mortality in men and women, the coefficient with highest magnitude was reached at three years after the change in healthcare spending, with the effect remaining at subsequent years but at smaller magnitude (Supplementary Figures 1 to 6). For under-5 mortality, the greatest effect on mortality was at year 5, for neonatal mortality at year 4 and at year 5 for postneonatal mortality.
Supplementary Tables 1 and 2 show the effect of changes in government healthcare spending measured as a percentage of gross domestic product and as per capita spending measured in purchasing power parity. For public spending measured as a percentage of gross domestic product, all mortality measures significantly increased, as spending decreased: neonatal mortality (R −0.3402, p = 0.0000, CI −0.4344 - −0.2459); postneonatal mortality (R −0.1683, p = 0.0000, CI −0.2166 -- −0.1201); one-to-five mortality (R −0.0555, p = 0.0000, CI −0.0688 -- −0.0421); under five mortality (R −0.5624, p = 0.0000, CI −0.7159 -- −0.4089); adult female mortality (R −3.1384, p = 0.0000, CI −3.9469 -- −2.3299); and adult male mortality (R −5.1519, p = 0.0000, CI −6.6235 -- −3.6802). For changes in government spending on healthcare measured in purchasing power parity per capita, four of the five associations with mortality measures significantly increased as spending decreased: neonatal mortality (R −0.0002, p = 0.0073, CI −0.0003 -- −0.0000); postneonatal mortality (R −0.0000, p = 0.3151, CI −0.0001 - −0.0000); one to five mortality (R −0.0000, p = 0.0048, CI −0.0000 -- −0.0000); under-five mortality (R −0.0002, p = 0.0252, CI −0.0004 -- −0.0000); adult female mortality (R 0.0020, p = 0.0006, CI −0.0031 -- −0.0009); and adult male mortality (R −0.0045, p = 0.0000, CI −0.0066 -- −0.0024).
To determine potential causal pathways we re-ran analyses examining the relationship between government healthcare spending, total healthcare spending per capita, physician availability and disease-specific mortality based on established methodologies.25,26 Decreases in government healthcare spending (as a percentage of total government expenditure) were significantly associated with decreased healthcare spending per capita (measured in purchasing power parity; R 312.9, p < 0.0001, CI 211.2 to 414.6). Decreased healthcare spending per capita was associated with significantly decreased physician availability (R 0.0002, p = 0.0001, CI 0.0001 – 0.0003). Reduced physician availability was significantly (p < 0.01) associated with increased disease-specific mortality (ischaemic heart disease R −31.4304, p = 0.0000, CI −43.5010 – −19.3597; cancer R −9.9689, p = 0.0001, CI −14.7944 – −5.1434; HIV mortality R −1.3403, p = 0.0080, CI −2.3275 – −0.3532) and increased all-cause mortality (neonatal mortality R −1.498, p = 0.0000, CI −1.9341 – −1.0624; postneonatal mortality R −0.6288, p = 0.0000, CI −0.8748 – −0.3828, age one to five mortality R −0.1754, p = 0.0000, CI −0.2503 – −0.1006; under-five mortality R −2.2935, p = 0.0000, CI −3.0354 – −1.5516; adult female mortality R −11.1550, p = 0.0000, CI −14.4944 – −7.8156; adult male mortality R −19.6706, p = 0.0000, CI −26.5082 – −12.8329).
Robustness checks
To assess the validity of the results, we conducted a series of robustness checks as shown in Supplementary Tables 2 and 3. First, economic controls, namely gross domestic product per capita changes, inflation, unemployment and government debt as a percentage of gross domestic product, were included in addition to the original controls. The associations remained significant for all mortality measures; furthermore, these additions increased the magnitude of all mortality change coefficients with smaller p values than for data using only the original controls. Second, urbanisation, calorie intake and access to water were added in order to control for infrastructure-related factors. With these additional controls, there was an increased magnitude of all mortality change coefficients, with lower p values than for the original data. Additional controls for health service provision included: out-of-pocket expenditures; the number of hospital beds per 1000; the number of physicians per 100,000; and private health spending (measured as a percentage of gross domestic product). When controlling for these factors, associations remained significant. Third, we re-ran our analyses incorporating all of the abovementioned controls simultaneously (41 controls); the association between government healthcare spending and all mortality metrics remained significant (p < 0.0001). We also re-ran analyses using an alternative data source for mortality metrics (the World Bank Development Indicators 2013 14 ); coefficients were similar and p values remained significant for all mortality measures.
Discussion
Our findings suggest that changes in government healthcare spending have short- and long-term effects on population mortality, with increases in the size of the effect over time, as indicated by the rising magnitude of coefficients, for the mortality measures analysed. The change in effect size is more pronounced for adult populations than for the population under five years of age. Our findings add to a growing body of evidence linking economic indicators to health outcomes.12,27,28 The time period of our analysis includes periods of prosperity and economic difficulty, allowing us to cover periods when government healthcare spending has varied.
Our inclusion of a large number of countries permitted investigation of European Union-wide trends. Notably, our study used a conservative and robust, panel data fixed-effects regression analysis model. This model, together with the implemented robustness checks, accounts for many of the criticisms levelled at other studies looking at health-economic relationships, controlling for time-invariant heterogeneity between countries; something that aggregate, time-series analyses fail to do. Further, all data used are publicly accessible, supporting the reproducibility of our study.
Mechanisms
Our results show an association between reductions in government healthcare spending increased mortality. There are several possible mechanisms by which this may occur. The first is a direct effect on the provision of care. Failure to fund health practitioners, hospital facilities, investigative modalities and treatments could lead to errors, missed diagnoses and lack of funds to provide treatments, in turn being associated with increased mortality in the short and long term.29,30 The second effect is through the funding of public health programmes. These measures can be targeted at communicable diseases, such as vaccination programmes 31 , at non-communicable diseases, such as nutritional and stop-smoking programmes, or at both, in the case of breastfeeding programmes. 32 Public health programmes often affect children and are likely to affect health over the longer term. It follows that reductions in funding of such programmes may be associated with worse long-term population health.
Inclusion of robustness variables increases the strength of association of our variables. International datasets are inherently noisy due to variability in measurement methods between different countries and other confounds. If, through our controls, we are able to reduce the noise in our dataset, it is perfectly possible for our p values to strengthen.
Limitations and recommendations for future study
This study has several limitations. First, in our analysis of health outcomes, we have only used mortality measures. The effects of changes in spending on other health measures could yield different results. 9
Second, we have not modelled intra-year variations in mortality; however, by looking at whole years we eliminate spurious trends that might be seen which are seasonal in nature.
Third, we have not controlled for reverse causality since, on first principles, this seemed unlikely. Changes in the number of people that die would have to be disproportionate to the measures of government spending used and our analyses show that one year of change in government spending has longer lasting effects on mortality than one year. Were we to suspect reverse causality, this would not be the case.
Fourth, we do not entirely control for measurement error; however, our controls for heteroscedasticity already partially control for this, since heteroscedasticity is a source of measurement error.
Fifth, our measures look at government healthcare spending and mortality for the entire population of countries. We have not segmented populations by socioeconomic status or by geographic location to give further granularity or show which population groups might have been most affected. This is of relevance as the inverse care law suggests that populations with lower socioeconomic status typically have poorer healthcare provision, 33 and times of economic hardship would likely have greater adverse effect on the poorest members of society.
Sixth, although we focus the quantity of government spending on healthcare, we do not factor how efficiently or effectively these funds were spent. Indeed, it is entirely feasible that a country may spend less on healthcare and achieve greater outcomes due to efficient application of funds or avoidance of ineffective or inappropriate interventions. 34 Future work could examine more whether there are closer correlations between health system archetypes.
Seventh, for reasons of data availability, we were unable to analyse the effects of the economic downturn from 2011 onwards. However, in addition to the sizeable economic fluctuations that occurred during the period studied, our analysis was able to capture the effects of the earlier stages of the recent economic downturn, during which changes in government spending in several countries decreased.
Lessons for policy makers
Our study has several implications for policy-makers at the national and international level. First, our findings demonstrate that macro-level multinational policy, similar to technologies or healthcare interventions, can impact mortality at the individual level. Second, we note that many governments have implemented austerity measures in response to the financial crisis, 2 either due to government policy or under compulsion after accepting financial assistance packages following problems with bound monetary policy in the Eurozone. 2 An analysis of healthcare spending in the European Union between 1995 and 2011 showed that austerity was significantly associated with the need to accept International Monetary Fund Assistance. 36 Austerity measures have been associated with reduced public spending, 2 and may be exacerbating the adverse health effects of the global economic downturn rather than ameliorating them. More generally, times of reduced government spending, such as recessions or governmental instability, are likely to result in longer-term effects on mortality than previously envisaged.
Conclusion
Reductions in government healthcare spending may be associated with increased population mortality. These changes do not only have an effect in the year that they occur but are felt for several years. Given the risk of injudicious reductions in health expenditures, we caution that reduced government spending should be achieved through increased efficiency of care delivery.
Footnotes
Declarations
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.