
Abstract
Lesson
Temporal lobe epilepsy is a rare but treatable cause of apnoea.
A previously fit and well 47-year-old teacher initially presented in 2007 with a two-year history of recurrent episodes characterised by a sensation of detachment followed by speech disturbance, lasting 60 s on each occasion. These were occurring on average every three months. She retained awareness, had no post-event confusion and no motor automatisms. A magnetic resonance imaging (MRI) brain scan and electroencephalography (EEG) were unremarkable.
The possibility of simple partial seizures was considered but the symptoms were thought atypical; there was a strong temporal relationship with increasing stress at work and the patient was concerned about starting potentially long-term anti-epileptic medication. The episodes settled spontaneously and she remained well until November 2008, when following a particularly stressful and busy week, she suffered an episode of involuntary nocturnal vigorous chest thrusting lasting 20 min, followed by apparent unresponsiveness and mild confusion for 10 min. A repeat EEG and MRI were again unremarkable.
After reducing her workload, no further events occurred until October 2009 when she experienced an episode characterised by severe postural arching of her back followed by waking up gasping for breath. Identical episodes, arising only from sleep, occurred over the next few months. Home oximetry studies recorded desaturations of less than 60%. Formal spirometry was normal and she was extremely fit, running in excess of 25 miles per week. Her sleep study was unremarkable although no episodes occurred during the recording period. She was reviewed by the respiratory team, and a primary respiratory mechanism was thought to be unlikely.
After repeated sleep studies and EEG recordings without capturing a clinical event, a five-day period of video EEG/ECG telemetry showed rare interictal epileptiform abnormalities over the left temporal lobe at night. Neither nocturnal attacks nor desaturations were recorded. In light of the EEG findings, the MRI was repeated and revealed a subtle area of cortical dysplasia around the left amygdala and adjacent cortex (Figure 1).
MRI brain with arrow showing left cortical dysplasia.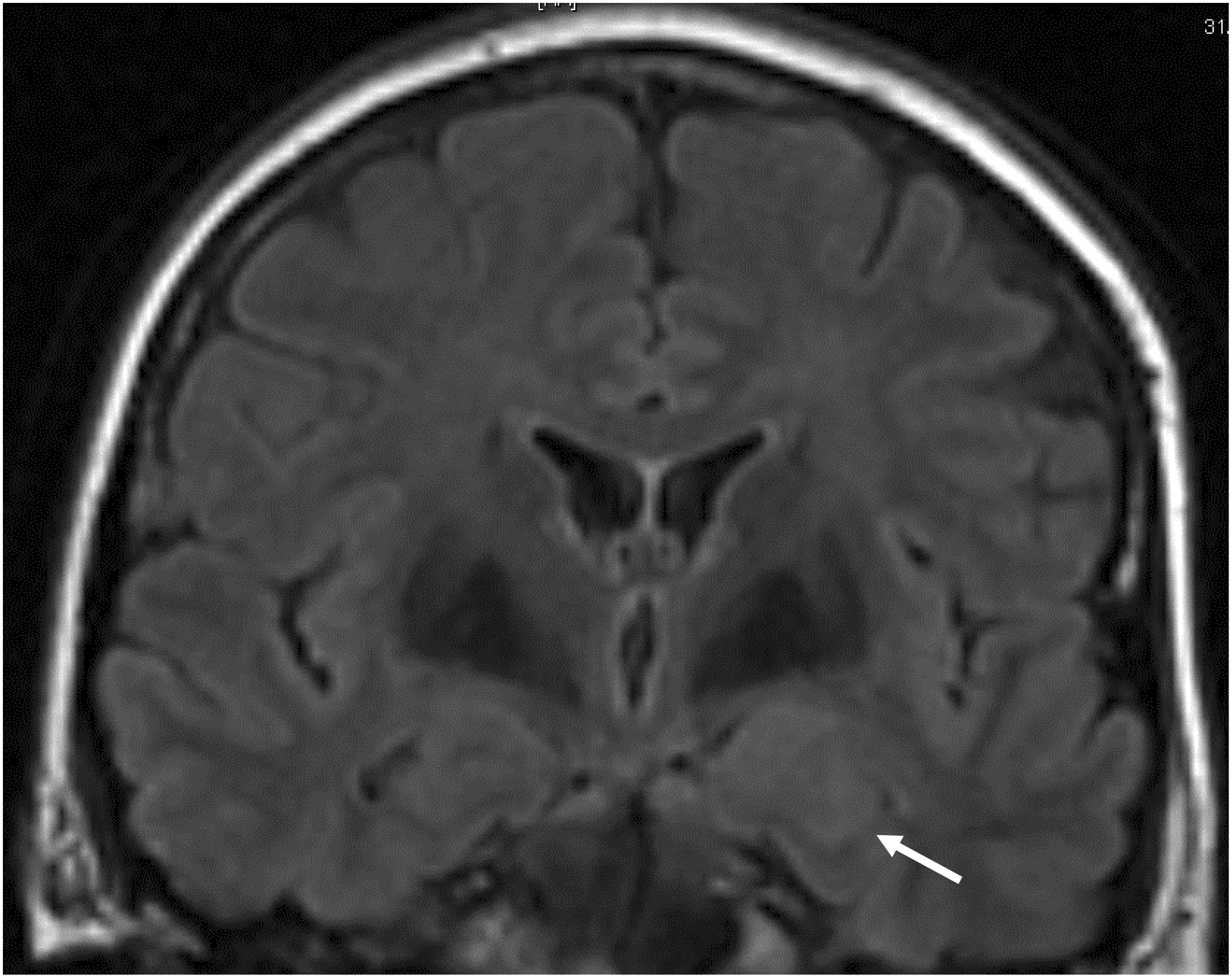
A presumed diagnosis of ictal apnoea was made and anti-epileptic medication was recommended. The patient developed significant side-effects, such as sedation, cognitive slowing and dizziness at low doses of a number of different medications, including levetiracetam, clobazam and lamotrigine, and she was concerned about the veracity of the diagnosis. Finally, another video EEG study captured two EEG events typical for left temporal lobe seizures with a 23-s period of apnoea preceding the second event (Figure 2). The dose of her anti-epileptic medication, lacosamide, was increased and her seizures improved subsequently.
EEG showing a 23 second period of apnoea (red arrow) prior to epileptiform activity (blue arrow).
Hypoventilation during sleep can be due to obstructive or central causes. Although most cases are due to obstruction, a normal body habitus with no evidence of snoring should raise the suspicion of a central cause. Central sleep apnoea is characterised by the interruption of airflow and respiratory effort for at least 10 s on polysomnography. 1 The most common causes are primary central apnoea, drug-related apnoea, Cheyne-Stokes breathing pattern often seen in heart failure and apnoea in stroke and neurodegenerative diseases. 2
Ictal apnoea is a rare but treatable cause. The unusual seizure semiology during our patient’s nocturnal episodes is likely to be due to the additional effects of the apnoea/hypoxia. Ictal apnoea is important to recognise, as this is a candidate pathophysiological mechanism underlying sudden unexpected death in epilepsy (SUDEP). Alternative mechanisms include cardiac dysrhythmias and post-ictal generalised EEG suppression, ‘cerebral shutdown’. SUDEP is defined as sudden death that is not due to trauma, drowning, status epilepticus, a structural or toxicological cause. 3 Sudden death is 20 times more likely in epileptics than the general population and increased frequency of generalised tonic clonic seizures is the major risk factor. 3 However, nocturnal supervision confers some protection. 4
In our case, the diagnosis was not straightforward. Typically, temporal lobe seizure semiology includes déjà and jamais vu, a rising epigastric sensation, olfactory or gustatory hallucinations, aphasia and automatisms. 5 Impaired consciousness and amnesia during the event may occur. Our patient had speech disturbance but no other key features. Diagnosis was only made after repeated video EEG telemetry. This case reports the unusual presentation of ictal apnoea in temporal lobe epilepsy and illustrates the importance of persistence in investigating patients with undiagnosed intermittent symptoms. Importantly, clinicians should be aware that while correct diagnosis means treatment can be initiated, an incorrect verdict causes unwarranted stress and anxiety.
Footnotes
Declarations
Ethical approval
Written informed consent for publication was obtained from the patient.