
Abstract
Summary
Objectives
To report the career progression of a cohort of UK medical graduates in mid-career, comparing men and women.
Design
Postal and questionnaire survey conducted in 2010/2011, with comparisons with earlier surveys.
Setting
UK.
Participants
In total, 2507 responding UK medical graduates of 1993.
Main outcome measures
Doctors’ career specialties, grade, work location and working pattern in 2010/2011 and equivalent data in earlier years.
Results
The respondents represented 72% of the contactable cohort; 90% were working in UK medicine and 7% in medicine outside the UK; 87% were in the UK NHS (87% of men and 86% of women). Of doctors in the NHS, 70.6% of men and 52.0% of women were in the hospital specialties and the great majority of the others were in general practice. Within hospital specialties, a higher percentage of men than women were in surgery, and a higher percentage of women than men were in paediatrics, obstetrics and gynaecology, clinical oncology, pathology and psychiatry. In the NHS, 63% of women and 8% of men were working less-than-full-time (in general practice, 19% of men and 83% of women; and in hospital specialties, 3% of men and 46% of women). Among doctors who had always worked full-time, 94% of men and 87% of women GPs were GP principals; in hospital practice, 96% of men and 93% of women had reached consultant level.
Conclusions
The 1993 graduates show a continuing high level of commitment to the NHS. Gender differences in seniority lessened considerably when comparing doctors who had always worked full-time.
Introduction
Doctors in the early stages of their careers are widely surveyed nowadays,1–4 and there are some published surveys of doctors approaching retirement.5–7 However, there are relatively few large-scale studies of doctors who have reached senior positions but are still far from retirement. It is very important for workforce planning to understand, at a whole-cohort level, the contribution to the workforce made by doctors in mid-career, and to understand their likely future career dynamics.
We have surveyed UK-trained doctors who graduated in 1993 on several occasions.8–13 Here, we describe their career progression in 2010/2011, approximately 17 years after graduation from medical school.
The aim of this paper is to report on these doctors’ employment, achievement of senior positions and working patterns at this mid-career stage, with particular emphasis on differences between men and women.
Methods
Since 1975, the UK Medical Careers Research Group has followed the careers of UK doctors by conducting regular postal and, more recently, web questionnaire surveys. Our methods are described fully elsewhere. 13
In their first postgraduate year, we sent postal questionnaires to all doctors who graduated in 1993 from all UK medical schools, having obtained their contact details from the General Medical Council (GMC). Contact information has been updated since then using information from both the GMC and the doctors’ own replies to successive surveys. These doctors have subsequently been surveyed in their third, fifth, ninth, 12th and most recently 17th postgraduate year, in 2010/2011.
The surveys comprised structured, ‘closed’ questions and statements, plus a few ‘open’ questions. Topics included career choice, current employment, jobs since our previous survey, future career plans, views about different aspects of their jobs/training and demographic information. We also asked for ‘free text’ comments on any aspect of the respondents’ career or work, the results of which, for this survey of the qualifiers of 1993, we report in an accompanying paper.
The specialties indicated by respondents in career choices and employment sections of the surveys were aggregated into specialty groups based on those initially defined in the Todd Report. 14
Doctors were asked ‘Apart from temporary visits abroad, do you intend to practise medicine in the United Kingdom for the foreseeable future?’ They had a choice of five responses: Yes-definitely, Yes-probably, Undecided, No-probably not and No-definitely not. Those who did not reply Yes-definitely to this question were asked to indicate whether they were considering one or more options from practising medicine abroad, leaving medicine but remaining in the UK or leaving medicine and leaving the UK. Respondents not working in UK medicine were asked whether they planned to return, responding on the same five-point scale from Yes-definitely to No-definitely not.
Quantitative methods of analysis used were descriptive statistics, chi-squared tests (Mantel–Haenszel χ2 is reported for linear trends) and binary logistic regression. Since multiple similar analyses were performed on the same dataset, we regarded the attainment of a level of significance of p ≤ 0.01 as evidence of real difference.
We used data about respondents in combination with Department of Health employment data using the method of capture-recapture analysis as previously reported elsewhere, 13 to enhance the accuracy of our estimates of the percentage of the whole cohort working in the NHS 17 years after graduation.
Results
Survey response
Excluding from the survey 17 doctors in the original who were deceased, 30 who had declined to participate and 145 who were untraceable after extensive searching, the response rate 17 years after graduation was 72.1% (2507/3479). Half the respondents (1252 doctors) were women.
Career destinations (Table 1)
Of respondents, 97% were working in medicine, comprising 90% who were in UK medicine and 7% who were working in medicine elsewhere. Some respondents held several medical posts: for example, 87% of respondents held a post in the UK National Health Service (NHS) with 5% also holding a post in UK private medicine and 11% working in UK academic medicine.
For comparison, the percentage of the whole cohort, including survey non-respondents, estimated to be working in the NHS using capture-recapture analysis was 86% (86.4% of men and 85.3% of women).
Family home location prior to medical school was known for 2451 of 2507 respondents. 87% (2063/2379) of those from UK homes were working in the NHS compared with 74% (53/72) of those from non-UK homes (
Career destinations of UK medical graduates of 1993 in 2010/2011: percentages of all respondents.

Specialties in the NHS
Of 2172 doctors with an NHS post, 61.4% (1334) were in hospital practice, 37.2% (807) in general practice and 1.4% (31) in public health medicine, community health or other medical specialties.
Men were much more likely than women to be working in a hospital specialty (70.6% (774/1096) and 52.0% (560/1076), respectively) and were less likely than women to be working in general practice (28.6% vs. 45.9%).
Excluding doctors in general practice and doctors who were not in the NHS, the percentage breakdown of men and women across the 10 NHS hospital specialty groups differed (χ29 = 138.0, p < 0.001): 28.8% of the men and 7.4% of the women in hospital specialties were surgeons, and other substantial differences were paediatrics (6.5% of men and 12.7% of women), obstetrics and gynaecology (2.3%, 6.7%), clinical oncology (3.2%, 6.9%), pathology (2.1%, 5.8%) and psychiatry (7.3%, 12.5%) (Table 1). The specialty distribution of all doctors (excluding general practitioners, GPs), including doctors in practice outside the UK, is shown in Table 1.
Working pattern in the NHS
Percentages and numbers of doctors who graduated from UK medical schools in 1993 working less than full-time in the NHS in 2010.
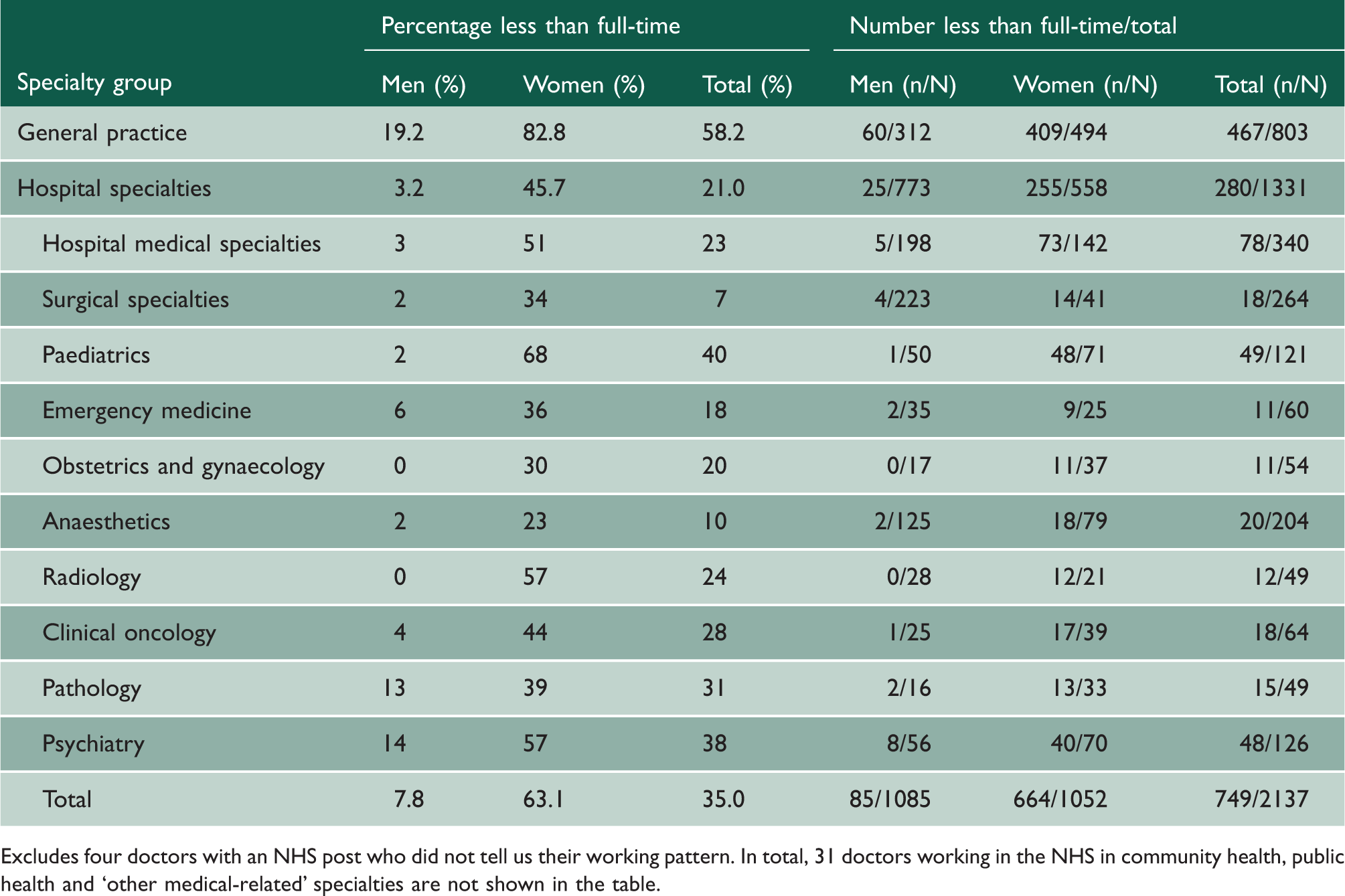
Excludes four doctors with an NHS post who did not tell us their working pattern. In total, 31 doctors working in the NHS in community health, public health and ‘other medical-related’ specialties are not shown in the table.
Achievement of senior career posts in the NHS
(a) Current post
At the time of the survey, 73% of NHS GPs and 90% of NHS hospital doctors were working at senior grade level, as GP principals or consultants respectively (Table 3). In general practice, 89% of men and 62% of women were in senior posts. In hospital practice, 95% of men and 84% of women were in senior posts. Career-long working patterns made a considerable difference to the figures: 93% of NHS GPs and 95% of NHS hospital doctors who had always worked full-time were in a senior post. The corresponding figures for NHS doctors working less than full-time were 59% and 74%, respectively. Within each work pattern, the gender difference in seniority was small and not statistically significant (Table 3). However, the much larger numbers of women than men who were working part-time meant that overall a higher percentage of men than of women were in senior positions (Table 3). Of NHS doctors who had always worked full-time, emergency medicine, obstetrics and gynaecology, clinical oncology and psychiatry showed the greatest gender difference in the percentage working in a senior post (Table 4). However, none of the gender comparisons reached statistical significance.
(b) Highest grade achieved
We also knew, for 2169 NHS doctors, whether they had achieved a senior grade at some point previously in their career, regardless of whether they were working in a senior position at the time of the survey. In all, 95% of men and 77% of women GPs (
Percentages of NHS general practitioners and hospital doctors working in senior posts 17 years after graduation by gender and employment group.

Figures include five NHS general practitioners/hospital doctors who held a professorship position, but no clinical post (they were counted with GP principals or consultants, depending on their specialty) and exclude seven whose grade was not known.
Percentages of NHS hospital doctors who have always worked full-time and who were in consultant posts 17 years after graduation by gender and mainstream specialty.

Figures represent NHS doctors who indicated that they have always worked full-time, excluding those whose grade was not known. Fisher’s exact test shows that there were no significant differences between men and women in the attainment of consultant posts.
NA: not applicable.
Logistic regression showed that for NHS hospital doctors who had always worked full-time, gender (Wald
Intention to practise medicine in the UK in the future
In 2010, 95.5% of UK-based respondents definitely or probably intended to continue practising medicine in the UK for the foreseeable future. NHS doctors were more likely than UK-based doctors working in medicine outside the NHS to hold this view: (96% (2072/2159) compared with 84.3% (70/83), (
In all, 8.4% of UK-based respondents specified that they were considering leaving medicine; 13.3% were considering practising medicine abroad; and 2.1% were considering the possibility of either leaving medicine or emigrating.
Of respondents who worked in medicine abroad and answered the question, 10.2% (17/166) indicated that they definitely or probably planned to return to UK medicine.
Late changes in location
Of those who responded in both years, between postgraduate years 9 and 12, 1.4% of doctors moved abroad and 2.3% returned to the UK; between years 12 and 17, 2.3% of doctors moved abroad and 2.3% returned to the UK.
Late changes in employment
Of respondents who provided their employment details in both years, 7.6% (185/2446) changed their employment between postgraduate years 9 and 12 (men 5.0%, 61/1227 and women 10.2%, 124/1219;
Between years 12 and 17, the corresponding figures were 6.2% (142/2274) who changed their employment (men 3.5% and women 8.9%;
Working pattern over time
Numbers and percentages of doctors who graduated from UK medical schools in 1993 who were working part-time in medicine in the UK and in the NHS 9, 12 and 17 years after graduation, by gender and whether in hospital or general practice.

Discussion
Main findings
The vast majority of respondents were working for the NHS 17 years after graduation. This included those respondents whose home location at the time of their application to medical school was outside the UK. Women were just as likely as men to be working in the NHS 17 years after graduation. Just over a third of NHS doctors who responded were working in general practice, with women outnumbering men in general practice by about three to two.
The almost identical estimates of NHS participation obtained by capture-recapture analysis and by analysis of data from responders suggest that our responder data of 1993 graduates working for the NHS were unaffected by responder bias.
About a third of NHS doctors worked less than full-time, with women being almost eight times more likely to be working part-time than men. The percentage of UK and NHS women doctors working less than full-time significantly increased between their ninth and 17th postgraduate years. There was no such increase among men.
The majority of the 1993 graduates who in year 17 worked in the NHS had reached senior career grade status as consultants or GP principals. Hospital doctors were more likely to be working in a senior grade than were GPs, and men were more likely to do so than women. However, the differences between men and women in the level of attainment of a senior grade reduced, and were not significant, when the analyses were restricted to doctors who had always worked full-time. Comparing hospital specialties, doctors in emergency medicine were notably least likely to be working in a senior post.
A large majority of UK-based doctors who graduated in 1993 intended to continue to practise medicine in the UK for the foreseeable future. The NHS doctors were significantly more likely than the other UK doctors to indicate that they intended to do so. There were no gender differences. Some respondents were considering practising medicine abroad (15%) and about 10% were considering leaving medicine. However, when looking back to the period between their ninth and 17th postgraduate years, about the same percentage returned from abroad as went abroad and the same percentage returned to medicine as left it. The percentages of both returners and leavers were higher for women than for men. A similar, small, percentage of men and women doctors changed their specialty during this period of their careers.
Strengths and weaknesses of the study
The study was national, spanned many years and had an excellent response rate for a self-completed survey, at each survey administration, many years after the first survey of the doctors in their first year after qualification. Some level of non-response is inevitable, and responder bias is possible. However, the results from the analysis of respondents and from capture-recapture show that there is almost no non-responder bias in whether the doctors were, or were not, working in the NHS.
Implications and conclusions
The graduates of 1993 showed a continuing high level of commitment to working in the NHS. However, the equal commitment of men and women is notable, as is the almost equal level of women and men reaching senior positions once account is taken of less-than-full-time working. This, in a more recent cohort, confirms our previous research based on cohorts of qualifiers from the 1970s and 1980s. 15
A small percentage of doctors leave the UK, but they may not represent a net loss to UK medicine of UK-qualifiers. Our results, limited to this cohort, show that at each career stage roughly the same percentage of our respondents returned to UK medicine as went to work abroad. A small percentage of senior doctors decide to change their specialty at a later stage and workforce planners may wish to take this possibility into account. It may prove possible to provide career advice, to assist doctors wanting to change direction, if their hopes are expressed and discussed.
Adsett and Roddis 16 discuss how it can sometimes be daunting and disheartening for a senior doctor to work in the same post for several decades. They persuasively argue that even consultants need help with career planning. The provision of additional, well-publicised and accessible career advice for senior doctors might help ensure that fewer doctors are lost from the NHS, for example due to early retirement through disillusion. Perhaps some may be enabled to change their career to a shortage specialty after appropriate re-training.
Our findings for the 1993 cohort suggest that the biggest single issue in relation to workforce capacity relating to senior doctors is not loss from emigration or leaving medicine, but the fact that more and more doctors, particularly women, want to work less than full-time. This tendency will have a greater impact on some specialties than others, since the proportion of women varies from specialty to specialty, 17 and part-time working is more common among some specialties than others.
In practice, part-time clinical roles in hospital medicine are not uncommon: many senior doctors take on academic, managerial or private practice commitments. 18 Part-time working for family reasons should be as acceptable as part-time working for these. This would be in line with the Improving Working Lives Standard, a framework produced by the NHS Staff Council and aimed at achieving good work-life balance among NHS employees. 19 However, Gray et al. 20 point out that there needs to be a working culture that ensures that part-time consultant posts are welcomed.
A proportion of senior doctors will opt to work part-time. This proportion is likely to increase most obviously because of the increasing number of women doctors but also because of other factors. 17 Availability of career posts with flexible working patterns is likely to result in more doctors being able to work full-time, and a greater number of hours being covered by those working part-time.
We hope to continue to monitor career progression of this and other graduation cohorts. There has been a number of developments relevant to the NHS doctors, since 2010, in particular the Public Service Pensions Act 21 and the Health and Social Care Act. 22 It will be interesting to see whether the same high level of commitment to the NHS will be found among doctors who are senior, but still decades away from retirement, in the future.