
Abstract
Introduction
Vision health is an important and underutilized health service among newly arrived refugees in Canada, yet the body of literature on eye-care delivery in this population is limited. The study objective was to identify patterns of eye-care utilization among refugee patients with type 2 diabetes mellitus (T2DM) in Newfoundland and Labrador (NL) under an interdisciplinary clinic model comprised of family physicians, eye-care providers, and settlement services.
Methods
This was a retrospective cohort study at the Memorial University Family Medicine clinic. All patients with a new T2DM diagnosis between 2015–2020 were included. Data were described using basic statistics and unpaired t-tests. This study received full ethics approval.
Results
Seventy-three (18 refugee, 55 non-refugee) patients were included. Refugees had a higher rate of referral to an eye-care provider (p = 0.0475) and were more likely to attend their eye-care provider appointment than non-refugees (p = 0.016). The time from diagnosis to referral was longer for refugees than non-refugees (p = 0.0498). A trend towards longer time from referral to appointment attendance for refugees than non-refugees was noted (p = 0.9069).
Discussion
Refugee patients had higher rates of referral to eye-care providers and utilization of eye-care services. However, refugees also experienced a longer time to access vision screening services suggesting possible gaps in accessible care delivery. This suggests that the interdisciplinary model of care may be effective in referring refugee patients for vision screening and there may be a role for increased collaboration across family physicians, eye-care providers, and settlement services to improve accessibility of vision screening services.
Introduction
Eighty million individuals globally have been forcibly displaced due to conflict, persecution, and human rights violations. 1 Refugees comprise 26.3 million of all displaced persons, of whom over 1 million have resettled in Canada.1,2 The current body of literature on refugee health reveals disparities in equitable access to care due to the cultural, linguistic, and socioeconomic barriers that are often faced during migration and resettlement.3–7 This may manifest as underutilization of health services which are known to be more challenging to access for vulnerable populations. Vision screening is an important health need and a critical locus for underutilization of health services among refugees resettling in Canada.7–10 Additionally, there is a disproportionate emphasis on infectious disease screening with underscreening for chronic non-communicable diseases, such as type 2 diabetes mellitus (T2DM). 5
Diabetic retinopathy is a leading and preventable cause of blindness that is associated with higher relative morbidity and mortality.11,12 Guidelines recommend screening for diabetic retinopathy with an eye-care provider—optometrist or ophthalmologist—at the time of T2DM diagnosis. 12 Diabetic retinopathy screening lies at the intersection of many documented challenges in access to care for refugees: it is a chronic non-communicable disease, 5 requires coordination between primary care and specialist services,2,5 and is most effective when patients are asymptomatic and thus not actively seeking care.
To date, there is a limited body of evidence on the ocular health of refugees in Canada and no known studies on diabetic vision screening among refugees. This study seeks to identify patterns of eye-care utilization among refugee and non-refugee patients with T2DM in Newfoundland and Labrador (NL).
Methods
We conducted a retrospective comparative cohort study at the Memorial University Family Medicine clinic in St John's, NL, Canada. NL has a population of approximately 520,000, 13 with 1,765 resettled refugees from 2015 onwards. 14 The province has the highest prevalence of diabetes (type 1 and type 2) or prediabetes in Canada, estimated at 35%, with a direct cost to the healthcare system of $546 million. 15 NL does not provide publicly insured routine eye examinations (i.e. vision screening by an optometrist), and the rate of eye-care utilization is 36.3%—lower than other Canadian provinces, both with and without publicly insured eye examinations. 16
The Memorial University Family Medicine clinic includes a dedicated refugee clinic designed to improve access to public and preventative health services for newly arrived refugees.2,17 This unique clinic model refers all newly arrived refugee patients to an optometrist for comprehensive eye exam to benefit from the Interim Federal Health Program (IFHP). 18 To our knowledge, routine referral of all newly arrived refugees to an eye-care provider for vision screening is not described in the existing literature.
The process of liaising newly arrived refugee patients with eye-care providers under this clinic model relies on three pillars of support: a dedicated refugee clinic, the IFHP, and community settlement services.17–20 The refugee clinic is typically the first point of contact with the healthcare system for newly arrived refugees and is designed to provide long-term continuity of care by connecting patients with a family physician early in the resettlement process. Among its many services, the refugee clinic provides preventive healthcare and facilitates routine referrals to optometric vision screening for all newly arrived refugees. 17 The IFHP provides partial insurance coverage of optometric services for one year after arrival. 18 Thus, the refugee clinic aims to refer all newcomers to an optometrist during this period. Once IFHP coverage expires, eye exams with an optometrist are not publicly insured and thus patients without private insurance are referred to an ophthalmologist for T2DM screening. Ophthalmology services are publicly insured but typically incur longer wait times. Lastly, community settlement services liaise with the refugee clinic to provide health navigation support such as interpreters, appointment coordination, and transportation when possible.17,20
Data were collected from the Memorial University Family Medicine clinic's electronic medical record. All patients with a new T2DM diagnosis at the clinic between 2015–2020 were included. Patients who were lost to follow-up due to relocation, death, or otherwise unknown reasons were excluded. Outcomes of interest were gender, age, country of origin, date of T2DM diagnosis, date of eye-care provider referral, and date of eye-care provider appointment attendance. Demographic data were described using descriptive and basic statistics. Unpaired t-tests were utilized to assess differences in the time from T2DM diagnosis to referral to an eye-care provider, time from referral to an eye-care provider to appointment attendance, and rates of referral to an optometrist versus an ophthalmologist among the refugee and non-refugee cohorts. A p-value less than 0.05 was considered statistically significant. Statistical analyses were performed with GraphPad Prism Version 9.1.0 (GraphPad Software Inc., CA, US). This study received full ethics approval from the Newfoundland and Labrador Health Research Ethics Board (2020.118) and was conducted in accordance with the Declaration of Helsinki.
Results
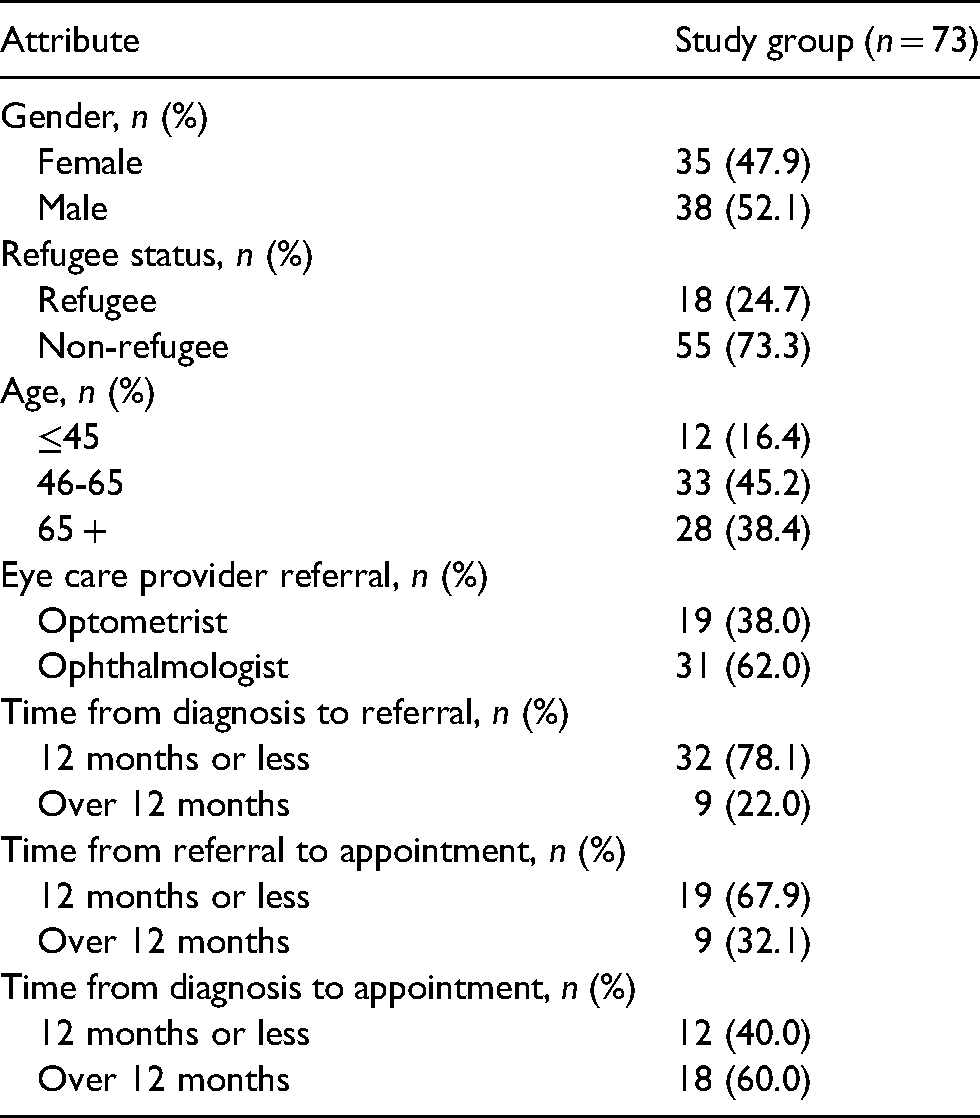
Between 2015–2020, 726 newly arrived refugees received care through the clinic. Seventy-three patients were diagnosed with T2DM during this period—18 (25%) were refugees and 55 (75%) were non-refugees. There were 35 females (48%) and 38 males (52%). Only 12 patients (16%) were younger than age 45, while 33 patients (45%) were between the ages of 46–65 and 28 patients (38%) were older than age 65. Nineteen patients (38%) were assessed by an optometrist and 31 patients (62%) were assessed by an ophthalmologist. Countries of origin for refugee patients included Eritrea, Syria, Sudan, Iraq, Palestine, and Republic of the Congo.
Rates of referral and appointment attendance for refugees were 89% and 61%, respectively. Rates of referral and appointment attendance for non-refugees were 47% and 35%, respectively. Time from diagnosis to referral was less than 12 months for 78% patients, time from referral to appointment was less than 12 months for 68% of patients, and time from diagnosis to appointment was less than 12 months for 40% of patients. Among both refugee and non-refugee cohorts, there were no statistically significant differences in rates of referral by gender (p = 0.6875). However, there was a statistically significant difference for rates of referral by age, with higher rates of referral among older patients (p = 0.0131).
Refugees were more likely to be referred to an optometrist rather than an ophthalmologist (p = 0.0013) and had a statistically significant higher rate of referral to an eye-care provider than non-refugees—89% versus 47% (p = 0.0475). Refugees were also more likely to attend their eye-care provider appointment than non-refugees—66% versus 35% (p = 0.016). The time from diagnosis to referral was longer for refugees (309 days) than non-refugees (128 days) (p = 0.0498). A trend towards a longer time from referral to appointment attendance for refugees (598 days) than non-refugees (464 days) was noted but this was not statistically significant (p = 0.9069). On average, the time to access vision screening was 907 days for refugees and 592 days for non-refugees.
Demographic data are described in the Table 1. Patterns of eye-care utilization are described in the Figure 1.
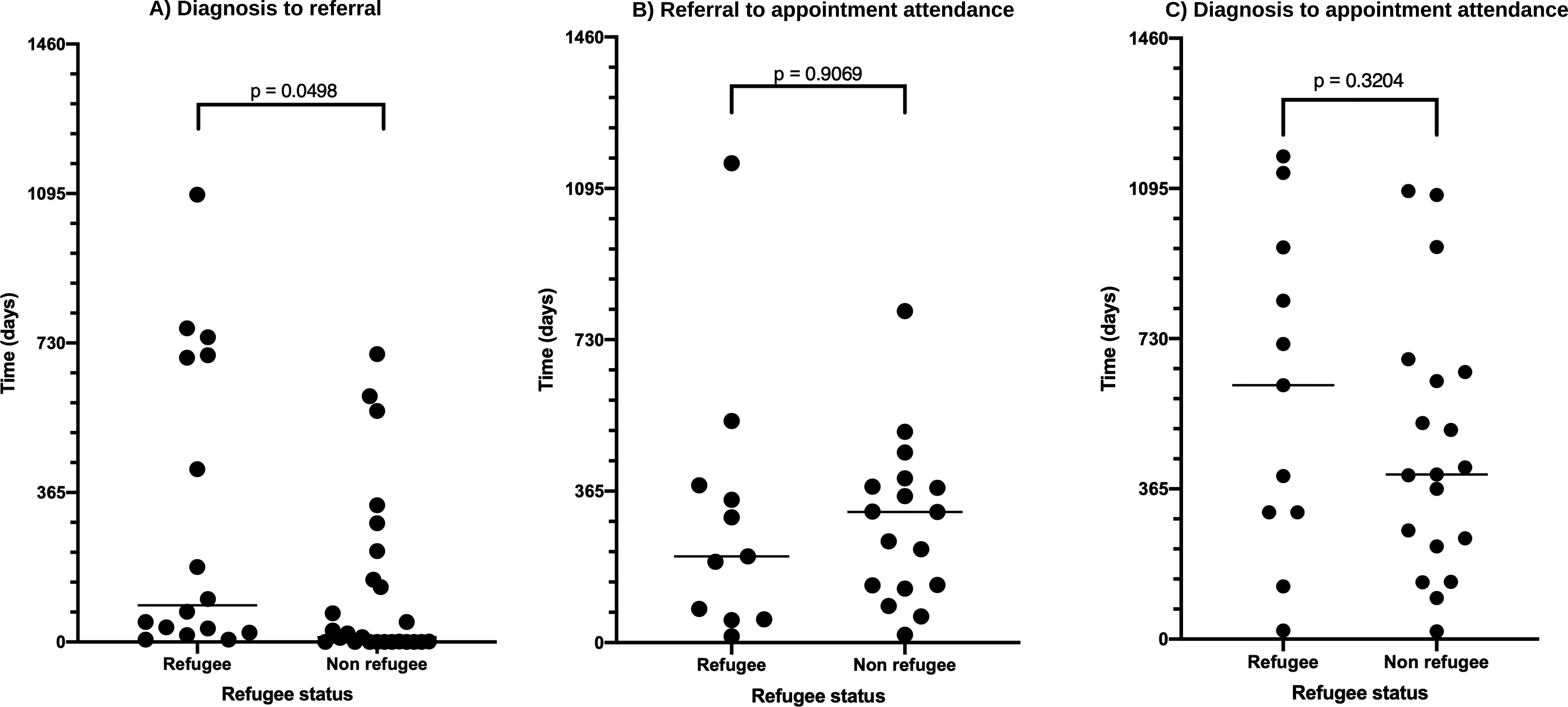
(A) time from diagnosis to referral based on refugee status, (B) time from referral to appointment attendance based on refugee status, (C) time from diagnosis to appointment attendance based on refugee status.
Characteristics of study group.
Discussion
Our findings suggest that refugee patients had a significantly higher rate of referral to an eye-care provider and were more likely to attend their appointment. Additionally, refugee patients were more likely to be evaluated by optometrists rather than ophthalmologists for initial diabetic vision screening. However, the time to access care was longer for refugees than non-refugees, representing potential barriers in eye-care utilization.
Our finding of high eye-care utilization among refugees is aligned with Kiss et al.'s study from a Canadian refugee-focused clinic, which showed higher rates of health services utilization in the primary care setting. 3 Refugee-focused primary care clinics can provide more culturally competent care by utilizing interpreters, engaging with community outreach services for health navigation, and understanding the evidence- and policy-based care guidelines which may be unique to newly arrived refugees. 5 Primary care is essential for delivering preventive health services among refugees, and several studies have demonstrated that providing insurance coverage for primary care services improves utilization. 5 In the context of vision screening, optometry is considered a primary eye care service. Our study demonstrates that refugees had higher eye-care utilization compared to non-refugees, and this may be attributed to routine optometry referral which was facilitated by partial insurance coverage through the IFHP for the first year of arrival to Canada. Bin Yameen et al.'s study of vision impairment in a larger Canadian refugee population found that only 52% of participants were aware of IFHP insurance coverage for vision screening. Of the 800 refugees who participated in their study, which comprised a free vision screening program, none had availed of services insured by the IFHP despite a 12.5% prevalence of vision impairment, which is 13.2 times higher than the non-refugee Canadian population. 9 The discrepancy between eye-care utilization among refugees between Bin Yameen et al.'s study and our findings suggests that routine referral to an eye-care provider may be an effective strategy to improving service utilization.
Principles of culturally competent and community-oriented care among vulnerable populations may be underrepresented in specialist health services, including vision care. Several studies show that specialist services are more challenging to access due to systemic barriers and structural inefficiencies. Fang et al.'s interview-based study of refugees in NL found that experiences with primary care services were generally positive, but access to specialist services was more difficult and often complicated by language barriers, lack of transportation, lack of information regarding insurance coverage, and long wait-times. 2 Kashim et al.'s systematic review on factors affecting non-attendance for diabetic vision screening found that socioeconomic deprivation was a key factor in non-attendance. Conversely, factors which helped to facilitate screening uptake included recommendation from a healthcare provider and knowledge about the importance of screening. 21 Missed appointments are a known byproduct of barriers in navigating the healthcare system and may be a contributory factor in delayed access to care. A testament to this notion may be borne within our finding that refugees experience a significantly longer time from diagnosis to referral and a trend towards longer time from referral to appointment attendance.
Robust settlement service delivery and interprofessional collaboration with eye-care providers are essential to bridging gaps in access to vision care. Bozorgmehr et al.'s study evaluating German health service utilization demonstrated that restrictions in access to care for refugees can translate to increased downstream healthcare costs. 22 The first year of arrival to Canada often presents challenges in navigating a new culture, language, and community; and there may be other active health concerns that warrant more urgent medical attention. These barriers may justify a longer period of insurance coverage for optometric services, which provide represent more efficient health services utilization in the context of T2DM vision screening. In addition, many health navigation programs remain critically underfunded with reports suggesting that insufficient funding may be associated with reduced collaboration across services, thereby limiting the ability to support newly arrived refugees in their economic, social, and health-related wellbeing.2,19,23 Continued support with health navigation services are necessary to ensure that newly arrived refugees are able to access vision screening. Emerging health policy, clinic models, and screening recommendations should reflect these considerations.
Diabetic vision screening is a topic of global public health interest as diabetic retinopathy is a leading—and preventable—cause of blindness. 12 Strengths of our study include that it is the first to explore diabetic vision screening in the Canadian refugee population and takes the form of a retrospective comparative cohort study based out of the primary refugee health clinic in Newfoundland and Labrador—an Atlantic Canadian province with high rates of T2DM 15 and low rates of eye-care utilization. 16 Our study explored the time required to access care as well as the type of eye-care provider accessed, allowing us to preliminarily identify patterns of eye-care utilization.
The small sample size limited our ability to control for variables such as gender and age within subgroup analyses, which are known to be associated with access to healthcare services. However, the study was designed to include every newly arrived refugee with T2DM at the predominant refugee clinic in NL since 2015. This limitation may therefore be an artifact of the nature of forced displacement, as refugees are typically resettled in small numbers across many jurisdictions. NL is a relatively small province and therefore there may be fewer refugees resettled compared to other locations. Additionally, our methodology is privy to detection bias particularly with identifying missed appointments and self-referral to an optometrist. Missed appointments would explain delays in access to care and may reflect difficulties in accessing care or appointment coordination. Self-referral to an optometrist would be theoretically more likely to occur in the non-refugee population as routine vision care is accessible for individuals with private insurance. As such, self-referral would not be captured in this chart review and may contribute in part to the low eye-care utilization seen among non-refugees in our study. Other limitations include selection bias inherent to a retrospective chart review.
Our findings suggest that refugee patients were more likely to access an eye-care provider for T2DM vision screening compared with than non-refugees. The authors hypothesize that the greater eye-care utilization by newly arrived refugees seen in our study may be attributed to routine referral for vision screening and availability of partial insurance coverage for optometric services in the first year of arrival. Despite the increased eye-care utilization, the time to access care was longer for refugees which may represent potential barriers in health services navigation. Future studies should better characterize dynamics of eye-care utilization among a larger refugee cohort as well as the relationship between gender, age, language proficiency, presence of comorbidities, and refugee status (i.e. government assisted refugee versus privately sponsored refugee) on access to screening services.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Memorial University of Newfoundland Summer Undergraduate Research Award.
Supplemental material
Supplemental material for this article is available online.